Malignant transformation of the seminal vesicles is very uncommon. Tumors involving the seminal vesicles are mainly secondary tumors originating from adjacent organs. The tumors that most commonly compromise the seminal vesicles are prostate adenocarcinoma, urothelial carcinoma, and rectal adenocarcinoma [3, 4]. Seminal vesicle metastasis from the transverse colon is very rare, with only two case reports in the literature describing this uncommon pattern of metastasis of primary colon adenocarcinoma [1, 2].
Primary tumors arising in the seminal vesicles are unusual, with adenocarcinoma being the most common form. Given its rarity, diagnosis is delayed and is unlikely to be made at an early stage due to the absence of symptoms, and when patients become symptomatic, it is highly suggestive of advanced disease; symptoms include obstructive uropathy, hematuria, hematospermia, dysuria, painful defecation, or pelvic and perineal pain [5, 6].
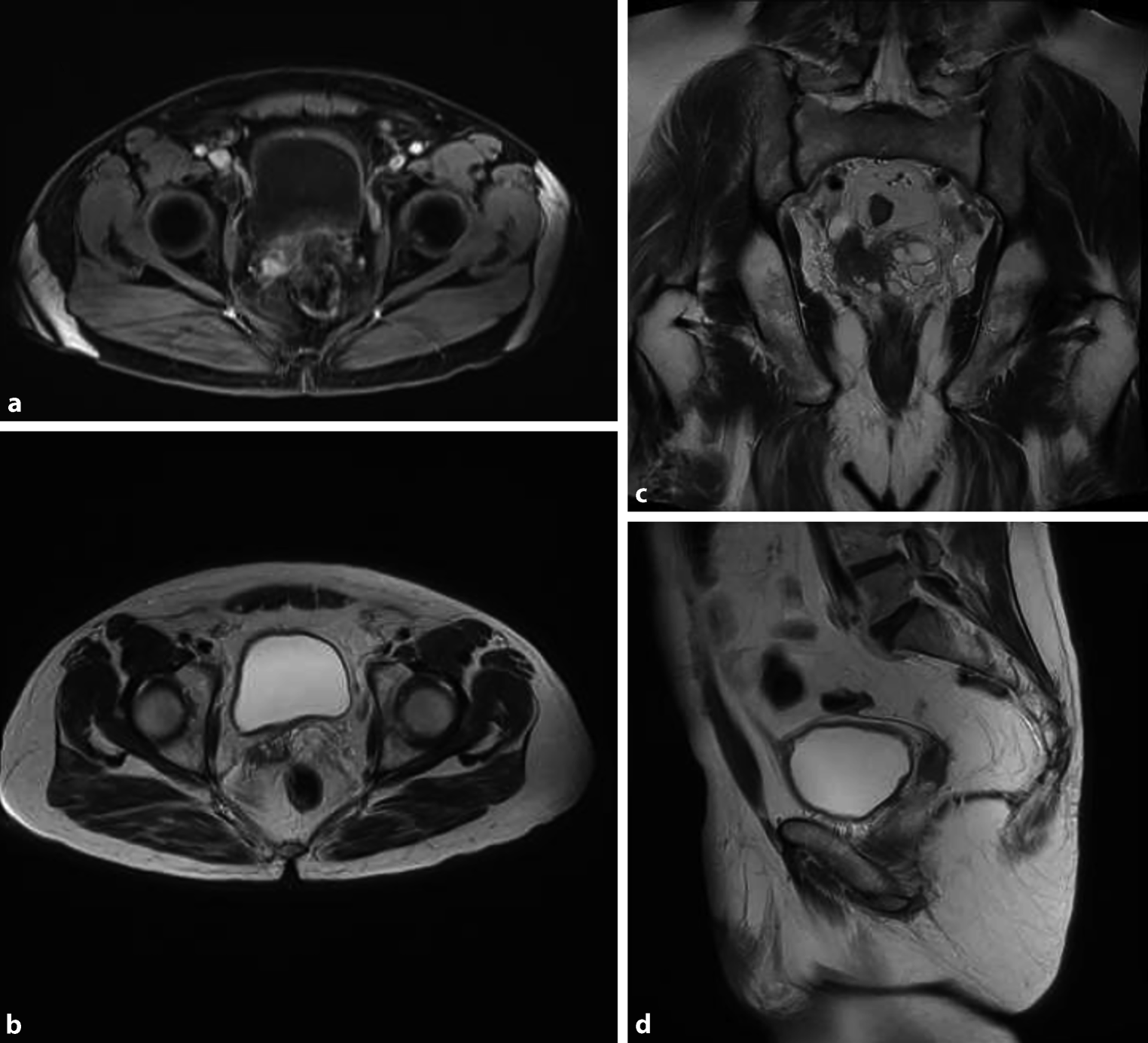
On imaging, some findings suggestive of seminal vesicle tumors include loss of normal seminal vesicle architecture, seminal vesicle enlargement or wall thickening with a low-signal-intensity mass on T2-weighted images, obliteration of the angle between the prostate and seminal vesicles, and appearance of a soft-tissue mass in the retrovesical region with or without prostatic or ureteral obstruction [1, 7].
To date, there are no specific clinical or imaging features in conventional or nuclear imaging that enable the differentiation of a primary from a secondary form of malignancy; thus, an accurate diagnosis remains based on immunohistochemistry [8].
The histological pattern of seminal vesicle adenocarcinoma is defined as moderate-to-poorly differentiated adenocarcinoma with at least focal papillary architecture and tubular structures. The tumor cell cytoplasm may show a clear cell or hobnail morphology. Immunohistochemically, primary seminal vesicle adenocarcinoma is characterized by CK7-positive, CK20-negative, CA-125-positive, PSA/PAP-negative immunophenotypes that distinguish it from other tumors that metastasize to the seminal vesicles (Table 1; [9, 10]).
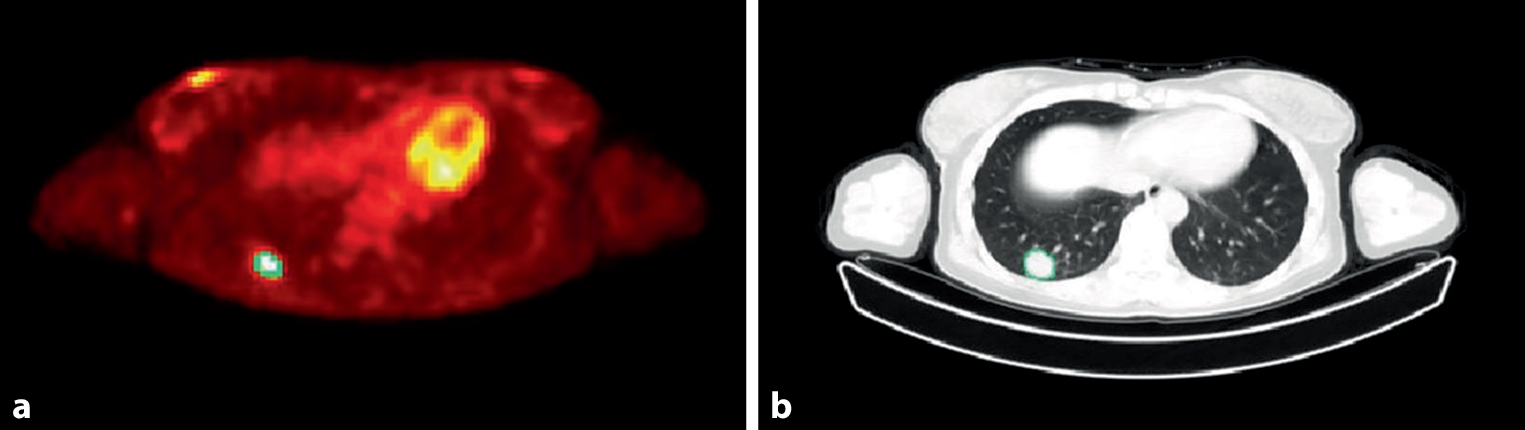
Table 1 Immunophenotypes of tumors that metastasize to the seminal vesiclesaRecently, PET combined with CT has emerged as a powerful tool for the evaluation of many cancers. The radiotracer most commonly used for PET in oncology is 2‑[18F] fluoro-2-deoxy-d-glucose (18F-FDG), a glucose analog that is preferentially taken up and trapped inside metabolic hyperactive tumor cells; hence, areas with increased 18F-FDG intake are suspected to be malignant. However, the use of 18F-FDG in urology is limited because of its physiological excretion through the urinary system; thus, PET imaging is not used as frequently as it is in other medical specialties. 18F-FDG has proven to be accurate, not only for urologic tumors but also for detecting metastatic disease. 18F-FDG is, therefore, commonly used in clinical practice as a diagnostic method during the follow-up of oncology patients with a serologic relapse in which conventional imaging methods do not show conclusive results. No SUV standards have been reported in the literature for seminal vesicle tumors, partly because of the rarity of the condition [11, 12].
Normally, the diagnostic algorithm for primary seminal vesicle carcinoma is the performance of a CT scan upon clinical suspicion, and depending on the results, the mass is biopsied for pathology studies [13]. There is only one case report in which the initial diagnosis was made with 18F-FDG, and described that the radiotracer accumulated only in the seminal vesicles; therefore, the authors argued that 18F-FDG could offer a faster and more accurate preoperative differential diagnosis of a primary tumor from a secondary tumor. For example, differentiating whether the mass of the seminal vesicles is due to invasion from the prostate or originates directly from the seminal vesicles is challenging with CT, but 18F-FDG accumulation solely on seminal vesicles confirms the diagnosis of primary seminal vesicle carcinoma. The advantages of PET/CT over CT as an initial study cannot be established with only one case report [14].
Regarding the diagnosis of seminal vesicle metastasis, it has been reported that the initial study is CT, and if it does not show results that explain the relapse of the oncology patient, PET/CT is performed [15]. In reports in which PET/CT was required during the diagnostic process [3, 4, 14, 16, 17], this technique showed a compromise of the seminal vesicles, as in our case. There are only two reports in which PET/CT was used to diagnose metastasis of seminal vesicles from the colon [3, 4]. To the best of our knowledge, there is no case report of a diagnosis of secondary seminal vesicle adenocarcinoma for which PET/CT was the initial diagnostic test.
With few reports on the use of PET/CT in the diagnosis of seminal vesicle tumors, partly because of the rarity of the disease, this imaging technique seems to have a promising role in detecting metastatic and primary seminal vesicle tumors.
The treatment of seminal vesicle adenocarcinoma usually involves surgical resection of the tumor and chemotherapy [18]. In cases of secondary seminal vesicle adenocarcinoma, the chemotherapeutic regimen is generally based on the primary metastatic tumor, and usually treatment of metastatic colon adenocarcinoma relies on systemic immunotherapy, radiotherapy, or surgical resection. Because in our case the primary tumor was a stage IV colon adenocarcinoma (distant metastasis), a FOLFIRI regimen, leucovorin/5-fluoracil + irinotecan (choosing 5‑fluorouracil) plus a targeted drug, which in our case was the monoclonal antibody against the epidermal growth factor receptor (anti-EGFR) panitumumab, was chosen. In cases of relapse of secondary seminal vesicle adenocarcinoma, which has not been described for metastatic colon adenocarcinoma, management should be based again on the primary metastatic tumor, and thus a regimen of FOLFOX (folinic acid, 5‑fluorouracil, and oxaliplatin) plus IMRT was chosen; however, in our patient it was never started because of infectious compromise [19].
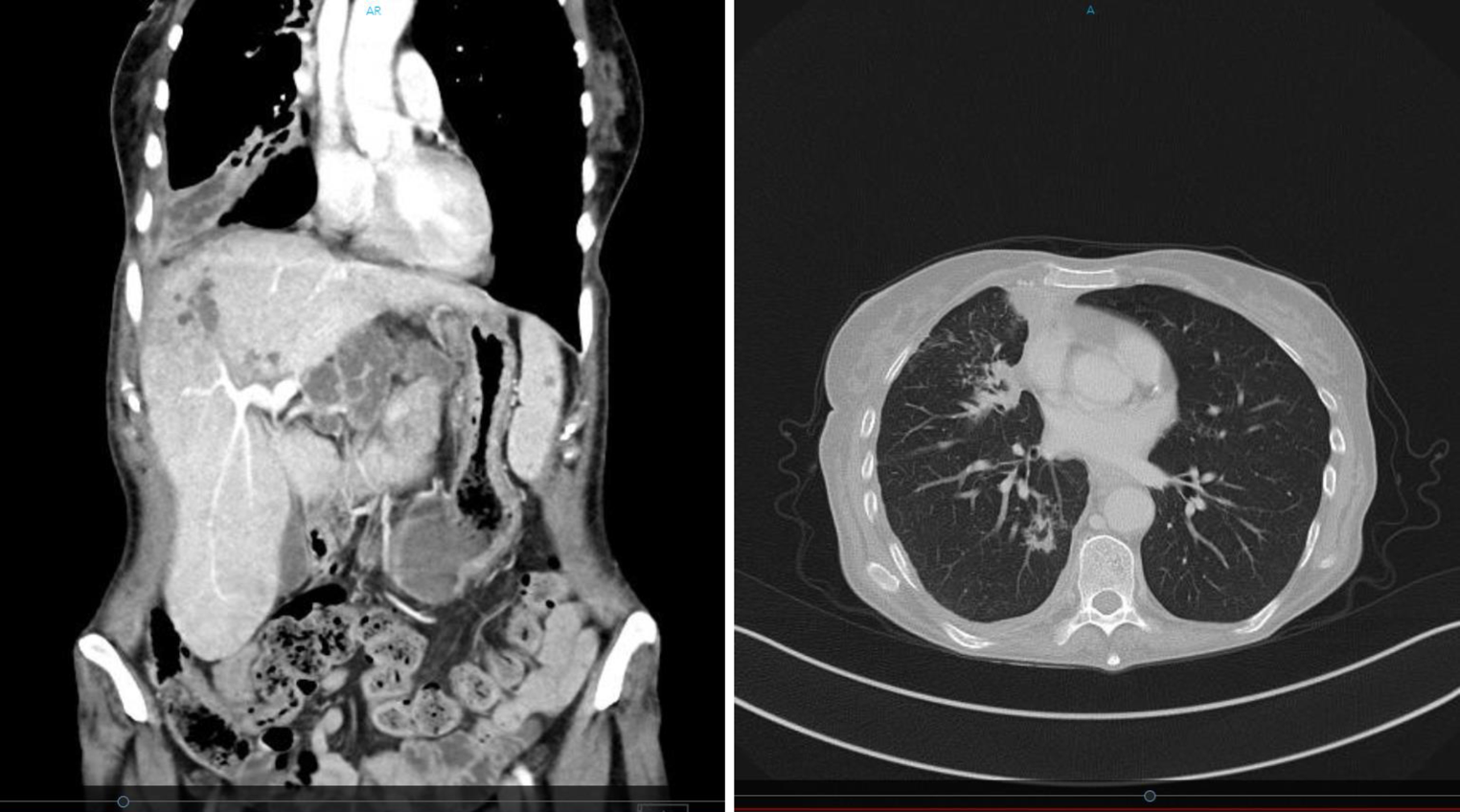
Surgical excision can have a role in treatment if the patient’s metastasis is confined to one site or if it is an oligometastatic disease; furthermore, patient age, life expectancy, and functional status must be taken into account. Laparoscopic excision of the seminal vesicle due to metastatic disease from colon adenocarcinoma has been described in one case report, but the patient only had metastasis to the seminal vesicles. By contrast, surgical excision was not feasible in our patient because he did not have oligometastatic disease (progression to the right seminal vesicle, regional lymph nodes, bone, and lungs), and by the time of relapse, he had a poor functional status [1, 20].
Radiosurgery plays an important role in the management of bone metastases, as in the case of our patient. The primary goal of radiosurgery in bone metastases is to provide effective pain relief and improve quality of life for patients. This is achieved by targeting and destroying tumor cells in the affected bone, thereby reducing tumor burden and relieving pain. In addition to pain relief, radiosurgery can also help prevent fractures and stabilize weakened bones. By delivering high doses of radiation to tumor sites, it can cause tumor shrinkage and promote bone healing. This can be particularly beneficial in cases where bone metastases have compromised the structural integrity of the bone and increased the risk of fractures. Radiosurgery is typically used in conjunction with other treatment approaches, such as surgery or systemic therapies, depending on the individual patient’s needs and the characteristics of the metastatic disease. The use of radiosurgery after chemo-targeted therapy depends on the type and stage of cancer, as well as the patient’s overall health. In some cases, radiosurgery may be used to treat any remaining cancer cells after chemo-targeted therapy. In other cases, it may be used in combination with chemo-targeted therapy to improve the effectiveness of treatment. This may be because the targeted therapy can help sensitize tumor cells to radiation, making them more susceptible to the effects of radiosurgery [21,22,23].
Given that metastasis to the seminal vesicles is rare, standard treatment guidelines are not available; hence, a multidisciplinary team approach is recommended.



留言 (0)