
記住我


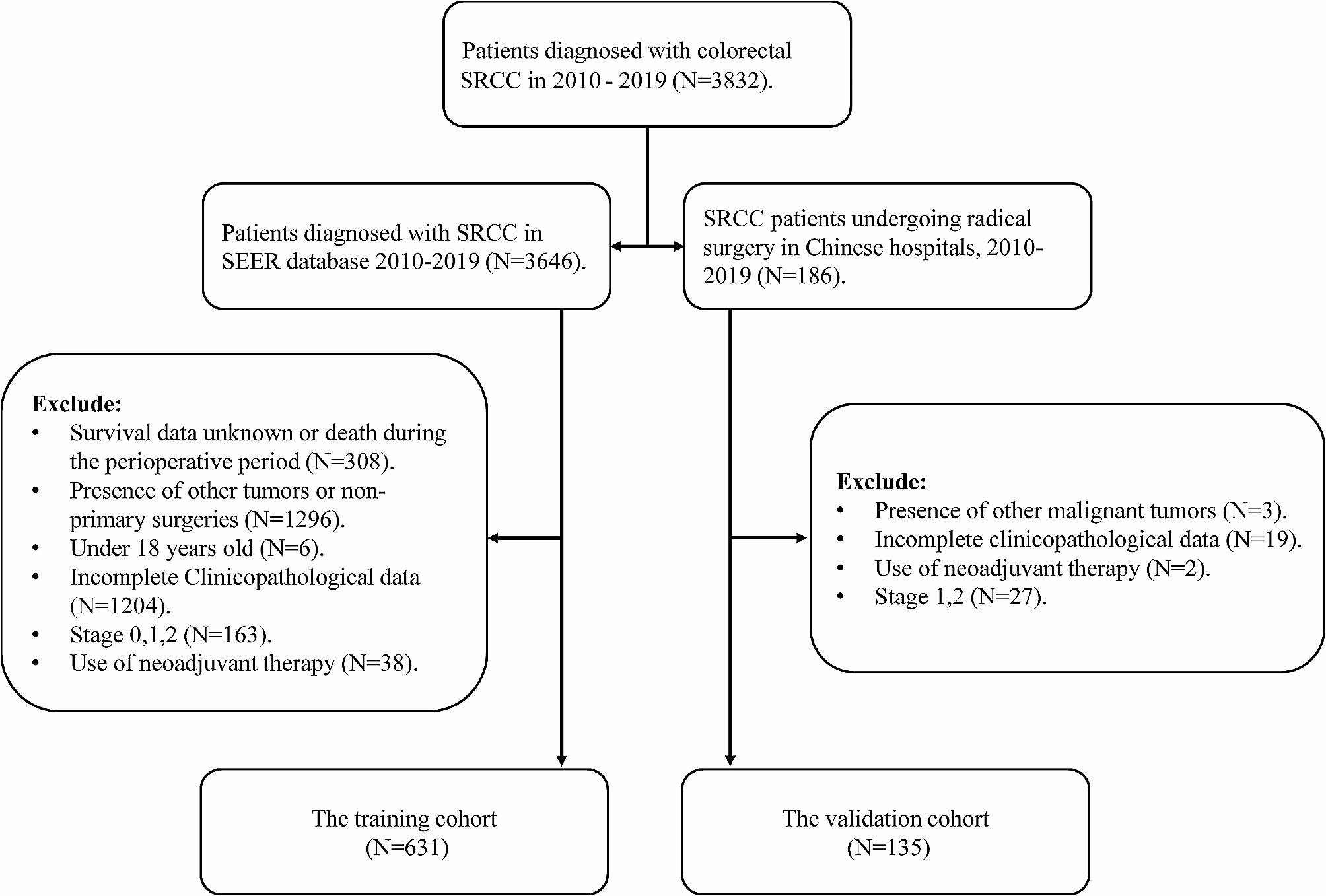



In this retrospective cohort study, we aimed to compare perioperative complications and survival outcomes between patients undergoing LS and OS for HCCA. Between March 2012 to February 2022, our hospital treated 313 patients with HCCA. The data were stored in a specialized hepatobiliary pancreatic tumor database. Initially, 114 patients met our inclusion criteria, but after applying our exclusion criteria, the final study cohort consisted of 68 patients, divided into the LS (n = 40) and OS (n = 28) groups (Fig. 1).
Fig. 1
Case inclusion flowchart for detailing the selection process for HCCA patients in LS and OS groups
Inclusion and exclusion criteriaPatients were included if they were as follows: (1) age ≥ 18 years; (2) had undergone surgical resection of HCCA, including palliative resections; (3) had an Eastern Collaborative Oncology Group (ECOG) score of 0–2; (4) received a postoperative histopathological confirmation of HCCA; (5) had liver function classified as Child-Pugh class B or C; (6) were graded as American Society of Anesthesiologists (ASA) I–III; (7) had complete clinical and follow-up data available; and (8) did not have serious comorbid conditions affecting the heart, lung, brain, or kidney. Tumor staging was performed using the Bismuth-Corlette classification, with particular attention to type IV tumors and any necessity for vascular reconstruction. This Bismuth-Corlette classification has been internationally recognized for the classification of hilar cholangiocarcinoma. In our cohort, patients typically exhibited elevated bilirubin levels due to the obstructive nature of the tumor, leading to their categorization as Child-Pugh class B or C. As a result, no patients with Child-Pugh class A were included in this study.
Exclusion criteria were as follows: (1) pregnancy; (2) intolerance to surgery; (3) neoadjuvant therapy (such as chemotherapy, radiotherapy, immunotherapy, targeted therapy, or other drug treatments) prior to surgery; (4) secondary HCCA; (5) combined surgeries; (6) surgeries not performed at our center; and (7) incomplete clinical data, such as missing visits, incomplete serological reports, and lack of imaging data.
This study is a retrospective cohort analysis wherein the patients were allocated to either the LS or OS group based on the type of completed surgery they underwent. This differs from prospective studies where patients are randomly assigned to specific surgical interventions. The selection for LS was guided by an exhaustive preoperative evaluation and intraoperative exploration, conducted by our multidisciplinary team. This process was underpinned by the specific oncological and anatomical challenges associated with HCCA. Preoperative imaging, including CT, MRCP, CT angiography, or MR angiography, was crucial in assessing the tumor’s relationship with the hepatic artery and portal vein and determining the presence or extent of invasion. Criteria for choosing LS encompassed patients with Bismuth-Corlette types I and II, select cases of type III, and part of type IV tumors, specifically those without portal vein and hepatic artery invasion. Conversely, contraindications for LS, aside from the general contraindications for OS, included inability to tolerate or establish pneumoperitoneum, extensive abdominal adhesions, significant tumor invasion into the portal vein or hepatic arterial trunk, and the presence of regional portal hypertension in the hepatic hilum which could preclude safe radical resection.
We acknowledge the inherent limitations of retrospective analyses, including the potential for selection bias in allocating patients to surgical groups based on completed procedures. To mitigate this, our multidisciplinary team employed stringent criteria based on preoperative imaging and intraoperative findings to guide the decision-making process. During surgery, if the tumor’s characteristics or patient’s anatomy deviated from our preoperative assessments, necessitating a change in the surgical approach, such cases were meticulously documented. This ensured that our comparative analysis between LS and OS groups was as robust as possible within the constraints of a retrospective design.
Ethics and consentAs a retrospective study, informed consent for participation was waived by the Medical Ethics Committee of our hospital, in compliance with ethical standards. The study adhered to the Declaration of Helsinki principles. The relevant data for this study were extracted from patient medical records.
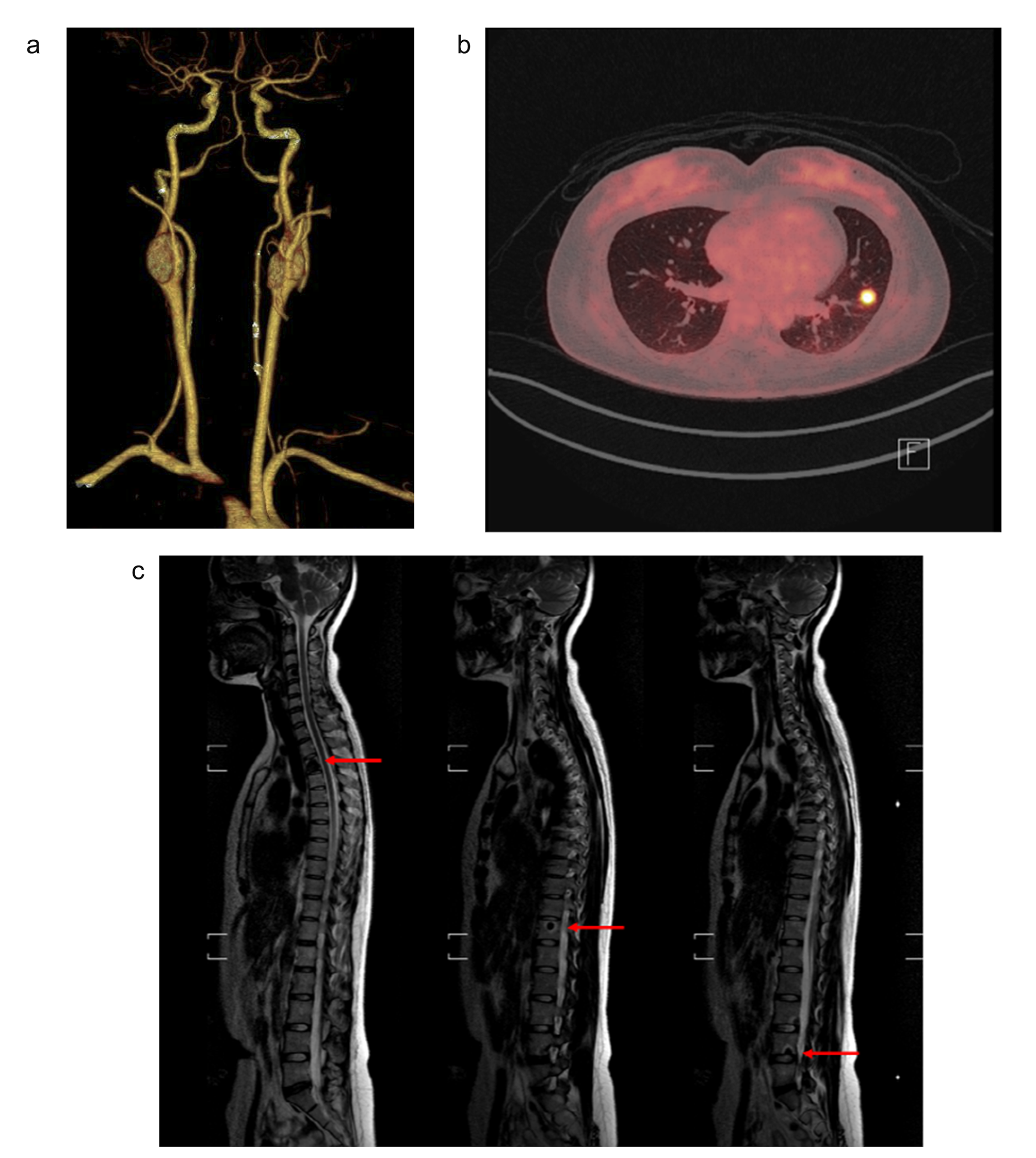
Preoperative preparationAll patients underwent a comprehensive preoperative assessment to assess the characteristics and staging of the tumor. This included contrast-enhanced computed tomography (CT) or magnetic resonance imaging (MRI), as well as magnetic resonance cholangiopancreatography (MRCP) when indicated. Three-dimensional reconstruction was particularly utilized for those with Bismuth-Corlette type IV HCCA to facilitate detailed preoperative planning (Fig. 2). For patients presenting with obstructive jaundice and serum bilirubin levels exceeding 200 μmol/L, or those suffering from cholangitis or at high nutritional risk, percutaneous transhepatic biliary drainage was the preferred method to alleviate jaundice and optimize their condition before surgery. Informed consent for the surgical procedure was obtained from each patient or their family after a thorough discussion of the risks, benefits, and alternatives to the proposed surgical intervention.
Fig. 2
A Location of the tumor on the MRI cross-section. B Coronal MRI showing the shape of the tumor. C MRCP showing the intrahepatic and extrahepatic biliary systems. D Three-dimensional reconstruction showing the relationship between the liver and the biliary system, blood vessels, and tumor. E Frontal three-dimensional reconstruction showing the relationship between the biliary system, blood vessels, and tumor. F Three-dimensional reconstruction of the relationship between the biliary system, blood vessels, and tumor, as shown in lateral view
The Bismuth-Corlette classification was initially estimated through imaging studies; however, it was acknowledged that the definitive classification often necessitates intraoperative assessment due to potential deviations from preoperative imaging predictions. A review of our center’s historical data has indicated a trend towards increased utilization of laparoscopic techniques for HCCA over recent years, which is consistent with the increased incidence of higher Bismuth type tumors in our study cohort. Importantly, the majority of patients were diagnosed at an advanced stage, underscoring the need for meticulous preoperative preparation and evaluation.
Surgical approachLaparoscopic surgeryBefore detailing the technical steps of the laparoscopic approach, it is crucial to outline the indications that led to the selection of LS for treating patients with HCCA. Patients were considered eligible for LS based on a combination of factors including, but not limited to, tumor size and location, the absence of extensive vascular involvement, patient’s physiological status, technical feasibility, and the surgeon’s expertise. The multidisciplinary team, including hepatobiliary surgeons, radiologists, and oncologists, evaluated each case to determine the appropriateness of LS. The decision also took into account the patient’s preference and understanding of the potential risks and benefits after thorough preoperative counseling. These indications align with the intention of providing a minimally invasive approach while ensuring patient safety and the best possible oncological outcomes.
Upon determining eligibility for LS and obtaining informed consent, patients were anesthetized and positioned supine with legs apart. The operating area was disinfected and pneumoperitoneum established. The surgical team’s arrangement was consistent, with the senior surgeon to the patient’s right, the first assistant to the left, and the camera assistant at the patient’s feet. Trocar placement followed a conventional five-port approach for Bismuth-Corlette type IV HCCA as depicted in Figs. 3, 4 and 5 outline the critical steps of the LS, focusing on the radical resection of HCCA, starting from intraoperative assessment to the completion of the anastomosis.
Fig. 3
Distribution of trocar locations in Bismuth-Corlette type IV HCCA surgery
Fig. 4
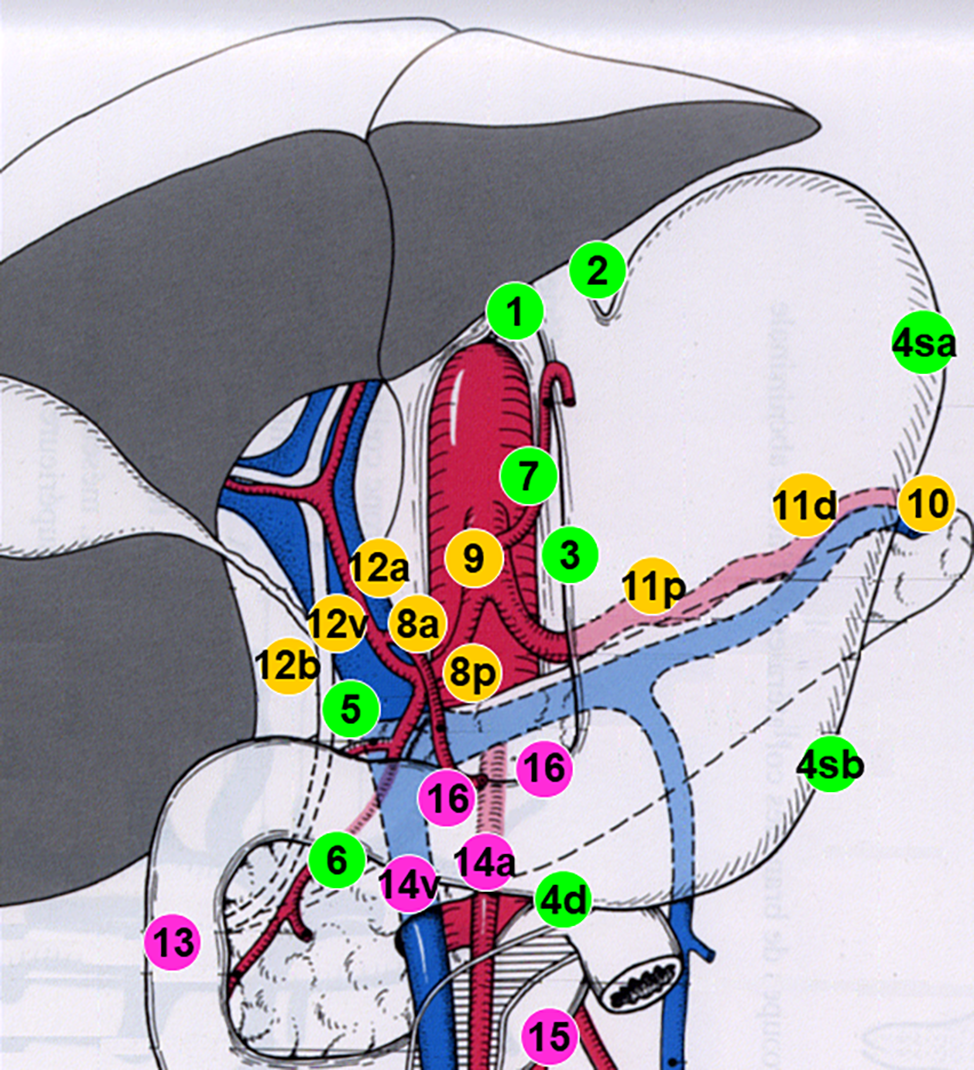
A Intraoperative ultrasound comprehensive exploration to evaluate tumors. B Dissection and separation of the common bile duct (CBD), common hepatic artery (CHA), and gastroduodenal artery (GDA). C Freeing and skeletalizing of the CBD, CHA, and GDA and simultaneous dissection of lymph nodes in groups 8, 12, and 13. D Clamping of the CBD with a Hom-Loc clamp from the upper edge of the pancreas, followed by severing. E Frozen pathological examination of the distal resection margin of the CBD. F Dissection and separation of the right hepatic artery, left hepatic artery (LHA), and portal vein (PV). G Double ligation and transection of the LHA. H Temporary occlusion of the left portal vein (LPV) with a vascular clip. I Observation of change in liver color combined with intraoperative ultrasonography to determine the left hepatic ischemia line. PHA, proper hepatic artery
Fig. 5
A Splitting of the liver and use of a Hom-Loc clip to close the thicker blood vessels. B Dissection and transection of the right hepatic duct (RHD). C Frozen pathological examination of the proximal bile duct margins. D The left portal vein is double-ligated and disengaged. E Hepatic duct-jejunal Roux en-Y anastomosis is performed after bile duct molding. F Sufficient hemostasis on the cut surface of the liver after completion of biliary anastomosis
Open surgeryThe open surgical approach commenced with the creation of a reversed “L”-shaped incision under the right costal margin, extending approximately 25 cm in length. This incision allowed for systematic exploration of the abdominal cavity, proceeding layer by layer. The remaining surgical steps were the same as for laparoscopic surgery.
VariablesIn order to analyze the factors that affect the prognosis of surgery, this study collected general patient data, laboratory findings, perioperative parameters, imaging, and pathological examination results. General data included gender, age, body mass index (BMI), ECOG score, concomitant diseases, and ASA and Child-Pugh classifications. Laboratory test result data collected included the following: preoperative alanine aminotransferase (ALT) level, aspartate aminotransferase (AST) level, alkaline phosphatase (ALP) level, glutamyl transpeptidase (GGT) level, direct bilirubin (DBIL) level, total bilirubin (TBIL) level, albumin (ALB) level, preoperative coagulation function (prothrombin time [PT], prothrombin international normalized ratio [INR], plasma fibrinogen concentration [FIB], and activated partial thromboplastin time [APTT]), carcinoembryonic antigen (CEA), carbohydrate antigen CA19-9 (CA-199), alpha-fetoprotein (AFP), and liver function 1-week post-surgery (ALT, AST, ALP, GGT, ALB, TBIL, and DBIL). Perioperative parameters included the following: preoperative nutritional support, preoperative biliary drainage, intraoperative blood loss, intraoperative blood transfusion, Bismuth classification, vascular invasion, liver resection, intraoperative presence or absence of hilar blockade, surgical margin status (R0, R1, or R2), operation time, and postoperative complications (liver failure, bile leakage, acute respiratory distress syndrome, abdominal infection, intra-abdominal hemorrhage, and disseminated intravascular coagulation), with or without postoperative blood transfusion, postoperative hospital stay time, and total hospitalization expenses (from admission to discharge). Imaging and pathological findings included the following: histopathological report, abdominal enhanced CT, abdominal ultrasound (US), MRI, and MRCP.
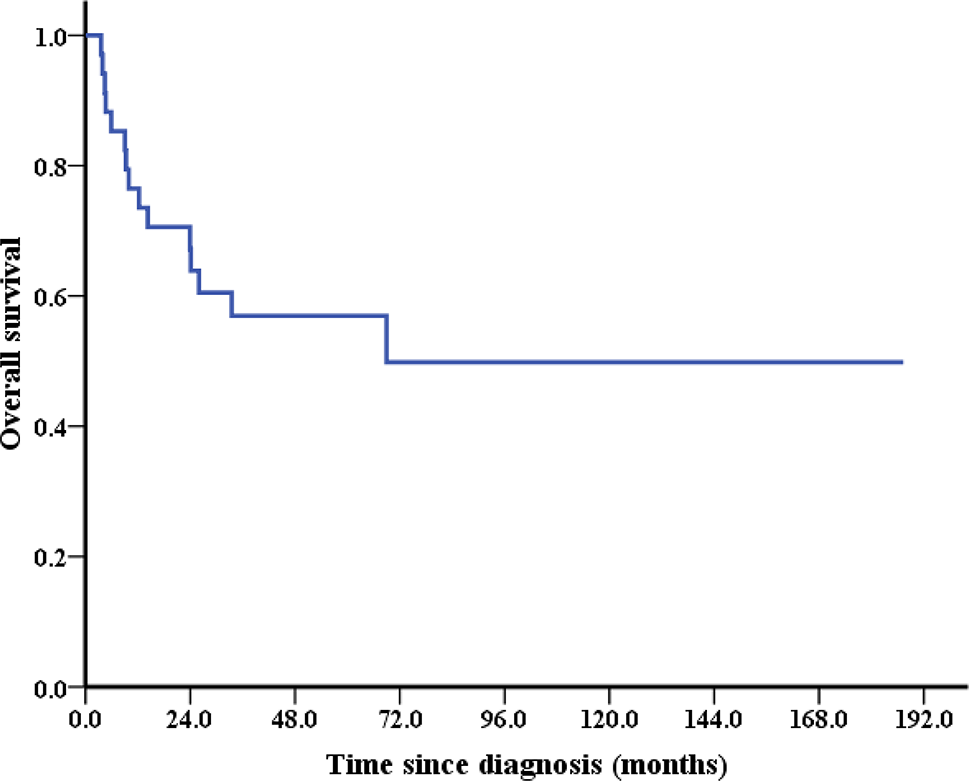
Endpoints and assessmentsOverall survival was defined as the period from the date the patient underwent surgical resection of HCCA to the end of follow-up or date of death. Disease-free survival (DFS) was defined as the time from the date of surgical resection of HCCA to the date of diagnosis of tumor recurrence or the end of follow-up or date of death. In addition, patients were followed up by telephone and outpatient services. According to Clavien-Dindo classification, postoperative complications were classified as grades I, II, III, or IV [11, 12]. Short-term outcomes were evaluated based on postoperative complication rate and mortality within 90 days. Long-term outcome was tumor recurrence or death after 90 days.
Statistical analysisContinuous variables are expressed as mean ± standard deviation (SD) or median (range), and the significance of differences between groups was assessed using the Student’s t-test or Mann-Whitney U-test, respectively. Categorical variables are expressed as frequencies and percentages, and differences between groups were analyzed using Fisher’s exact test or the χ2 test. Survival was analyzed using the Kaplan-Meier method, with differences evaluated using the log-rank test.
In our study, addressing the crucial aspect of sample size adequacy was paramount, particularly given the unique challenges in accruing large cohorts for HCCA surgery. We performed a rigorous power analysis using PASS software, specifically focused on the median survival outcomes shown from our survival time curves. This analysis yielded a power value of 0.76. We acknowledge that this figure is slightly below the standard threshold of 0.8. However, considering the specific context of HCCA surgery — a field where patient eligibility for either LS or OS is inherently limited due to the complex nature of the disease and technical demands of the procedures — this power value represents a reasonable level of statistical robustness. It indicates our study’s ability to detect significant differences in survival outcomes between the LS and OS groups, despite the challenges in patient recruitment. Our study cohort, encompassing 68 patients from a single center over a decade, represents one of the larger cohorts in this specialized field, as outlined in our “Introduction” and “Discussion”. This cohort size, while smaller than those in more prevalent conditions, is substantial given the rarity and surgical complexity of HCCA.
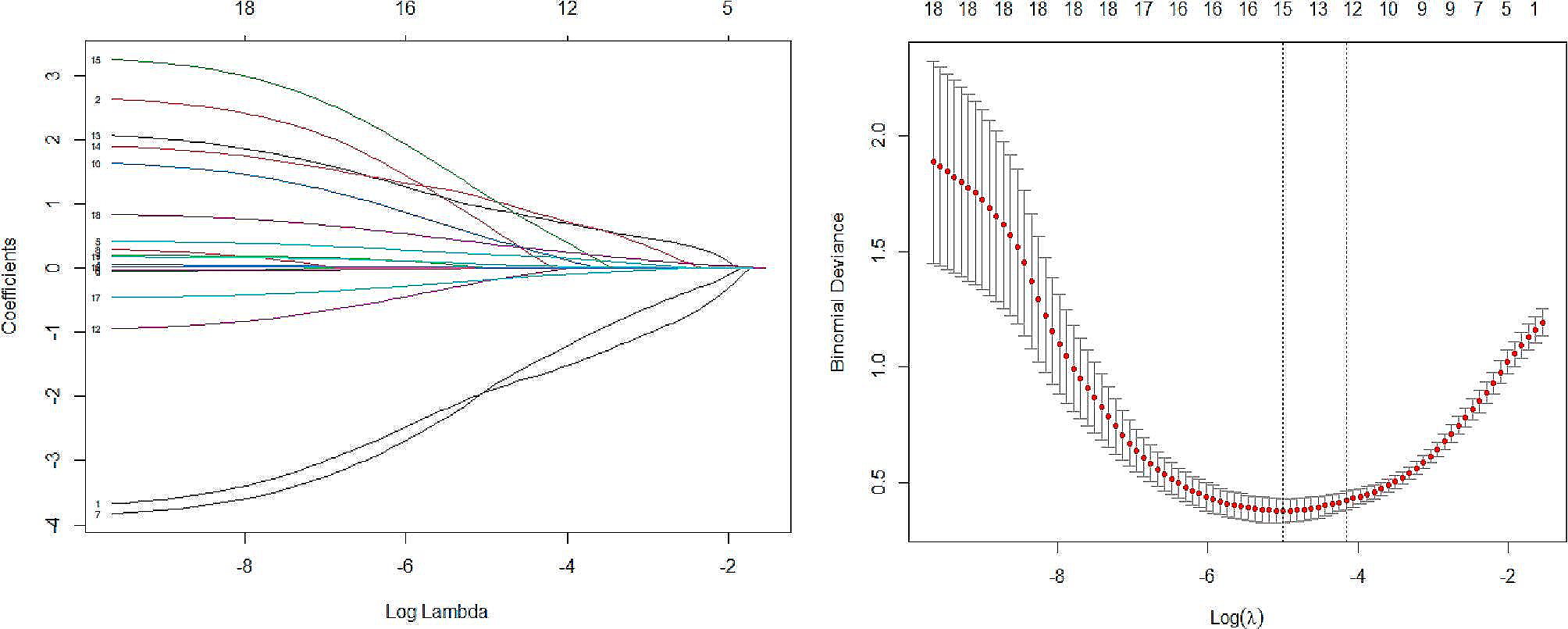
Univariate and multivariate analyses of overall survival and DFS were performed using the Cox proportional hazard model (variables with a combination of clinical expertise and P < 0.20 in the univariate Cox proportional hazards analysis were incorporated into the multivariate Cox proportional hazards analysis). Three-dimensional reconstruction used SYNAPSE 3D (Fujifilm Medical Co., Ltd., Tokyo, Japan). All statistical analyses were performed using R Studio software (version 1.3.1093) and IBM SPSS software (version 23.0). P < 0.05 indicated a statistically significant difference.
留言 (0)