
記住我


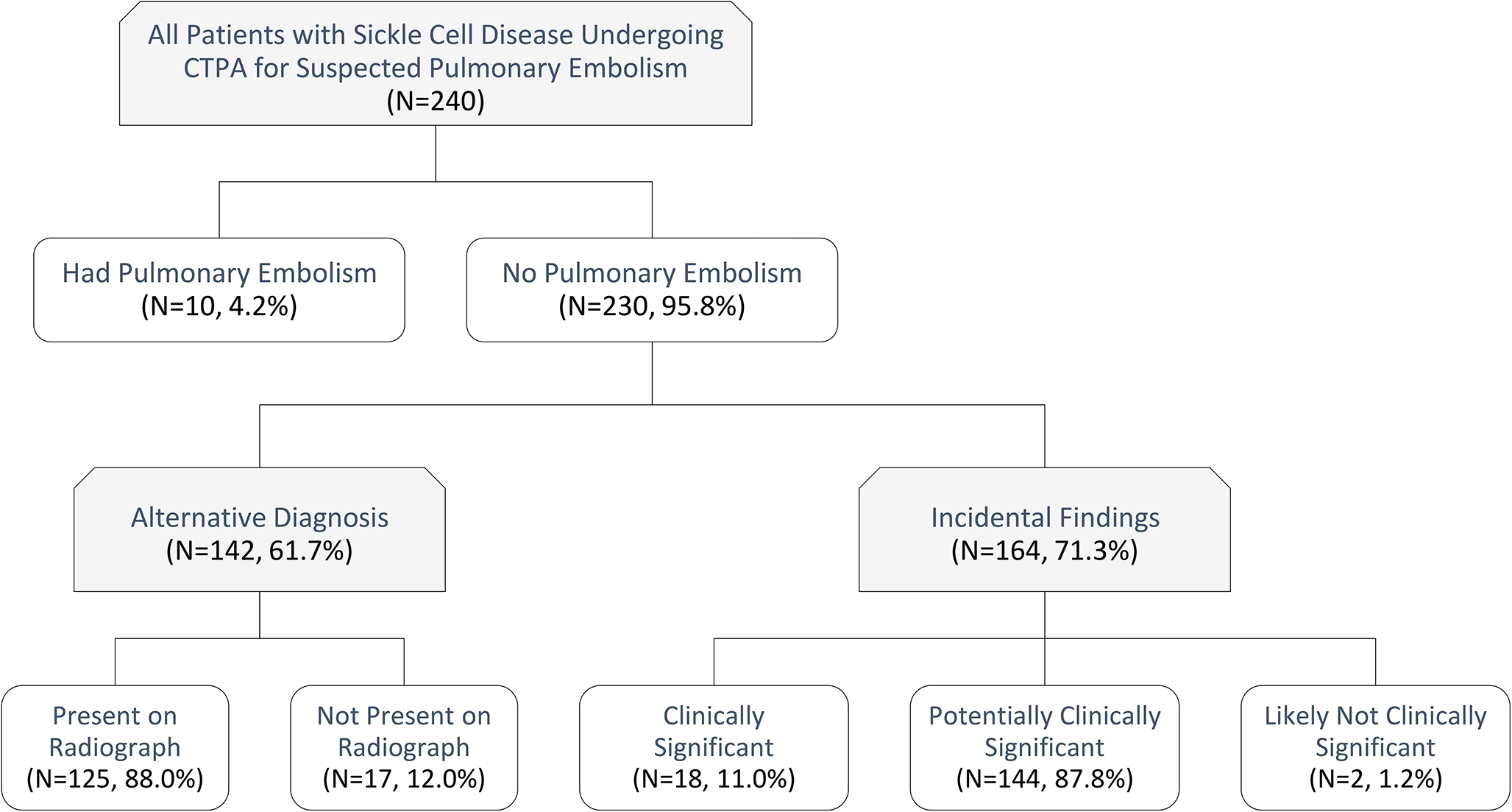

A total of 262 trauma patients admitted between June 2014 and September 2021 with bowel and/or mesenteric injuries were identified in our institution’s trauma registry which consisted of 12,336 patients admitted to or consulted by our trauma service. Exclusions included one pediatric patient, 92 patients who lacked an admission abdominal CT scan, and seven patients who expired in hospital without laparotomy, leaving a total of 162 patients in our cohort. These seven patients all underwent palliative care for severe traumatic brain injury.
The 162 patients in our cohort were on average 40.9 ± 17.6 years of age, the majority male (69.1%) and White (54.9%) (Table 2). The most common mechanism of injury was motor vehicle crash (81.5%) with 65.4% of patients having an ISS of 16 or greater. Overall median length of stay was 7 (4 – 13) days. Seventy-two patients underwent laparotomy and 43 (59.7%) had sBMI, leaving 29 (40.3%) who underwent non-therapeutic surgery. The average length of stay for these patients was 9.5(5.0 – 15.5) days. 90 patients did not undergo laparotomy and had a median length of stay of 5.5(3.0 – 12.0) days.
Table 2 Patient and injury characteristicsEach BIPS and RAPTOR scoring feature is listed in Table 3 with the corresponding count and percentage present with and without sBMI. The presence of two of the three BIPS criteria (abdominal tenderness and CT grade > 3) was more prevalent in the group with sBMI (60.5% vs 34.5%, P =.003 and 65.1% vs 18.5%, P < .001). WBC > 17 g/l did not discriminate between patients with or without sBMI (P = 0.670). Five of the 7 RAPTOR criteria (multifocal hematoma, acute arterial extravasation, bowel wall hematoma, pneumoperitoneum, and fat pad injury) were more prevalent in sBMI groups (Table 3).
Table 3 Comparison of BIPS and RAPTOR score features with bowel and/or mesenteric injuryThe distribution of BIPS, RAPTOR, and radiologist impression scores is shown in Table 4. Seventy-five percent of scores were either 0 or 1 for all three scales. 3.7%, 1.2%, and 14.2% of cases were categorized as the most severe score by BIPS, RAPTOR, and radiologist impression. As shown in Table 4, radiologist impression was no or unlikely sBMI on 99 of the 162 scans. However, 7 (7.1%) of these patients had sBMI as confirmed by laparotomy. Sixteen (40%) of the 40 scans determined by radiologists to have a possible sBMI were confirmed by laparotomy, and 20 (87%) of the high-likelihood cases had sBMI confirmed by laparotomy.
Table 4 Distribution of BIPS, RAPTOR, and radiologist impressionFigure 1 demonstrates a patient with a suspected high likelihood of injury via radiology impression (score = 2) and BIPS (BIPS CT Grade = 5), but a low likelihood on RAPTOR (score = 1). This patient had a confirmed small bowel injury. Figure 2 demonstrates a mesenteric contusion with active bleeding and had a BIPS score of 5 and a RAPTOR score of 2 and a radiologist impression score of 0. This patient did not have a confirmed bowel injury. Examples of radiologic findings of patients with confirmed bowel injuries are shown in Fig. 3.
Fig. 1
Sagittal CT in lung window demonstrates a large amount of free air (red arrow). There were no other signs of bowel injury according to the RAPTOR grading; however, the patient was confirmed to have an injury of the distal ileum. This was graded as a 2 given the large volume of free air
Fig. 2
(Left) Coronal CT of the abdomen demonstrates a small mesenteric contusion (red arrow). (Right) Axial CT shows the mesenteric contusion with a small focus of active extravasation (yellow arrow). This patient had no bowel injury upon exploratory laparotomy
Fig. 3
(Left) Coronal CT of the abdomen showing a collection of free air and fluid adjacent to a small bowel loop (red arrow). (Center) Coronal CT of the abdomen in a different patient showing bowel wall thickening with interloop fluid collection (white circle). (Right) Coronal CT of the abdomen in a different patient showing a devascularized bowel (yellow arrow)
Sensitivity and specificity with the area under the curve are shown in Fig. 4. BIPS and RAPTOR were highly specific (86.6% and 82.4%) but not sensitive (48.8% and 46.5%) with AUCs of 0.75 and 0.72 (Fig. 4, left). Radiologist impression exceeded the sensitivity of the others at 81.4% with only a slight drop in specificity (71.4%) and the overall highest AUC of 0.82. There was not a significant difference between BIPS and RAPTOR AUCs (P = 0.55). Radiologist impression was the superior discriminator of sBMI when compared to RAPTOR (P = 0.04) but not BIPS (P = 0.13).
Fig. 4
Receiver operating characteristic curves for BIPS, RAPTOR, and radiologist impression in predicting blunt bowel and/or mesenteric injury. Abbreviations: AUC, area under the curve; BIPS, Bowel Injury Prediction Score; CI, confidence interval; CT, computed tomography; RAPTOR, radiographic predictors of therapeutic intervention
Thus far, the AUCs presented are based on the continuous score of BIPS, RAPTOR, and radiologist impression. The creators of the BIPS and RAPTOR scores determined that threshold scores of 2 and 3 for BIPS and RAPTOR respectively most accurately predict sBMI. In this study, 25% (40/162) of radiologist impressions were categorized as possible sBMI, and 40% of these were found to have sBMI. Thus, we grouped the possible sBMI and high likelihood sBMI cases together and repeated our analysis using the dichotomous scale (i.e., score of zero vs. ≥ 1). Thresholds of > 3 for RAPTOR and >2 for BIPS were used for this analysis. As expected, the AUCs for each measure dropped; however, radiologist impression remained associated with the highest AUC (0.76) followed by BIPS (0.68) and then RAPTOR (0.64) (Fig. 4, right).
留言 (0)