The fiscal projections presented across three countries demonstrate that patients with HER2-positive eBC with residual invasive disease experience more work losses compared with the healthy population, resulting in projected lower taxes paid over remaining working years. The fiscal results presented here are also compared with more traditional outcomes of societal perspectives using productivity losses. Overall, the patients with HER2+ eBC are projected to have a considerable negative impact on the governmental net fiscal balance as well as considerable productivity losses to society when compared with a healthy population. To the government, only part of the societal productivity losses will be directly attributable to the government’s fiscal accounts (e.g., income tax). Unlike the societal perspective, the fiscal perspective presented here captures those costs that typically fall directly on governments. The model indicates that reducing the proportion of women who develop recurrences and metastasis will have positive impact on the fiscal balance, as it will increase the number of LYs lived and the number of productive life years lived.
The results are presented in the original currency, as it is not feasible to compare costs across countries. This is because employment activity rates and social benefit programs, which influence fiscal costs, are different across countries. Consequently, there are likely to be variations in tax losses and transfer costs observed across different countries, which is evident in our work. Furthermore, the underlying disease modeling considers no differences in treatment efficacy across countries, which could, in theory, influence fiscal projections in each country. The sick leave costs reported here are caused by patients with residual invasive eBC discontinuing work while receiving treatment, although the fiscal losses are a small proportion of lifetime taxes paid over their remaining lifetime. The reality is that many survivors return to work, which has been reported at around 43–93%, although there is considerable variation across countries that is further impacted by sociodemographic and clinical factors [31]. In addition, the amount of taxes paid by partners as caregivers is also reduced, although there is notable variation across countries. Comparing rows (b) and (c) in Table3 indicates that reduced taxes for patient and caregiver are comparable in Canada and Portugal; however, caregiver tax losses equate to a smaller proportion in Brazil. While we believe our approach is generalizable to other countries, it is important to recognize that the magnitude of effect will vary depending on cultural and policy factors rather than clinical outcomes.
Previous studies have documented the indirect societal losses attributable to breast cancer owing to reduced work activity [32]. The analysis described here has applied a different perspective by estimating how breast cancer imposes fiscal gains and losses for government applying a “government perspective” framework. A previous study in Europe has used top-down prevalence-based modeling approach to estimate public revenue losses in a single year attributed to breast cancer in Poland. The authors report tax losses of €211 million in a single year in which social insurance contributions and value added taxes (VAT) were the main revenue losses from breast cancer [33]. These results are not directly comparable to our findings, which use a bottom-up cohort modeling approach and projects costs over subsequent years. Nonetheless, the results described by Łyszczarz and Nojszewska illustrate the magnitude of the aggregate effects felt by government in relation to breast cancer in a single year.
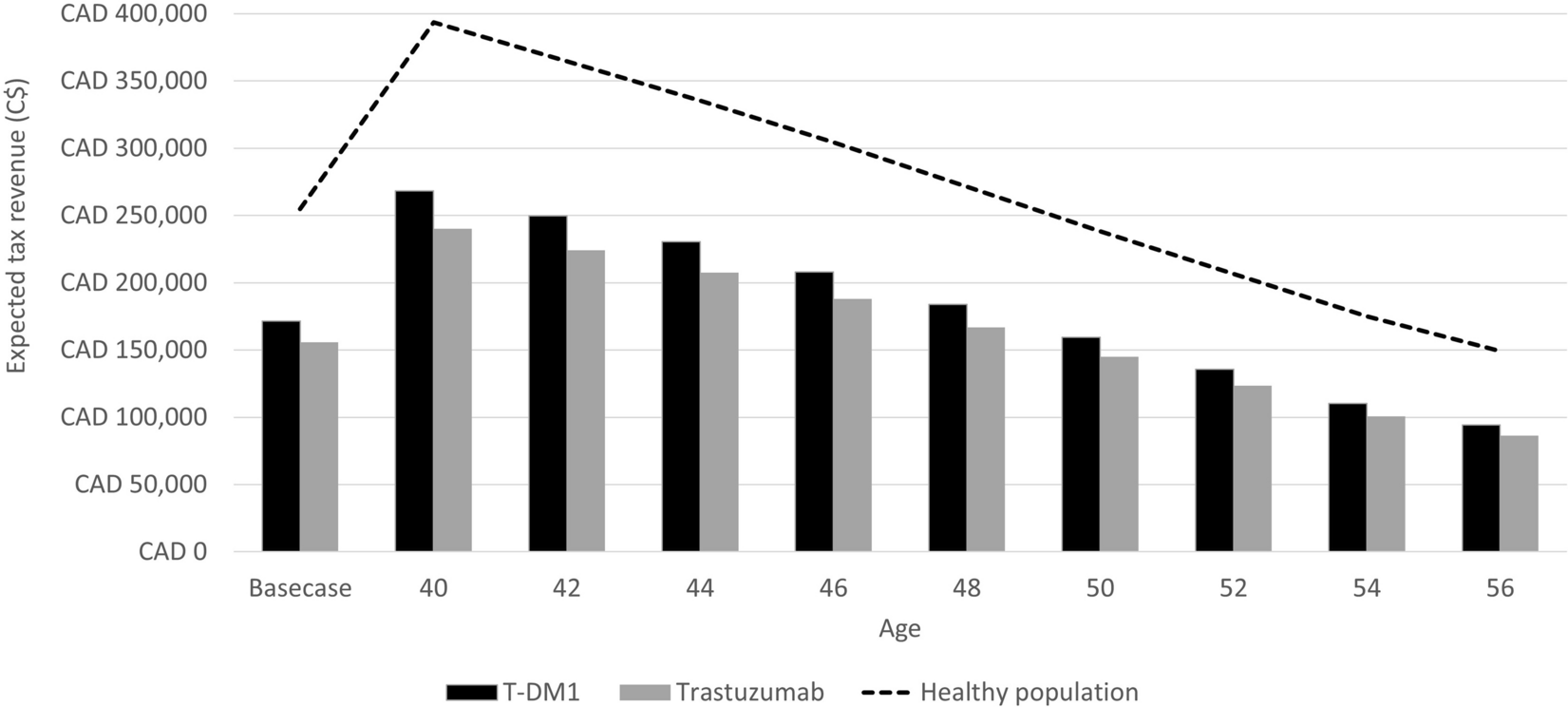
The analysis described here helps to illustrate how cancer recurrence, such as eBC, can impact government tax revenue and social benefit costs. Despite advances achieved with the addition of 1 year of trastuzumab to standard (neo and adjuvant) chemotherapy in the treatment of patients with HER2-positive eBC, it is estimated that up to one in four patients will experience recurrence within 10–11 years of diagnosis [34, 35]. Since metastatic disease is currently incurable, improving the results of initial therapy, when the disease is still without distant metastases, offers the best chance of cure. For patients who are not cured, improved initial therapy may also lead to meaningful delays in disease recurrence and death. The results described in our analysis illustrate the likely fiscal gains from preventing disease recurrence in patients with residual invasive disease after neoadjuvant therapy. By comparing gross tax revenue for T-DM1 and trastuzumab in Table 3, we can see the likely fiscal benefits for governments from reducing the proportion of women with recurrences. The analysis here was informed by a study illustrating that 83% of women in Canada with recurrence will experience work loss during the treatment period [29]. For women in the metastatic health state, we apply the observation that only 35% of women continue to work during the metastatic period [30]. Both of these elements were used to adjust the work activity rate by age for women on which the fiscal projections are based. These findings suggest that new treatment options that reduce the risk of recurrence are still required for patients with HER2-positive eBC, and particularly those with high risk of recurrence that are likely to generate fiscal returns.
Women experiencing BC face a wide range of choices that can influence their household finances. While many will discontinue labor force activity during the treatment period, a considerable proportion of them will return to full-time work, while others will elect not to return to work and may consider part-time employment or permanently retire. A wide range of factors can influence these choices depending on their labor market skills, stage at diagnosis, intervention type, and a range of sociodemographic variables [36]. These employment choices not only impact households but, in turn, have consequences for governments owing to reduced tax revenue and likely increased expenditure on public benefits. While these patients have a perfectly legitimate claim for these benefits, society is better off when every person is able to work and contribute. This is most evident in BC, which impacts women in the prime of their working careers, where earnings are highest. We believe the work described here helps to illustrate the importance of “return to work” as an important outcome in cancer care, as this often signals defeat of one’s health condition and a return to normalcy. Importantly, the fiscal value applied to returning to work described here is likely to be undervalued when taking into consideration the role that work status can have on mental health in cancer survivors [37].
Advancing age with fewer workers represents a fiscal challenge for governments. As the remaining number of working years declines, ageing patients start to draw more from public programs, which are, in turn, funded by the less populous body of workers. The challenge of intergenerational fiscal transfers between citizens in different age groups has been widely researched in the literature of public economics [38]. However, as shown here, the consequences are even more dramatic when patients experience chronic and acute events, such as residual invasive eBC, which prevents them from reaching the employment levels of the healthy population norm (Table 1). To a large extent this is also influenced by age at diagnosis. This study highlights that patients diagnosed in earlier years represent a greater fiscal loss for governments; however, curative treatments that improve survival may lead to fiscal benefits for governments.
Age at diagnosis and treatment are important components that have fiscal consequences for governments. From a policy perspective, early detection and treatment without recurrence offers the greatest fiscal gain for governments, as this enables workers to be productive over the normal life course. Diagnosis at later age has less impact, as patients have fewer working years remaining and the option for early retirement might exist. The analysis described here focused on women with HER2-positive eBC with residual invasive disease, where a rich body of evidence has explored the relationship between treatment, recovery, and wages in this population. In practice, the fiscal framework could be applied to any cancer or health condition that influences choices patients are likely to make regarding labor market activity. Applying this approach to HER2+ residual invasive eBC is a good example to investigate, as it can afflict relatively young women for whom the prognosis is good, hence who are more likely to return to work. The methodology and results described in this study may also help inform some of the fiscal benefits that can be expected among other cancer treatments; however, applying this approach to cancers that are diagnosed, on average in older ages, would likely yield different results.
Improved cancer survival creates future expenditure for governments in relation to numbers of pension payment recipients. Here we report both pension costs likely to occur prior to normal retirement age and all pension costs for projected remaining life years. Pension costs that arise pre-retirement age represent those patients opting for early retirement or some form of permanent transition out of work and the associated costs paid by government. These costs were small in relation to all other pension costs for the three countries explored. These cost comparisons are presented in Table 3 columns (I) and (e). However, these fiscal projects are likely conservative because remaining working years and increased economic activity generate additional economic gains for society that are not accounted for here.
Fiscal projections are often produced and used by governments and central banks to assess the cross-sectorial impact on public accounts of policy changes and the introduction of new programs. When evaluating health programs, the most common perspective is that of the health service applying a welfarist approach for assessing value in an effort to achieve technical efficiency using cost-effectiveness analysis. From a public economic viewpoint, the health service perspective can be viewed as shortsighted, especially in tax-financed health systems, as it does not take a broader systems approach to understand how spending in health and outcomes achieved influences other government sectors, e.g., tax revenue and transfers. At the margin, every health event avoided, case cured, and death averted or delayed has both positive and negative fiscal consequences for governments. This is most evident in patients with remaining working years, as they will continue to work and pay taxes and help to sustain the system for someone who is more in need than they might be. Every working-aged person out of the work force must be paid for by those remaining workers. The fiscal approach applied here is essentially a fiscal cost–benefit analysis that is already used by governments for informing resource allocation decisions [39]. For cancer survivors, the costs of curative treatment apply over a short period of time; however, the fiscal consequences of labor market choices that follow have sustained effects over long time horizons. We are advocating that the fiscal framework explained here should be adopted to evaluate some technologies alongside more traditional approaches to health technology assessments to inform decision-makers about fiscal sustainability.
Model Limitations
There are several limitations to the modeling work described here that are worth taking into consideration. Firstly, a limited number of studies were identified that describe the relative measure of effect associated with eBC recurrence and especially how invasive disease impacts employment in each country. Whilst our search identified several useful studies for Canada, we were unable to find comparable data on employment transitions for eBC health states in Portugal and Brazil. In the absence of local data, we applied the risk ratios for Canada on employment to these markets, which may over or underestimate the likely impact on employment and consequently the fiscal impact. We have explored how changes to these parameters may influence the net fiscal balance in each country and observed that no change influenced the findings by more than 10%. The choice made by women whether they return to work following treatment is governed by financial and cultural factors and the availability to access income support programs in each country. While this may be less of an issue in Portugal with a universal welfare system as found in Canada, these job transitions and the need to return to work may be less applicable in Brazil. A second limitation is that our analysis does not include healthcare costs for treating eBC with residual invasive disease and for future non-related health costs. This suggests that what we are showing here is only a segment of the costs that fall on governments. Another limitation in our analysis is the extrapolation of employment data over long periods of time. This limitation is common to all fiscal projections owing to lack of visibility over future work environments and likelihood for retirement policy changes. This does not make our analysis incomplete; rather, it suggests our work highlights a different range of costs. This work is not designed as a cost-effectiveness analysis, although it does use the engine from a previously described economic model that has been compared with the healthy population in each country [27]. It is also important to recognize that our analysis is limited to its consequences on governments. We do not consider the impact on household savings rates, which provide wealth in later years and associated taxes derived from investments or impact of additional private healthcare coverage. Similarly, our approach fails to take into consideration the interaction between different economic domains, which can give rise to growth attributed to economic multipliers [40]. As our approach is simply an accounting framework, there are likely to be broader economic gains from changes in health status that are not reflected here. Furthermore, our analysis does not capture many non-labor related activities that add value to society, such as caring for grandchildren or volunteering.


留言 (0)