Based on the predefined inclusion and exclusion criteria, a total of 31 patients with recurrent presacral tumors who underwent surgical treatment between June 2009 and November 2018 were ultimately enrolled in this study. All patients had previously undergone surgery for presacral tumors at other institutions and presented to our hospital with recurrent presacral tumors. Among the patients, there were 22 females and 9 males, resulting in a female-to-male ratio of 2.4:1. The mean age of the enrolled patients was 36.77 ± 11.17 years (range, 20–61 years). The diameter of the presacral tumors ranged from 5 to 21 cm, with a median measurement of 11 (IQR = 7) cm. The patient demographics and clinical data have been recorded in Table 1.
Table 1 Demographic and clinical data of the studySymptoms
Among a total of 31 patients, 2.3% (n = 10) of the patients were asymptomatic, and the rest of the patients (67.7%, n = 21) were symptomatic (Table 2). Among the symptomatic patients, sacral caudal pain was reported as the most prevalent complaint by 7 individuals.
Table 2 Symptoms observed in the studySurgical data
Twenty-seven patients underwent surgery using the posterior approach, while 1 patient underwent surgery via the anterior approach (transabdominal excision), and 3 patients received the combined surgical approach involving both posterior and anterior approaches. During the surgical procedures, coccygectomy was performed in 8 (25.8%) patients, while coccygectomy + partial sacrectomy was performed in 3 (9.7%) patients. Complete en bloc (R0 + R1) resection was performed in 29 patients, while palliative (R2) resection was performed in 2 patients due to tumor invasion and adhesion to vital structures in the pelvis.
The operative time ranged from 40 to 660 min, with a median measurement of 170 (IQR = 125) min. The operative time for the posterior approach group ranged from 40 to 355 min, with a median measurement of 150 (IQR = 90) min, while the operative time for the anterior approach and combined approach groups ranged from 215 to 660 min, with the median measurement of 292.5 (IQR = 205) min. The operative time for the posterior approach group was significantly shorter compared to both the anterior approach and combined approach groups (P = 0.006).
As shown in Table 1, the median length of hospital stay for the entire patient cohort was 14 (IQR = 11) days. Specifically, patients who underwent the posterior approach had a postoperative hospital stay of 12 (IQR = 10) days, while those who underwent the anterior and combined approach had a significantly longer stay of 35 (IQR = 53.5) days (P = 0.002).
Complications
The resection of a segment of the bladder wall and subsequent repair were performed in 1 female patient. Vaginal damage occurred in 1 female patient due to recurrent lesion invasion, which was subsequently repaired following the removal of the recurring tumor. The decision to perform prophylactic ileostomy in one female patient was based on the patient's compromised general condition and extensive surgical field. Tumor perforation occurred in 5 patients during surgical procedures. Uncontrolled presacral hemorrhage was observed in 4 patients, necessitating the implementation of temporary tamponade using a long piece of packing gauze to effectively manage and control the bleeding.
Staged resections were performed on two female patients, one of whom had a recurrent schwannoma and underwent her initial surgery at our hospital. However, only partial resection of the recurrent presacral tumor was conducted. Due to the superior extent of the lesion reaching L5 and the inferior extent reaching the coccyx, we performed a partial resection of approximately 50% of the tumor using a posterior approach. Considering the patient's limited tolerance for further resection, our priority was to expedite the completion of her initial surgery. After a 4-month postoperative recovery period, we performed an anterior approach to surgically resect the remaining tumor. The other female patient diagnosed with fibromatosis underwent 2 surgical procedures for resecting the recurrent lesion via a posterior approach. Due to tumor invasion into the vaginal wall and the patient’s limited surgical tolerance, only partial resection of the recurrent tumor was performed during her initial surgery. After an approximately 9-month postoperative recovery period, the remaining tumor was successfully excised during her second surgery, accompanied by resection of a portion of the vaginal wall and subsequent repair of the injured area (as shown in Table 3).
Table 3 Clinical data of the two patients undergoing staged resectionsRectal wall damage was observed in 4 (12.9%) patients, with one case successfully treated through rectal repair and two cases requiring rectal repair + sigmoidostomy due to recurrent lesions. For the fourth rectal injury, we initially attempted the injury during surgery but were unsuccessful. Subsequently, 10 days post-surgery, a grade III rectal leakage occurred necessitating further surgical intervention. To facilitate the healing of the leakage, a transverse colostomy was performed.
Postoperative wound infection (grade I) occurred in 2 patients (6.5%), while postoperative urine retention (grade I) was observed in 1 patient (3.2%). Following conservative treatment, all patients achieved complete recovery. Another 2 patients (6.5%) experienced postoperative wound infections of grade III, necessitating surgical intervention for management.
No perioperative deaths were recorded during the study period.
Pathology
As shown in Table 4, a total of 13 pathological types were confirmed by histological examination, including 24 (77.4%) benign lesions, 1 (3.2%) intermediate lesion, and 6 (19.4%,) malignant lesions. Among all the pathological types in our study, mature teratoma was the most prevalent benign pathological type (32.3%, n = 10), while liposarcoma (6.5%, n = 2) and teratoma with malignant transformation (6.5%, n = 2) were identified as the most predominant malignant pathological types.
Table 4 Pathologies observed in the studyComplete en bloc (R0 + R1) resection was performed in 29 patients, while palliative (R2) resection was performed in 2 patients due to tumor invasion and adhesion to vital structures in the pelvis (including 1 case of recurrent liposarcoma, 1 case of recurrent fibromatosis). Following pathological confirmation, R0 resection was achieved in 25 patients, while R1 resection was performed in 4 patients, including 1 case of recurrent primitive neuroectodermal tumor (PNET), 1 case of recurrent adenocarcinoma, 1 case of recurrent teratoma with malignant transformation and 1 case of recurrent teratoma, respectively.
Among the 2 patients who underwent R2 resection, the individual with recurrent liposarcoma did not receive any adjuvant therapy post-surgery and succumbed to mortality within 6 months; the individual with recurrent fibromatosis received postoperative high-intensity focused ultrasound (HIFU) treatment after surgery at our institution. The presacral tumors remained stable, and the patient was closely monitored through imaging techniques.
Among the 4 patients who underwent R1 resection, those with recurrent teratoma exhibiting malignant transformation and recurrent PNET received postoperative chemotherapy + radiotherapy at our institution. Conversely, the patients with recurrent teratoma and recurrent adenocarcinoma did not receive any adjuvant therapy following surgery at our institution.
Follow-up
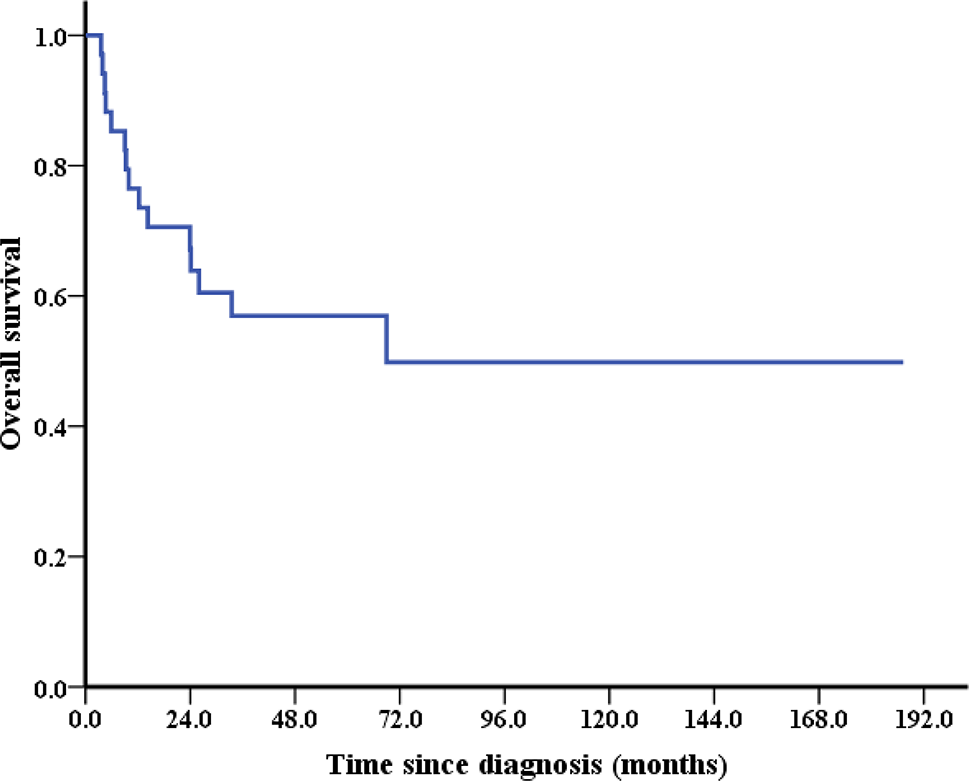
Follow-up assessments were conducted as previously described, with the most recent follow-up occurring in November 2023. The median duration of post-surgical follow-up was 115.5 (IQR = 70, range, 6–157) months. Throughout the follow-up period, 1 patient with teratoma with malignant transformation was lost to subsequent monitoring.
During the follow-up period, tumor recurrence resulted in the death of 5 patients (16.1%). All fatalities were attributed to malignant presacral lesions, including liposarcoma (2 cases), PNET (1 case), adenocarcinoma (1 case), and teratoma with malignant transformation (1 case). These 5 patients succumbed at 6, 9, 10, 22, and 39 months post-surgery in our hospital.
One female patient with foregut cysts experienced tumor recurrence 25 months after surgery, and she declined further surgical intervention for personal reasons. Similarly, 1 male patient with teratoma experienced tumor recurrence 2 months post-surgery; however, he opted against additional surgical treatment as he remained asymptomatic. These two patients are currently being closely monitored through imaging surveillance. Among the remaining patients (n = 23) who underwent surgery for recurrent benign or intermediate presacral tumors at our institution, no evidence of recurrence was observed during the follow-up period.
During the long-term follow-up, constipation occurred in 2 patients, while one patient experienced chronic sacral caudal pain accompanied by constipation. Additionally, lower extremity fatigue was observed in two patients, and urinary incontinence occurred in one patient post-surgery.






留言 (0)