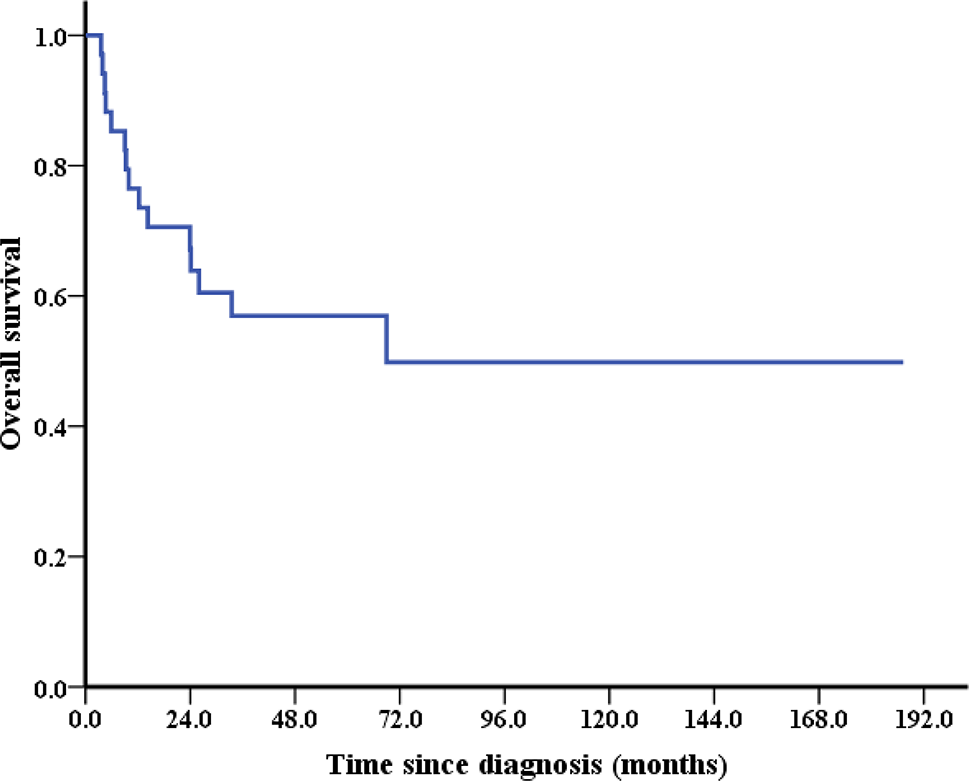
The prognosis of this patient before starting treatment was particularly poor, not only because his tumour harboured BRCA2 mutation and EGFR copy number gain but also because he had multiple metastases within 1 year of diagnosis. With the typical prognosis of metastatic PSCC being less than 1 year, the 2-year survival of this patient is remarkable, especially given that he is currently alive [2]. This patient may have benefited from mutation-specific therapies such as chemotherapy plus immunotherapy, olaparib, and radiotherapy.
A previous study reported cisplatin combined with ifosfamide and paclitaxel (TIP regimen) as prior treatment for metastatic penile cancer [2]. Pagliaro et al. reported 30 patients with locally advanced disease who received neoadjuvant TIP; 15 (50.0%) reached objective response, comprising 3 complete responses (CRs) and 12 partial responses (PRs). Nineteen patients (63.3%) in this group had disease progression or recurrence [7]. Currently, there is no standard second-line regimen after first-line chemotherapy failure. In a study of 17 patients who underwent ≥ 1 salvage therapy after tumour progression from the first treatment, those who were treated with a second cisplatin-based therapy had a median overall survival (OS) of 5.6 months, and those who did not receive a second cisplatin-based therapy had a median OS of 4.3 months [8].
Given the rarity of mPSCC and the high recurrence rate after conventional treatment, it is critical to explore the genomic profile of mPSCC for potential therapeutic targets. Of 20 mPSCC patients who were enrolled to analyse comprehensive genomic profiling (CGP), 10% carried BRCA2 mutations [5]. BRCA2 consists of 5 domains, which bind to DNA and interact with RAD51. Therefore, BRCA2 plays an important role in error-free repair of DNA double-strand breaks by mediating orderly assembly of RAD51 on ssDNA. Individuals with BRCA2 mutations are susceptible to breast, ovarian, and other cancer types [9]. While the genomic landscape of mPSCC has been previously reported, the therapies received by patients and their responses to treatment were not given.
BRCA1/2 mutation carriers are more responsive to chemotherapy treatments than noncarriers in breast cancer and urinary and/or ovarian cancer [10]. Recently, some studies have also shown that the immunostimulatory effects of chemotherapy can improve the efficacy of many immunotherapies because of enhanced genomic instability and immunotherapy activity [11]. and cytoplasmic dsDNA-induced DNA damage and immunogenicity have been proven to induce cell death [12]. Therefore, clinical trials have been developed to investigate the efficacy of combining chemotherapy and ICIs; for example, a significantly longer survival has been observed in non-small cell lung cancer (NSCLC) patients treated with pembrolizumab co-administered with chemotherapy as the first line [13]. Thus far, few studies have applied immune checkpoint inhibitors (ICIs) plus chemotherapy for PSCC. Li et al. reported the efficacy of immunotherapy plus chemotherapy in a patient with PSCC after recurrence. The disease progressed with multiple enlarged inguinal lymph nodes at 11 months after surgery, and immunotherapy combined with chemotherapy was administered. Pelvic magnetic resonance imaging (MRI) showed that the multiple lymph nodes in the groyne area disappeared [14]. However, no relevant reports on immunotherapy combined with chemotherapy in advanced penile SCC with BRCA mutations are available.
Here, we report the first mPSCC patient with BRCA2 mutation whose disease was stable for 9 months when receiving treatment with olaparib combined with pembrolizumab and anlotinib. BRCA2 p.S3245X was detected in the penis primary lesion, metastatic thigh lesion, and lung lesion of this patient. As with previous studies in other solid tumours, tumours with BRCA2 mutations are sensitive to treatment with poly (ADP-ribose) polymerase inhibitors (PARPi). Olaparib is a PARPi that inhibits PARP enzymes such as PARP1, PARP2, and PARP3. PARP enzymes are critical for DNA transcription and repair [15]. Based on the results of a series of clinical trials, olaparib has been approved by the FDA as a treatment for ovarian cancer, breast cancer, pancreatic cancer, and prostate cancer [16]. Meanwhile, the FDA has specified that the mutation status of patients should be identified before treatment. To date, several biomarkers have been confirmed to be able to indicate the sensitivity of patients to olaparib, including BRCA mutation and homologous recombination deficiency (HRD)-positive and homologous recombination repair (HRR) gene mutation. However, olaparib usage is linked to varied adverse effects, as revealed in a meta-analysis of 14 studies with 5119 cases [17]. Adverse reactions vary across different cancers. Notably, fatigue is prominent in pancreatic cancer, while ovarian cancer shows increased severity in anaemia, neutropenia, nausea, and vomiting. Breast cancer exhibits notable grade 3 or above adverse reactions with fatigue and vomiting. Furthermore, there is currently no relevant research on the side effects of olaparib in penile cancer. Therefore, using olaparib in penile cancer carries maybe certain risks. Our case is the first report of a penile cancer patient with BRCA mutation benefiting from olaparib treatment, but further research is needed to expand its applicability in the future.
BRCA1/2 mutation carriers are not only more responsive to chemotherapy and PARPi than noncarriers but are also sensitive to radiotherapy [18]. Alain Fourquet et al. reported that breast cancer patients who received radiotherapy had a major clinical response rate of 68% (13/19 tumours). This study suggests that BRCA1/2 mutations are associated with higher response rates to radiosensitivity in breast cancers. In a recent systematic review of the literature, PARPi were also efficient radiosensitizers capable of enhancing the death ratio between 1.04 and 2.87 in several tumour models [19, 20]. The reason is the synergistic effects on DNA damage caused by ionizing radiation and inhibition of proteins essential for DNA damage repair by PARPi. Radiotherapy is used for penile cancer, but few articles have reported efficient radiotherapy. In our case, the patient carried a BRCA2 mutation and received PARPi therapy after radiotherapy, and follow-up chest CT scans (October 2022) showed significant tumour shrinkage. These findings indicate that in penile cancer, cases involving BRCA mutation are sensitive to radiotherapy and/or PARPi. However, larger clinical samples may be needed to confirm this in the future.
Of note, in our case, the patient’s disease was stable at 9 months after triple therapy of olaparib with pembrolizumab and anlotinib, and the patient also benefits from radiation therapy and chemotherapy plus immunotherapy. All of these results indicate that the combination of immunotherapy and targeted therapy as well as radiation therapy were beneficial for restricting tumour progression in this patient. Therefore, to potentially increase treatment efficacy and prevent the development of disease resistance, we hypothesize that if radiation therapy is used immediately after lung metastasis, it may further improve the quality of life of patients.
In conclusion, the drugs available for treating recurrent PSCC are very limited. This is the first report of olaparib efficacy in treating PSCC with BRCA2 mutation. We report a PSCC patient with BRCA2 mutation who received olaparib combined with pembrolizumab and anlotinib, with satisfactory effects. Furthermore, posterior-line treatment options for recurrent PSCC with BRCA2 mutation were studied, and the effectiveness of chemotherapy combined with immunotherapy and radiotherapy was verified. The results suggest potential treatment options for advanced or refractory PSCC and show that genetic testing facilitates personalized tumour treatment, offering a pathway to individualized therapeutic strategies.






留言 (0)