The present study aimed at developing and externally validating a scoring system for the prognostication of in-hospital all-cause mortality of patients with OHCA undergoing coronary angiography. By utilizing multivariable logistic regression analysis, key variables that are associated with increased in-hospital mortality were identified and incorporated into an easily computable score (FACTOR score). External validation of the score confirmed its excellent prognostic accuracy. As such, a reliable prognostic tool was developed.
The FACTOR score utilizes only four clinical variables, explicitly: age, downtime (≥ 10 min or unwitnessed arrest), first detected rhythm and administration of epinephrine, all of which are readily available at the time of hospital admission. Despite using only four easily available variables, the FACTOR score achieved a reliable prediction of in-hospital mortality with an AUC of 0.83 in an external validation cohort. Furthermore, the FACTOR score demonstrated high diagnostic accuracy in predicting survival with good neurologic outcome in the external validation cohort.
Predicting outcomes is relatively straightforward when dealing with extreme cases in the clinical spectrum, such as those with very favorable or very unfavorable conditions. However, a majority of patients are found to be in a 'gray area,'. These unresponsive patients may undergo significant recovery despite initially inconclusive examination results even after a prolonged duration or they may never recover from the neurological damage [9]. So far, clinical tests are lacking accuracy. A score which could provide further help in prognostication would, therefore, be highly useful. Currently, guidelines advise waiting a minimum of 72 h post-cardiac arrest before conducting the initial neurological assessment without sedation, yet this duration might be too short [10]. It would, therefore, necessitate an extensively longer stay at the intensive care, leading to significant costs [9]. The FACTOR score could prove useful in allowing healthcare professionals in resource allocation in these specific settings.
Previous studies have proposed various scores (e.g., OHCA score and ACLS score) for prognostication in OHCA patients [3, 11,12,13,14,15,16,17]; however, they were mostly not externally validated [11,12,13,14,15], meanwhile outdated [13, 15, 16], incorporated only a small number of patients with OHCA due to cardiac causes or are very cumbersome to calculate [11, 12, 16]. Further, one score required an exact downtime, which is often not available, thereby excluding patients with unwitnessed cardiac arrest [16].
Another score to predict short-term mortality in OHCA patients is the NULL-PLEASE score. Even though it was derived in an only small patient cohort, it showed very good prognostic accuracy in an external validation study comprising a cohort of 700 patients with OHCA. However, its prognostic accuracy did not translate effectively to our cohort, only achieving an AUC of 0.59. Similarly, the OHCA score derived by Adrie et al. in a similar patient setting only achieved an AUC of 0.56 in our cohort [16]. This disparity in prognostic performance could be attributed to several factors. For instance, differences in the prevalence of CAD, as well as disparities in patient demographics and characteristics such as a lower prevalence of metabolic syndromes in Switzerland could have contributed. Further, differences in healthcare systems and EMS strategies could play a role. Another significant aspect that might influence the accuracy of the previously discussed scores in our cohort could be differences in geographical conditions: the present study was conducted in Switzerland, which has a dense population, thereby short transportation times and a possibly higher chance of bystander CPR. Moreover, it is among the regions with the highest density of hospitals and has a highly elaborated healthcare system. All together, these factors may also contribute to the relatively high number of survivors compared to other studies. However, the majority of the discussed studies did not display important results such as the baseline characteristics of their patient cohort and hence, our interpretations remain hypothesis generating only. Lastly, some scores such as the NULL-PLEASE score used cut off values for variables only. To address the lack of accuracy of previous published tests and enhance the applicability of our study, we developed a comprehensive nomogram within our patient cohort. This nomogram incorporates our scoring system along with the health care centers’ overall mortality rates for patients experiencing OHCA.
A strong association between neurological outcomes and mortality was observed. The most likely explanation is that there were more treatment discontinuations due to a limited neurological prognosis. Decisions on discontinuation of treatment, however, are also further influenced by other limiting comorbidities. However, given that the primary focus of this study did not involve predicting neurological outcomes, it is plausible that the development of a score specifically designed to predict favorable neurological recovery could potentially yield superior predictive performance. The main objective of the secondary endpoint was to offer insights into survival with a good quality of life.
Interestingly, the mortality risk in patients with CPR initiation by laypersons tended to be comparable to that of initiation by policemen or firefighters (Suppl. Table 3). However, the initiation of CPR by medical personnel that was on the scene by chance significantly reduced the risk of in-hospital death. The significant reduction in mortality after CPR by medical personnel compared to laypersons or semi-professionals (firefighters or policemen) suggests that if initial CPR is not performed through medical personnel, it is likely insufficient. Consequentially, mortality can be substantially reduced if CPR is sufficiently performed from the very beginning. This reflects the urgent need for enhanced CPR training in the general population as well as firefighters and police officers, who frequently initiate CPR (10% in this study). Ultimately, the implementation of enhanced CPR training and additional educational resources could yield favorable outcomes on a broader scale [18].
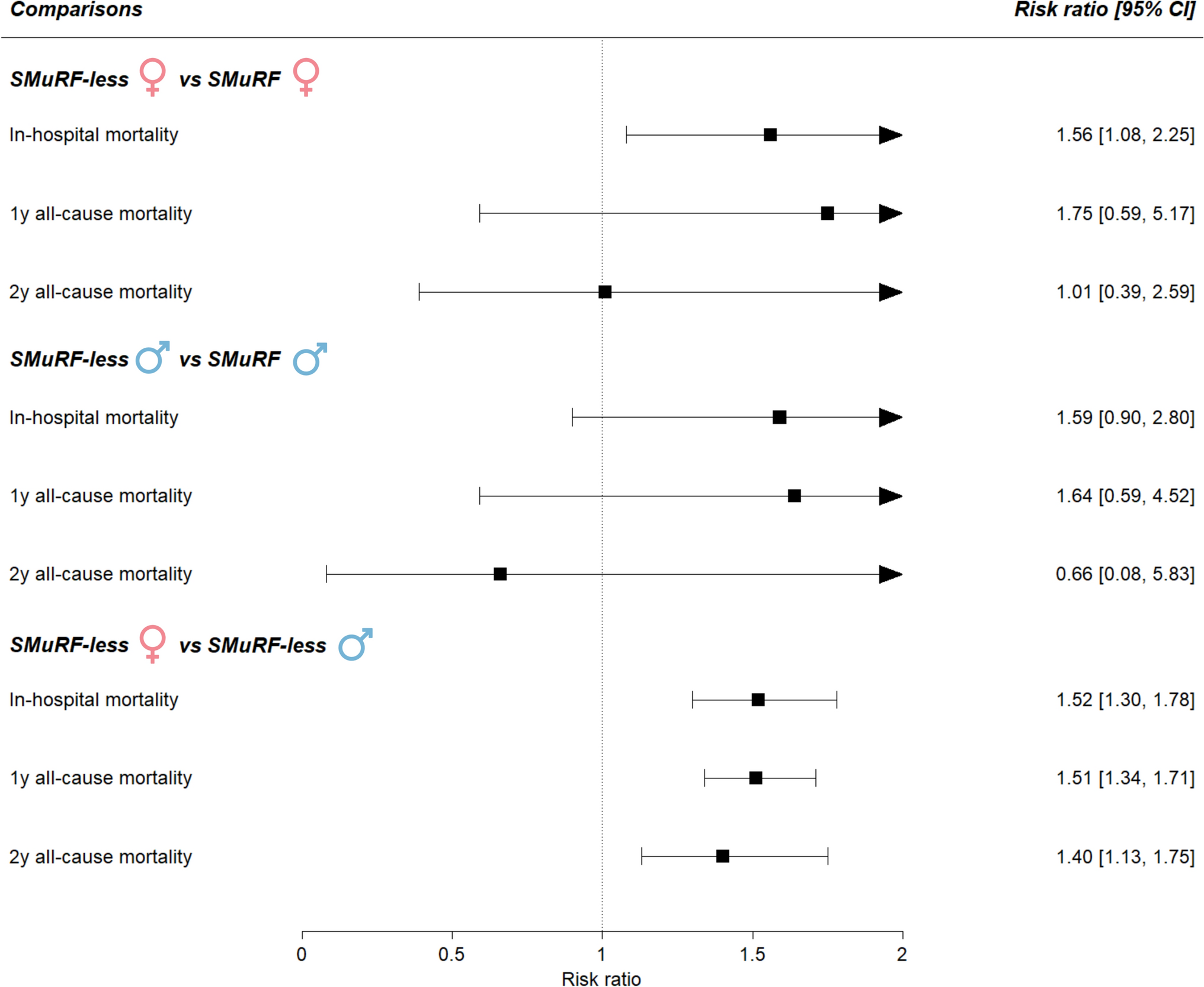
Sex differences in the prognostic accuracy of scoring systems can often be observed [19]. This might be attributable to the lower prevalence of female patients in studies involving patients with ACS and that while initially presenting similarly in the ER, women and men do have different outcomes [19, 20]. In the present study, when comparing the prognostic performance of the FACTOR score on the all-cause mortality between males and females, it was found that the FACTOR score exhibited similar diagnostic accuracy in both sexes. However, in the present studies’ cohort, female patients only comprised 16% of the total population.
Limitations.
Some limitations merit consideration. The study is limited by its retrospective, single-center design with a moderate sample size, which, however, represents a larger derivation cohort than the so far best validated Null-PLEASE score [21]. Further, since only patients who also underwent coronary angiography were included, a selection bias exists. We, therefore, cannot comment on patients who have had therapy withdrawn, while in the emergency department due to a dismal neurological prognosis.
Switzerland has a rather dense population and a well-developed health care system. Therefore, the applicability and usefulness of our score may be constrained when employed in a distinct patient population and healthcare system, as well as different geographical contexts such as rural areas.



留言 (0)