when it comes to bio-signals, expectations are to get data that provide a clear insight into what is analyzed. But the intrinsic variability of physiological processes makes the measurement method a critical choice. The swallowing process is no exception, and several methods have been developed to better understand its functioning [29]. However, no unique approach exists to entirely reveal its subtleties and several of them are often used in combination to compensate. But very few can be used daily and even be implanted. Yet, we aim at the feasibility of an implantable active artificial larynx as a natural airway rehabilitation method, following total laryngectomy. Currently, the surgery permanently separates the air passage from the bolus passage with the creation of a tracheostomy: the trachea is sewn on the anterior neck to allow breathing, and no air passes through the mouth and the nose anymore. Previous attempts have already shown the possibility to implement an artificial larynx to set the trachea back in place and restore the natural airways [2], [3]. The prosthesis was entirely passive and allowed the patients to breathe and swallow normally. However, food residues were found in the trachea [4] and the possibility to develop a real-time and safe detection of swallowing could significantly improve the safety of such a system, by allowing to close any active mechanism that would temporarily protect the airway during swallowing. This would therefore enable the development of an implantable active artificial larynx.
This translates into the need for an implantable physiological measurement that can provide meaningful swallowing data as early as possible, once the swallowing has started. This could allow to protect the airways as soon as possible before the bolus put the airway at risk of aspiration. Also, the data should be as dedicated as possible to swallowing, to forbid any swallowing detection failures. Indeed, the more diversified is the content of a signal, the more challenging it becomes to differentiate a specific activity (i.e swallowing). These requirements arise from the functioning of real-time detection algorithms, that can analyze the signals as they arrive and to discriminate the event in progress before it is completed. Therefore, the efficiency of such algorithms depends on the measured data, which requires looking for both suitable anatomical structures and implantable measurement methods.
In that regard, when it comes to physiological evaluation and identification of specific movements, muscle activity recording with electromyography (EMG) is the preferred method and comes with a large corpus of study in various fields. In addition, it is one of the few measurement methods that can be implanted [18]. It consists of the measurement of the seemingly random firing of all the muscle fibers situated within the sensitive area of an electrode. The content of the resultant signals is, therefore, inherently random, but it gives access to distinct muscle activity and allows to evaluate their recruitment intensity and their temporal relationships [1]. However, EMG has little been used in swallowing detection and was mostly combined with other measurement methods. Also, these approaches only used surface electrodes, which limits the access to swallowing-related data and showed limited detection accuracy with regard to the requirements we described for a real-time detection [18]. Therefore, these results mitigate the interest in an EMG-based swallowing detection so far, and further explorations are required to look for muscles that could provide earlier and more dedicated data.
Indeed, thoroughly selected anatomical areas could provide more qualitative myoelectric data, and surface electrodes limit the measurements to the superficial muscles only. Moreover, EMG-based detection strategies have already shown promising results in the field of upper limb gesture recognition, both with surface [10], [23] and implanted electrodes [21], to measure the residual muscles of amputees. It allows for the myoelectric control of a robotic arm with multiple movements, which is meant to reproduce seemingly natural movements through real-time detection. Yet, the swallowing process is considered to be mostly reflex, driven by the central pattern generator, a group of neurons located in the brain stem. This makes it a quite stereotypical process, as opposed to limb movements, and the requirement of the airways to be protected actually falls down to an on/off detection. This encourages the idea that the swallowing process might provide robust data, and intramuscular EMG would allow to overcome the limit of surface electrodes, to evaluate deep muscles that have never been considered so far. In addition, while total laryngectomy removes the larynx and impairs various neck area, several muscles are only separated from the hyo-laryngeal complex via their insertion point and are left in place with no damage [15], [18]. This could therefore give access to their activity to an implantable real-time detection system, similar to a robotic arm that measures the activity of the residual muscles of the arm.
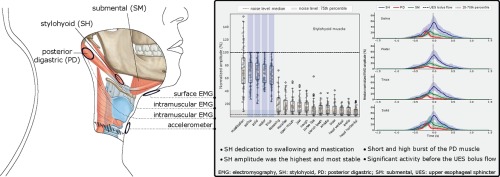
In this regard, the stylohyoid and the posterior digastric muscles have little been studied but few results hint toward their importance. First off, they are part of the suprahyoid muscles and are morphologically suited to act on the upward and forward movements of the hyoid bone [27]. Subsequently, the hyoid bone is joined together with the larynx and its movements directly act on the opening of the upper esophageal sphincter (UES), for the bolus to enter the esophagus safely. In other words, this suggests that the stylohyoid and the posterior digastric muscles essentially act on the stabilization of the hyoid bone. In comparison, although the submental muscles are well studied and have been shown to contain key swallowing muscles involved in hyoid bone movements [18], [27], they also constitute the floor of the mouth and support the tongue in its various actions. So, this latter point is likely to limit their ability to provide a swallowing dedicated activity. Besides, the particular attention that previous works have given to the submental muscles is likely due to their accessibility, but the stylohyoid and the posterior digastric muscles might deserve similar attention. Especially, for a real-time swallowing detection, we hypothesize that the stylohyoid and the posterior digastric muscles could provide more dedicated and potentially earlier data than the submental muscles.
This is further supported by recent investigations based on modern imaging methods that evaluated the physiological response of the stylohyoid and the posterior digastric [25]. The authors showed that they significantly activate during swallowing, but they did not provide comparisons with other activities. However, Kurt et al. [12] reported on both muscles, studied as a whole stylohyoid-posterior-digastric (STH-PD) complex with intramuscular EMG, and observed that it mainly activated for saliva swallowing, mastication and jaw opening. But the variety of tasks was limited and no strict and quantified comparisons were provided. Their study actually mainly focused on the nerve conduction evaluation of the muscles, which are innervated by the facial nerve. They emphasized that the STH-PD complex seems to have nothing to do with mimicry but has similar functions to the submental muscles, which are innervated by the trigeminal nerve. They suggest that this intermediary position may facilitate the electrophysiological identification of swallowing.
Besides, regarding the requirement in early data for the development of a real-time and safe detection of swallowing, the definition of a temporal limit after which the airway must be closed could allow us to better evaluate the potential of the measured signals. This time point is chosen to be the moment when the bolus passes through the UES, when the pressure in the throat suddenly increases and the airways are at the highest risk of aspiration [18]. This moment has been shown to be accessible via the swallowing sound measurement [19].
This paper, therefore, intends to evaluate the ability of the stylohyoid and the posterior digastric to provide early and dedicated data about swallowing, measured with intramuscular EMG. We specifically focused on their recruitment pattern and hypothesized that they exhibit a repetitive and potentially identifiable activity. We also measured the submental muscles with surface EMG, to provide a basis for recruitment comparison, and the swallowing sound with an contact transducer, to provide a basis for the evaluation of the temporal aspects of the muscles recruitment.



留言 (0)