
記住我



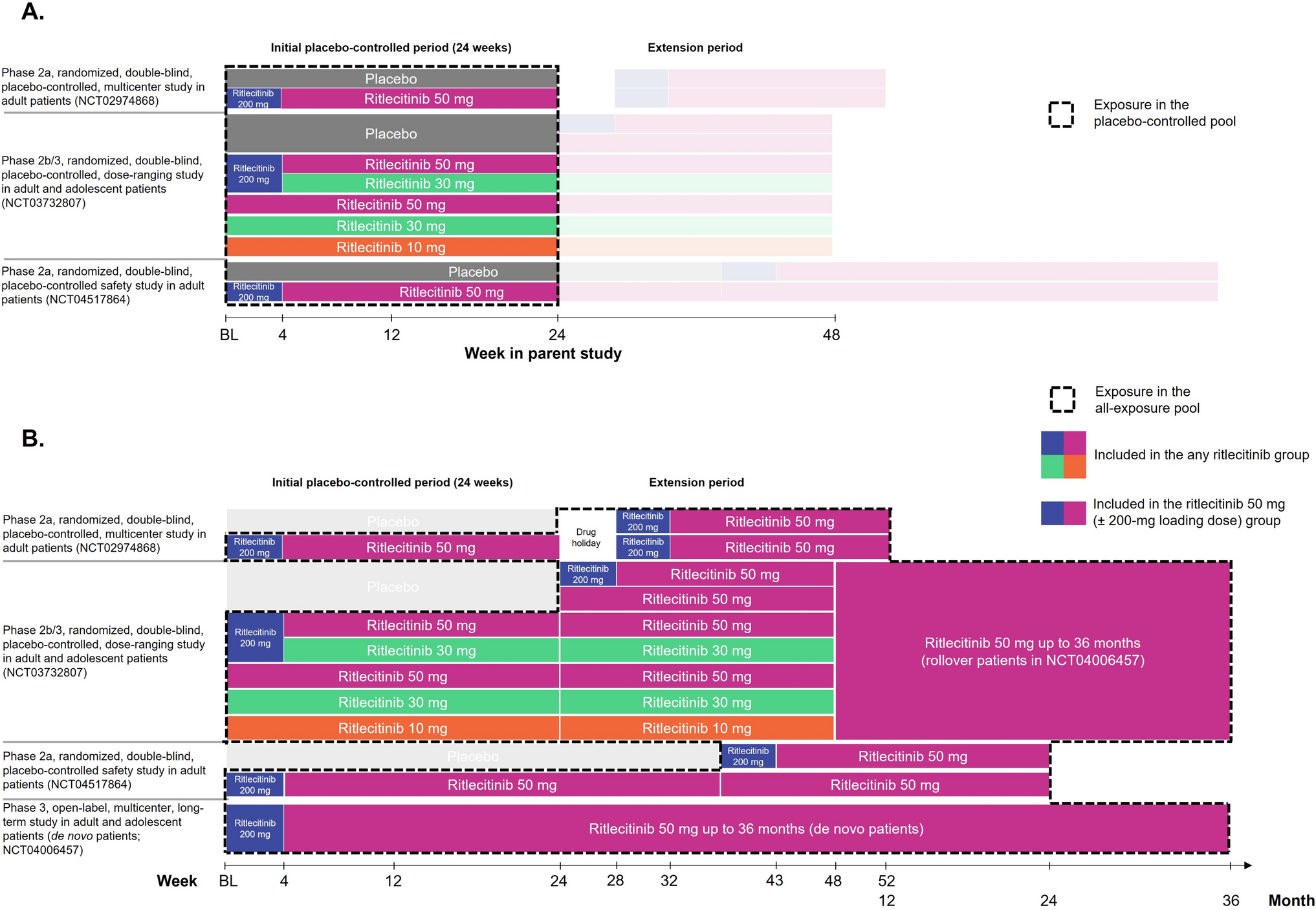
The placebo-controlled pool included 881 patients: 215, 130, 345, 261, 62, and 213 patients in the ritlecitinib 200/50-mg, 50/50-mg, all 50-mg, all 30-mg, 10-mg, and placebo groups, respectively. The all-exposure pool comprised a total of 1294 patients (any ritlecitinib group), of which 1228 patients received ritlecitinib 50 mg with or without a 200-mg loading dose (ritlecitinib 50-mg group). Baseline characteristics for patients in the placebo-controlled pool and the all-exposure pool were comparable (Table 1) and were well matched between treatment groups in the placebo-controlled pool. Median age was 33.0 and 32.0 years in the placebo-controlled and all-exposure pools, respectively; 11.9% (n = 105) and 14.0% (n = 181) of patients were adolescents, respectively. The majority of patients were female and white; 22% of patients in each pool were Asian.
Table 1 Demographic and baseline characteristics in the placebo-controlled and all-exposure poolsIn the placebo-controlled pool, median [interquartile range (IQR)] exposure was 169 (167–173) days in each of the ritlecitinib and placebo groups. Total patient-years (PY) were 96.1, 58.3, 154.4, 114.7, 27.6, and 94.9 for the ritlecitinib 200/50-mg, 50/50-mg, all 50-mg, all 30-mg, 10-mg, and placebo groups, respectively. In total, 67 patients (7.6%) discontinued during the placebo-controlled period (Table S4). Among the 1294 patients in the all-exposure pool, median (IQR) exposure was 624 (407–792) days (2091.7 total PY); 1052 (81.3%) and 533 (41.2%) patients had ≥ 12 months and ≥ 24 months of cumulative ritlecitinib exposure, respectively (Table S5). Maximum duration of exposure was 1181 days (approximately 39 months). In the ritlecitinib 50-mg group, median (IQR) exposure was 547 (366–716) days (1813.7 total PY). At the time of data cutoff, 367 patients (28.4%) had discontinued in the all-exposure pool (Table S6).
3.2 Safety and Tolerability in the Placebo-Controlled Pool (up to 24 Weeks)In the placebo-controlled pool, AEs occurred in 70.2%, 75.4%, 72.2%, 71.3%, and 69.4% of patients in the ritlecitinib 200/50-, 50/50-, all 50-, all 30-, and 10-mg groups, respectively, and in 69.5% of patients who received placebo (Table 2). Most treatment-emergent AEs (TEAEs) were mild to moderate in severity across treatment groups. There was no increase in overall number of TEAEs, SAEs, or severe AEs with increasing dose, and no individual SAE was reported for more than one patient in any treatment group during the placebo-controlled period. The number of temporary discontinuations due to AEs was higher in the ritlecitinib groups, occurring in 6.9–10.0% of patients compared with 3.8% of patients who received the placebo. The number of permanent discontinuations from the study or study drug due to AEs was similar across treatment groups and the placebo (1.5–3.2% for ritlecitinib groups versus 2.3% for placebo). Overall, the most common AEs (≥ 5% in any treatment group) were nasopharyngitis, upper respiratory tract infection, and headache (Table 2). The most frequent AEs (≥ 2% in any treatment group) that occurred more commonly in the ritlecitinib groups than the placebo, and in a dose-related fashion, were diarrhea, acne, urticaria, rash, and dizziness.
Table 2 Overall safety summary and frequent treatment-emergent adverse events (all causalities) for the placebo-controlled pool3.3 Longer-Term SafetyThe proportions of AEs, SAEs, and severe AEs across the all-exposure pool are presented in Table 3. In the any-ritlecitinib group, AEs were reported in 1094 patients (84.5%), SAEs in 57 (4.4%), and severe AEs in 83 (6.4%); 78 patients (6.0%) permanently discontinued due to AEs. The most common TEAEs in the any-ritlecitinib group were headache (17.7%), SARS-CoV-2 positive test (15.5%), nasopharyngitis (12.4%), acne (10.4%), and upper respiratory tract infection (10.2%). Except for events related to coronavirus disease 2019 (COVID-19, which predominantly occurred outside of the placebo-controlled periods), AEs were similar to those in the placebo-controlled pool. The incidence of AEs, SAEs, and severe AEs was consistent across the any-ritlecitinib and ritlecitinib 50-mg groups. Events in the infections and infestations system organ class were the most frequent SAEs (full listing of SAEs in Table S7); pregnancy (12 patients; 0.9%), headache, and urticaria (4 patients each; 0.3%) led to most of the permanent discontinuations. There were two deaths (0.2%) due to breast cancer and acute respiratory failure/cardiorespiratory arrest (described below).
Table 3. Summary of treatment-emergent adverse events (all causalities) in the all-exposure pool3.4 Adverse Events of Special Interest3.4.1 InfectionsThe proportions and IRs of serious infection in ritlecitinib groups were low across both the placebo-controlled and all-exposure pools. Serious infections occurred in 0.9% of patients in the 200/50-mg group, 0.6% in the all 50-mg group, 0.4% in the all 30-mg group, and none in the 50/50-mg and placebo groups. In the all-exposure pool, serious infections were reported in 12 patients (1.0%) in the ritlecitinib 50-mg group (IR: 0.66/100 PY [95% CI 0.35, 1.13]) and in 14 patients (1.1%) in the any ritlecitinib group (IR: 0.64/100 PY [95% CI 0.36, 1.06]) (Fig. 2). The most frequent serious infections (each occurring in ≤ 0.4% of patients in each group) included appendicitis, COVID-19, and COVID-19 pneumonia. Per protocol, all serious infections required discontinuation; however, all events resolved or were resolving, and none were fatal.
Fig. 2
IRs per 100 PY for adverse events of special interest (a–i). IRs are exposure adjusted and expressed as the number of patients with events per 100 PY. IR incidence rate, MACE major adverse cardiovascular events, NMSC nonmelanoma skin cancer, PY patient-years, VTE venous thromboembolic events. Study size–adjusted IRs are per 100 PY and are shown with mid-p gamma CIs. Ritlecitinib all 30 mg includes patients who received ritlecitinib 30 mg QD with or without an initial 4-week 200-mg QD loading dose. Ritlecitinib all 50 mg and ritlecitinib 50 mg includes patients who received ritlecitinib 50 mg QD with or without an initial 4-week 200-mg QD loading dose from the placebo-controlled and all-exposure pools, respectively. aAdjudicated safety events. bIRs shown for breast cancer in female patients. cMACE was defined as a composite of death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke. dVTE was defined as events of deep vein thrombosis and pulmonary embolism
In the all-exposure pool, one patient (< 0.1%) in the 200/50-mg group experienced a TEAE of varicella zoster virus infection, which was adjudicated as an opportunistic infection (OI) of multidermatomal herpes zoster (HZ) [IR: 0.05/100 PY (95% CI 0.00, 0.23)]. The event was mild in severity and resolved without treatment interruption. There were no cases of active tuberculosis in any safety pool. With a single case of OI (multidermatomal HZ) across the entire pool of data, incidence rates of OIs were low across the placebo-controlled and all-exposure pools (Fig. 2).
In the placebo-controlled pool, HZ occurred more frequently in some ritlecitinib groups (50/50 mg, 1.5%; all 50 mg, 0.9%; all 30 mg, 0.8%) than in the placebo group, in which no events were reported. All were nonserious, mild, or moderate, and all resolved; there were no events with visceral involvement. In the all-exposure pool, the proportion of patients with HZ was 1.5% [0.99/100 PY (95% CI 0.60, 1.55)] in the ritlecitinib 50-mg group and 1.5% [0.92/100 PY (95% CI 0.57, 1.40)] in the any ritlecitinib group (Fig. 2); most events were localized, with only one event affecting multiple dermatomes (the OI described above). One patient (0.1%; 71-year-old woman; 50-mg group) who experienced HZ was permanently discontinued from the study; the event was deemed moderate and related to treatment, and the patient was recovering at the time of discontinuation. Across the program, the median time to onset for HZ events was 37.4 weeks, and most cases resolved in < 6 weeks (median 15.0 days). Events of herpes simplex were not dose dependent; a higher incidence was observed with placebo than ritlecitinib 50 mg (Fig. 2).
3.4.2 Dermatological EventsIn the placebo-controlled pool, the proportions of patients with dermatological events of interest were similar across treatment groups. The most frequently reported dermatological AEs (> 2% in any treatment group) across all treatment groups were urticaria, folliculitis, acne, dermatitis atopic, dermatitis contact, pruritus, and rash. Events that occurred more commonly in patients in the all 50-mg group than placebo included urticaria (4.9% versus 1.4%), folliculitis (4.9% versus 1.9%), atopic dermatitis (2.3% versus 0.5%), and rash (3.2% versus 1.4%). The number of dermatological events of interest in the all-exposure pool was similar to that reported in the placebo-controlled pool. The most frequently reported dermatological events in the ritlecitinib 50-mg and any ritlecitinib groups included acne (9.0% and 10.4%, respectively), urticaria (6.0% and 6.8%), and folliculitis (5.1% and 6.3%); all events were nonserious and mild to moderate in severity, and few led to interruption or discontinuation of treatment. The majority (52.8%) of urticaria events occurred during the first 12 weeks of treatment (median time to onset: 10.1 weeks; Table S8); four patients (0.3%) permanently discontinued from the study due to urticaria.
3.4.3 MalignanciesSeven events were adjudicated as malignancies (excluding NMSC) in the all-exposure pool [0.32/100 PY (95% CI 0.14, 0.64)]; all events were reported in the ritlecitinib 50-mg group, and 2 (both breast cancers) occurred during the placebo-controlled period (Fig. 2, Table 3). Breast cancer occurred in four female patients [0.5%, IR: 0.29/100 PY (95% CI 0.09, 0.70)], for whom one event was fatal. The SAEs of breast cancer occurred in a 64-year-old woman (50-mg group), a 66-year-old woman (50-mg group), a 58-year-old woman (50-mg group), and a 46-year-old woman (200/50-mg group); clinical details for all SAEs of breast cancer are provided in Table S9. For the four events of breast cancer, the time to onset of the event ranged from 68 to 299 days (median 156 days) after starting ritlecitinib. All four patients had identified risk factors, including supplemental estrogen therapy, family history of breast cancer, or nulliparity in two patients, current smoker or a history of smoking in three patients, and alcohol consumption in all four patients.
There was one event each of testicular cancer (21-year-old man, 50-mg group; recovered/resolved) and papillary thyroid cancer (26-year-old man, 50-mg group; ongoing at the time of discontinuation); one adjudicated event of malignant melanoma (50-year-old woman, 50-mg group; ongoing at the time of discontinuation) was reported (Table S9).
There were three patients (0.2%) with adjudicated NMSC reported in the all-exposure pool [0.14/100 PY (95% CI 0.03, 0.38)], all of which occurred in the ritlecitinib 50-mg group [0.15/100 PY (95% CI 0.03, 0.43)]; these included two patients (0.2%) with basal cell carcinoma and one patient (0.1%) with Bowen disease (Table 3).
3.4.4 Cardiovascular SafetyIn the ritlecitinib 50-mg group of the all-exposure pool, three patients (0.2%) with SAEs adjudicated as MACE were reported [0.15/100 PY (95% CI 0.03, 0.43)] (Fig. 2). These included one event of myocardial infarction in a 49-year-old man (200/50-mg group), who was a current smoker with a history of hyperlipemia and diabetes. The patient underwent percutaneous transluminal coronary angioplasty/percutaneous coronary intervention the following day; treatment was discontinued and not resumed. The other events included one retinal artery occlusion in a 48-year-old woman (200/50-mg group) with a history of congenital carotid artery defect, patent foramen ovale, and migraine. This patient also experienced a non-SAE of antiphospholipid syndrome and was discontinued from the study. One sudden CV death (acute respiratory failure and cardiorespiratory arrest) occurred in a 51-year-old woman (50-mg group) with a history of asthma, anxiety, and smoking; ongoing concomitant medication was salbutamol for asthma (additional clinical details are provided in Table S10).
One patient (54-year-old woman) in the ritlecitinib 50-mg group of the all-exposure pool experienced a pulmonary embolism (PE) that met adjudication criteria for a VTE [0.06/100 PY (95% CI 0.00, 0.29)]. This patient had potential risk factors, including a recent positive SARS-CoV-2 test and a medical history of morbid obesity, sleep apnea, hypertension, hyperlipidemia, and monoclonal gammopathy of undetermined significance (Table S10). No AEs met the adjudication criteria for deep vein thrombosis.
3.4.5 Neuroaudiological EventsIn the all-exposure pool, the most frequently reported adjudicated events of interest term was paresthesia and dysesthesia. In the ritlecitinib 50-mg group, 21 patients (1.7%) experienced TEAEs meeting criteria for adjudicated term paresthesia and dysesthesia [1.11/100 PY (95% CI 0.69, 1.67)] and three patients (0.2%) experienced TEAEs meeting criteria for adjudicated peripheral neuropathy [0.16/100 PY (95% CI 0.03, 0.45)]. In the any ritlecitinib group, 26 [2.0%; IR: 1.20/100 PY (95% CI 0.80, 1.75)] and four [0.3%; IR: 0.18/100 PY (95% CI 0.05, 0.45)] patients had adjudicated paresthesia and dysesthesia and peripheral neuropathy, respectively (Table 3).
In this analysis, TEAEs adjudicated by the external committee to meet criteria for an audiological event of interest reflect both the outcomes of protocol-specified audiological testing (even in the absence of spontaneously reported TEAEs related to hearing loss) and spontaneously reported TEAEs related to hearing loss. In the all-exposure pool, there were 12 patients [1.0%; 0.67/100 PY (95% CI 0.36, 1.16)] with TEAEs adjudicated to meet criteria for sensorineural hearing loss in the ritlecitinib 50-mg group and 14 patients [1.1%; 0.64/100 PY (95% CI 0.36, 1.06)] in the any ritlecitinib group; these events were all identified through protocol-specified audiological testing (Table 3), and no events were adjudicated as central hearing loss.
3.5 Laboratory AssessmentsOverall, ritlecitinib was associated with small short-term changes in hematological parameters that remained stable during long-term treatment. Median platelet levels decreased to week 4 and remained stable at a lower level through month 36 (Fig. 3). In the all-exposure pool, no patients had platelet counts considered Common Terminology Criteria for Adverse Events (CTCAE) grade ≥ 2 or met protocol-specified discontinuation criteria (< 75 × 103/mm3). TEAEs of thrombocytopenia and platelet count decrease were reported in four (0.3%) and seven (0.5%) patients, respectively; one patient (0.1%) was permanently discontinued from the study due to a non-serious AE of thrombocytopenia (platelets 83 × 103/mm3).
Fig. 3
Select laboratory parameters over time. HDL-C high-density lipoprotein cholesterol, LDL-C low-density lipoprotein cholesterol, LLN lower limit of normal, ULN upper limit of normal
There was a slight decrease from baseline in median hemoglobin (Hgb) levels over the first 4 weeks, and then levels subsequently returned toward baseline and remained stable through month 36 (Fig. 3). In the all-exposure pool, TEAEs of anemia were reported for 17 patients (1.3%), and Hgb decrease was reported for 11 patients (0.9%). In the ritlecitinib 50-mg group, one patient (< 0.1%) met discontinuation criteria for change in Hgb (confirmed < 9.0 g/dL or decrease of > 30% from baseline) and one patient (< 0.1%) had Hgb levels considered CTCAE grade 3 (< 8.0 g/dL), leading to temporary treatment discontinuation (Table S11).
Absolute neutrophil count remained stable through month 36 (Fig. 3). In the ritlecitinib 50-mg group, nine patients (0.7%) had absolute neutrophil count decreases considered CTCAE grade 3 (< 1000 to 500/mm3); no patients had a decrease considered grade 4 (< 500/mm3; Table S11). No patients met protocol-specified discontinuation criteria for neutrophils (confirmed < 750/mm3). TEAEs of neutrophil count decrease, neutropenia, and abnormal neutrophil count were reported in five (0.4%), three (0.2%), and one (0.1%) patient, respectively, in the 50-mg group. Overall, two patients (0.2%) discontinued due to neutropenia, including one (0.1%) in the 50-mg group.
There was a decrease in median absolute lymphocyte count (ALC) from baseline to week 4 with ritlecitinib; ALC levels remained stable at a lower level through month 36 (Fig. 3). In the ritlecitinib 50-mg group, 25 patients (2.0%) had lymphocyte count decreases considered CTCAE grade 3 (< 500–200/mm3), and one patient (< 0.1%) had grade 4 lymphocyte count decrease (< 200/mm3; Table S11). One patient (<0.1%) met discontinuation criteria for lymphocytes (confirmed by two sequential tests ALC < 500/mm3).
Treatment with ritlecitinib was associated with concurrent small increases in median total cholesterol, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol from baseline to week 4 that did not progress over time and remained stable through month 36 (Fig. 3). Hyperlipidemia and hypertriglyceridemia were reported in two patients (0.2%) each in the ritlecitinib 50-mg group of the all-exposure pool; none led to discontinuation of study or study drug.
In the placebo-controlled and the all-exposure pool, there was no meaningful change over time in median alanine aminotransferase or aspartate aminotransferase levels. The proportion of patients with alanine aminotransferase or aspartate aminotransferase greater than three times the upper limit of normal (ULN) was similar in the ritlecitinib 50-mg and any ritlecitinib groups (Table S11). In the ritlecitinib 50-mg group, TEAEs of liver function test increase and abnormal liver function test were reported in four (0.3%) and two (0.2%) patients, respectively; none led to permanent discontinuation from the study or study drug. No AEs were adjudicated as Hy’s law or drug-induced liver injury.
There were changes in serum creatinine or creatine kinase (CK) levels over time with ritlecitinib through month 36 (Fig. 3). In the ritlecitinib 50-mg group, 65 patients (5.3%) had CK increases considered CTCAE grade 3 or 4 (greater than five times ULN; Table S11); TEAEs of blood creatine phosphokinase increase were reported in 40 patients (3.3%). In total, three patients (0.2%) permanently discontinued due to blood creatine phosphokinase increases; one patient (< 0.1%) met discontinuation criteria for CK (two sequential tests greater than ten times ULN). No events of rhabdomyolysis were reported, and no AEs, including myalgia, were found to be associated with increases in CK.
留言 (0)