
記住我






Fidelity, or realism, is a fundamental consideration when designing simulation curricula. The Agency for Healthcare Research and Quality's definition of fidelity is “the degree to which the simulation replicates the real event and/or workplace; this includes physical, psychological, and environmental elements.”1 Many strive for the highest fidelity possible within logistical and financial limits. But does the level of physical realism make any difference in learner outcomes for teamwork training? We focus this review on examining that question.
Physical fidelity includes “factors such as environment, equipment, and related tools.”1 It is recognized that fidelity occurs on a continuum from high (ie, extremely realistic, complex, interactive experiences) to low (ie, simplistic, low-tech, not requiring programming). As such, we sought to include studies where high/low may be a comparison of 2 closely related or vastly different simulation modalities. Despite the assumptions that higher fidelity leads to increased learning, satisfaction, procedural skill, learning/skill transfer, and teamwork, there is relatively little evidence in the health professions literature to support or refute this sentiment.2–4 This is in contrast to the abundant literature on the effectiveness of team training, crew resource management (CRM), and fidelity levels in simulation for the military5 and commercial aviation.5–8 Our particular interest focuses on the construct of teamwork and the associated learning outcomes and user experiences as functions of physical fidelity/realism used in the simulations.
METHODSThe review was commissioned by the Society for Simulation in Healthcare as part of a process to generate guidelines for practice. It was planned, conducted, and reported in adherence with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) standards of quality for reporting metaanalyses (see Table, Supplemental Digital Content 1, https://links.lww.com/SIH/A984, which presents the completed PRISMA checklist).9 Although a study protocol had not been previously published for this overview, an a priori protocol was developed and adhered to (see Table, Supplemental Digital Content 2, which presents the review protocol, https://links.lww.com/SIH/A985). Because this is a systematic review of previously published studies, no ethical approval or patient consent was required.
Research QuestionThe a priori protocol used the PICO format (Population, Intervention, Control, Outcomes)10 to formulate the research question: In health care providers and/or health care trainees/students engaging in simulation training for team training (P), does a higher physical realism simulator or task trainer approach (I), as opposed to a lower physical realism or task trainer approach (C), affect the following outcomes: educational (immediate and retention): participant satisfaction, knowledge, skills, and attitudes; clinical: changes in health care practitioner behaviors, and patient outcomes; and process: cost (O).
Study EligibilityWe included all comparative randomized and observational studies (prospective and retrospective) published since 2011 to ensure that the evidence was contemporaneous. Publications of all languages were included if there was an English abstract available. Studies involving unpublished results, trial protocols, commentaries, editorials, and reviews were excluded. We sought to include studies where teams and teamwork were defined as 2 or more people working together during a simulation exercise.
Data SourcesSearch strategies were created by an information specialist using a combination of keywords and standardized index terms pertaining to simulation physical realism and teams involving a comparison (see Table, Supplemental Digital Content 3, which presents the search strategy, https://links.lww.com/SIH/A986). Searches were originally run on January 29, 2022 in CINAHL via EBSCO (1963+), Ovid Embase (1974+), and Ovid Medline (1946+ including epub ahead of print, in-process, and other nonindexed citations). Searches were limited beginning with the year 2011 with conference abstracts, case reports, technical reports, and clinical trial protocols removed. An update of the searches was performed on January 24, 2023.
Study SelectionThe titles and abstracts of all potentially eligible studies were independently screened in duplicate for inclusion. The included studies were then independently screened in more detail for eligibility in duplicate based on set inclusion and exclusion criteria. Any disagreements between the reviewers were resolved by discussion. Included articles were also scrutinized for additional citations.
Data CollectionData from each study were independently extracted by each reviewer, and any conflicts were resolved by discussion to reach consensus. The data included study design, setting, study population, description of intervention and control, and outcomes measured.
AnalysisDue to the substantial clinical and methodological heterogeneity of the studies identified after the search, it was deemed undesirable to perform any metaanalysis, and therefore a narrative summary was provided. Risk-of-bias assessments were performed independently and in duplicate using the revised Cochrane risk-of-bias tool (RoB2)11 for randomized trials and the Newcastle-Ottawa Scale12 for nonrandomized studies. An assessment of certainty of evidence was made using Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology.13
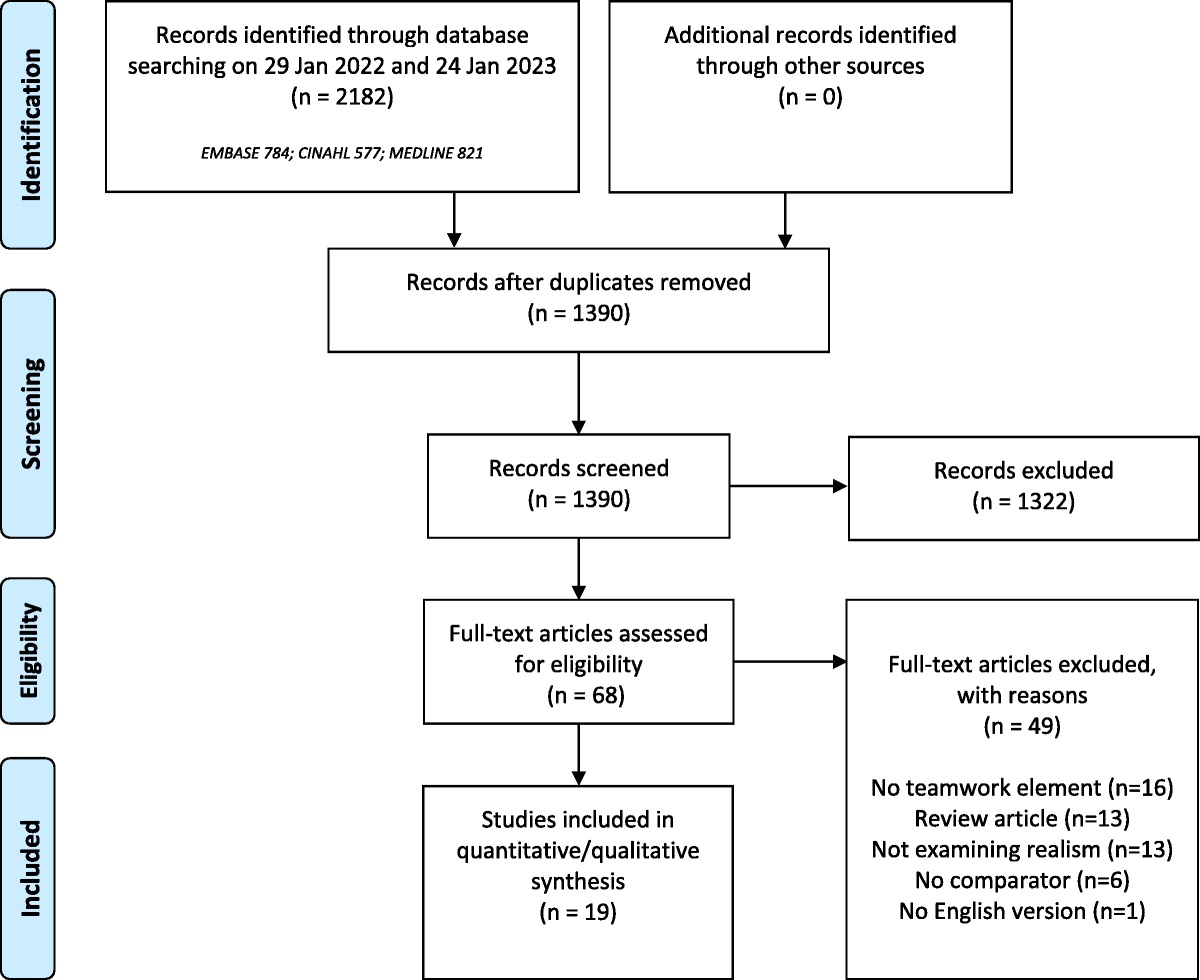
RESULTS Study SelectionThe search identified 1390 articles after removal of duplicates. Of these, 1322 were excluded leaving 68 full-text articles to be screened for eligibility (Fig. 1). In total, 19 studies were identified for inclusion (see Table, Supplemental Digital Content 4, https://links.lww.com/SIH/A987, which details data extraction from the included studies).14–32
 FIGURE 1:
FIGURE 1: Flowchart of inclusion of articles.
Study CharacteristicsFourteen randomized controlled studies with 1530 participants14,16,18–23,26–31 and 5 case-controlled studies with 257 participants15,17,24,25,32 were conducted between 2012 and 2021. Most of the studies were conducted in North America14–16,18–21,25,26,28,29,31 and Europe,17,22,24,27,30 with other locations including New Zealand32 and Singapore.23 Participants included training and independently practicing physicians, nurses, first responders, and technicians including those undertaking interprofessional education courses. Outcomes identified included learner perceptions, confidence, knowledge acquisition, technical skills, nontechnical skills, indicators of stress, and teamwork.
Risk of Bias Within Studies and Certainty of EvidenceThe risk-of-bias assessments are summarized in Tables 1 and 2. There were 4 studies that were assessed to be low risk of bias.16,20,22,24 The main issues identified with the remaining studies related to inadequate blinding of participants and assessors, inadequate randomization, incomplete outcome reporting, and unclear selection processes. The certainty of evidence was judged to be low for indicators of stress (downgraded for inconsistency and risk of bias) and very low for all other outcomes (downgraded for very serious risk of bias and inconsistency).
TABLE 1 - Risk-of-Bias Assessment Using ROB2 for Randomized Controlled Studies Study Year Total (N) Population Allocation Generation Allocation Concealment Blinding Participants Blinding Assessors Outcome Complete Outcome Selective Other Bias Overall Cheng 2013 387 Interprofessional Low Low Low Low Low Low Low Low Curran 2015 66 Medical students Some concerns Some concerns Some concerns High Low Low Low High Finan 2012 16 Neonatal trainees Some concerns Some concerns Low Low Low Low Low Some concerns Katz 2020 25 Anesthesia residents Low Low Low Low Low Low Low Low Kron 2017 421 Medical students Some concerns Some concerns Low High Low Some concerns Low High Lejus-Bourdeau 2021 129 Postgraduate doctors Low Low Low Low Low Low Low Low Liaw 2020 120 Nursing and medical students Some concerns Some concerns Low Low Low Some concerns Low Some concerns Semler 2015 52 Medical residents Some concerns Some concerns Some concerns Low Low Low Low Some concerns Sorensen 2015 100 Interprofessional High High Low Low Low Low Low High Stefanidis 2021 42 Interprofessional Some concerns Some concerns Low Low Low Low Low Some concerns Uslu 2020 84 Interprofessional Some concerns Some concerns Low Low Some concerns Low Low Some concerns Sparks 2017 15 Interprofessional Some concerns Some concerns Low Low Low Low Low Some concerns Wang 2016 40 Interprofessional High High High High Some concerns Low Low High Bultas 2014 33 Pediatric nurses High High High Low High Low Low HighGood quality: 3 or 4 stars (*) in selection domain AND 1 or 2 stars in comparability domain AND 2 or 3 stars in outcome domain. Fair quality: 2 stars in selection domain AND 1 or 2 stars in comparability domain AND 2 or 3 stars in outcome domain. Poor quality: 0 or 1 star in selection domain AND 0 stars in comparability domain OR 0 or 1 stars in outcome domain.
Eleven randomized controlled studies (n = 1343) studied pediatric advanced life support instructors,16 medical students,18,21 postgraduate medical residents,19,22,26,28 pediatric nurses,14 and interprofessional learners.27,30,31 Teamwork was assessed using a variety of instruments: clinical/technical performance rating,14,16,18,21,26 anesthesia nontechnical skills (ANTS),19,22 surgery nontechnical skills,28 team performance rating,14,26,27,31 and team attitudes.30 Fidelity comparisons were made between high- and low-fidelity mannequins,14,16,18,19,22,28,30 virtual reality and multimedia computer,21 immersive simulation and didactic instruction,26 in situ and off-site instruction,27 and hands-on versus computer-based training.31 All studies showed no difference between higher and lower fidelity models for this outcome.
Four case-controlled studies (n = 217) studied medical students15,24,25 and interprofessional learners.17 Teamwork was assessed by the TeamSTEPPS teamwork attitude questionnaire,15 team performance rating,17,24 and observation of participants asserting their leadership.25 Fidelity comparisons were between standardized patients and mannequins,17,25 standardized patients wearing hyperreactive suits and those without,24 and mannequin versus computer-based activity.15 All studies showed no difference in teamwork between higher and lower fidelity models.
Learner PerceptionsEight randomized controlled studies (n = 821)14,18,21,23,28–31 showed increased satisfaction, and 4 studies (n = 306)20,22,26,27 showed no difference in satisfaction between higher and lower fidelity models. Increased satisfaction occurred in studies that compared higher and lower fidelity teaching and learning materials/models. These included comparisons between higher fidelity patient simulators14,18,29 or cadavers28 and lower fidelity noncomputerized mannequins or partial task trainers; higher fidelity virtual reality21 or mannequin31 and lower fidelity computer-based activity, and higher fidelity mannequins plus standardized patients followed by tabletop scenarios versus mannequins and standardized patients alone or tabletop alone.30 One additional study showed an immediate posttest increase in satisfaction for both high-fidelity mannequin and virtual reality groups and sustained significant satisfaction for virtual reality in the follow-up posttest scores but not for the mannequin group.23 Three studies that showed no difference had learner groups of advanced physician trainees and junior faculty (anesthesiology20; anesthesiology, emergency medicine, intensive care22; internal medicine26). One study that compared learning environments (higher fidelity in situ clinic and lower fidelity simulation laboratory/classroom27) showed no difference in satisfaction.
Four case-controlled studies (n = 251)15,24,25,32 showed increased satisfaction for higher fidelity simulation. In a crossover study, medical students preferred standardized patients over mannequins, regardless of whether they first encountered the mannequin or standardized patient.25 A second crossover study showed medical students preferred standardized patients wearing hyperrealistic suits over standardized patients without suits.24 Anesthesiologists showed increased satisfaction for being observed in actual operating room cases over simulated cases, both for routine and crises scenarios.32 Medical students undertaking in-person simulations felt more strongly that they gained an understanding of roles and expectations of those in other professions than those doing online simulations.15
Knowledge AcquisitionFive randomized controlled studies (n = 644)14,16,27,30,31 showed no difference in knowledge acquisition between any 2 fidelity models (high/low, high/medium, medium/low) for any group of learners (medical students, trainees, junior physicians, nurses, etc).
Two case-controlled studies (n = 171)15,25 showed no difference in knowledge acquisition between higher and lower fidelity models. Medical students performed no differently on knowledge assessments for ability to list differential diagnoses when using a standardized patient or mannequin.25 Although pretest/posttest TeamSTEPPS Benchmarks scores increased from baseline for both groups of medical students, the gains were not significantly different per fidelity arm of in-person interprofessional group training versus asynchronous individual online training.15
Non-Technical SkillsTwo randomized controlled studies (n = 436)21,28 showed increased nontechnical skills for higher fidelity, and 5 studies (n = 330)19,20,22,23,31 showed no difference for nontechnical skills between higher and lower fidelity models. Nontechnical skills of surgical residents assessed in 3 fidelity models (higher fidelity cadaver, medium-fidelity anatomically enhanced mannequin, and lower fidelity mannequin) showed significant differences between higher/lower and medium/lower models. There was no difference between higher and medium-fidelity models.28 In a study of medical students, evaluators rated the communication skills of virtual reality-trained students significantly higher than computer-based–trained students for scenarios of interprofessional and intercultural communication.21 No difference was found in studies that compared higher fidelity patient simulators and noncomputerized manequins,19,22 higher fidelity patient simulators versus virtual reality,20 standardized patients versus virtual reality,23 or in-person hands-on task trainers versus computer-based training.31
Three case-controlled studies (n = 86)17,24,32 showed no difference for nontechnical skills between higher and lower fidelity models. The quantity of communication events from anesthesiologists to circulating nurses was significantly higher in actual operating room cases (high fidelity) versus 2 models of lower fidelity simulation (crisis and routine scenarios), although no difference was found between the 2 lower fidelity models.32 However, the simulated crisis scenario showed significantly higher percentages of situational information verbalized in 3 of 6 categories versus the real routine operating room cases.32 Health care workers were more likely to propose a medical procedure with an explanation and ask permission before touching a simulated patient than a mannequin.17 Participants were also more likely to talk to a simulated patient than a mannequin, although this finding was not statistically significant (P = 0.125). There were no differences in attitudes toward nontechnical skills among medical students engaging in interactions with a simulated patient either wearing a high-fidelity hyperrealistic suit or not wearing such a suit, although both groups had higher self-assessments than before the interventions.24
Self-Competence/ConfidenceOne randomized controlled study (n = 66)18 showed higher confidence levels with higher fidelity models, and 2 randomized controlled studies (n = 55)28,31 showed no difference between higher and lower fidelity models. Medical students who interacted with higher fidelity mannequins reported higher confidence levels than those students who worked with lower fidelity mannequins.18 Advanced learners, such as residents and working nurses and technologists, showed no difference in confidence levels.28,31 Two case-controlled studies (n = 180)24,25 showed no difference for confidence between higher and lower fidelity models. One study of medical students showed increased mean group confidence preintervention/postintervention with no difference between groups.24 A crossover study of medical students showed increased confidence for all learners after the second scenario, regardless of the scenario order of high to low or low to high.25
Technical SkillsThree randomized controlled studies (n = 73)14,20,28 showed better technical skills for medium or higher fidelity, and 5 randomized controlled studies (n = 561)16,18,19,26,31 showed no difference between higher and lower fidelity models. Technical skills for surgical management demonstrated by surgery residents increased significantly from baseline after either higher fidelity cadaver and medium-fidelity mannequin with enhanced anatomy compared with a lower fidelity mannequin; however higher fidelity was equivalent to medium-fidelity for skills gain.28 Teams that trained with a higher versus lower fidelity mannequin showed significant improved performance in a respiratory scenario at 6 months posttraining.14 Technical skills were significantly lower when using virtual reality compared with a higher fidelity mannequin.20 No difference was shown for studies comparing computer-based activity to virtual reality, mannequins, or didactics plus mannequins.16,18,19,26,31
Indicators of StressOne randomized controlled study (n = 42)29 showed increased indicators of stress with higher fidelity, and 2 randomized controlled studies (n = 116)19,27 showed no difference between higher and lower fidelity models. Stress levels increased significantly for the higher fidelity model with greater perceived workload, and females found the workload conditions to be significantly higher than male participants.29 Regardless of fidelity model, buccal cortisol levels increased significantly over the duration of the simulated experience, and subjective stress increased significantly from baseline to scenario completion.19 Regarding in situ versus off-site simulation, the measurement of salivary cortisol levels, Stress-Trait Anxiety Inventory responses, and cognitive stress appraisals did not differ based on location.27
One case-controlled study (n = 40)24 showed increased indicators of stress for higher fidelity simulation. Medical students reported significantly higher stress levels after higher fidelity scenarios of standardized patients with hyperreactive suits than those without.24
DISCUSSIONTeamwork training is an important aspect of health care education.33 Interprofessional activities in education enhance collaboration and foster a sense of camaraderie among health care professionals. The interaction between professionals from different health care disciplines facilitates learning within their respective fields and promotes synergy during simulation exercises.
One key observation from the review was the significant variation in the instruments and tools used to measure teamwork abilities across the reviewed studies. This heterogeneity makes it challenging to compare teamwork outcomes between the studies. A systematic review conducted to assess the validity of teamwork tools used in simulation-based interprofessional training for health care workers and learners found a wide variety of teamwork measurement tools that were reported and used across studies.34 The authors suggested the validity evidence supporting these various tools was variable and in many instances, tools were being reused across studies without consideration for the population studied. In general, there seemed to be a lack of agreement as to which tools are best for assessing teamwork in interprofessional simulation settings. The authors recommended the importance of considering which teamwork domains were important to be measured bearing in mind that the content of tools and definitions of teamwork seemed to be highly subjective and variable. Several tools were found to have strong psychometric properties, including the Team Emergency Assessment Measure (TEAM) tool,35,36 the Team Performance Observation Tool (TPOT),37 and the Assessment of Obstetrical Team Performance (AOTP) and Global Assessment of Obstetrical Team Performance tools.38
The review went on to recommend that the construction of a framework for the reporting of studies assessing teamwork in simulation-based training could improve the methodological quality of future studies and is an important consideration for future research.34 The authors also recommended that tools should be formed with an understanding of the theory underpinning teamwork models and, when applied in simulation-based interprofessional training, must reflect the specific objectives of the activity. It would therefore be beneficial to establish guidelines for selecting measurement tools in the future or consider adopting a competency framework such as the Interprofessional Education Collaborative (IPEC),39 or the Canadian Interprofessional Health Collaborative (CIHC)40 framework. Such frameworks could provide common reference points for measuring teamwork abilities.
The central question is whether high-fidelity simulation or low-fidelity simulation should be used for team training in health care providers and trainees. In our review, we found limited evidence suggesting a benefit for high-fidelity simulation. One of 5 studies addressing confidence, 3 of the 8 studies addressing technical skills, and 2 of the 8 studies addressing nontechnical skills showed a positive impact for higher fidelity simulation. The remainder of the studies addressing these outcomes showed no significant difference. We found no significant difference in knowledge outcomes and teamwork abilities between lower and higher fidelity simulation. One of the 3 studies addressing stress levels showed increased indicators of stress with higher fidelity training. Although participants generally expressed higher satisfaction with the use of higher fidelity teaching and learning materials, it is important to note that this satisfaction did not have a noticeable impact on overall outcomes in terms of knowledge, skills, or teamwork abilities.
It is crucial to have clear consistency in the definition of high-fidelity simulation, which encompasses the highest level of realism. This can involve a range of approaches including trained actors, advanced mannequins with various physiological features, realistic cadavers, and other sophisticated equipment.
The identified studies indicated that the success of simulation depends on various factors, including costs, technological expertise, equipment quality, available space, and maintenance support. The literature review did not identify any formal cost-comparative studies. It is important to note that high-fidelity mannequins are generally more expensive than low-fidelity ones, considering both initial purchase costs and ongoing maintenance expenses. Moreover, high-fidelity mannequins often require additional personnel to operate and maintain their functionality.
Given that the evidence highlighted in this review shows no difference between high- and low-fidelity simulation for most outcomes, an alternative to high-fidelity simulation could be the combination of low-fidelity technology and in situ simulation. It has been shown that interprofessional activities not only facilitate learning but also have the potential to cultivate long-lasting relationships that can be applied in real-life situations.33
LimitationsA common limitation found in many studies is the lack of standardized definitions and descriptions for low-fidelity and high-fidelity methods and types of simulation. Establishing such standardized definitions would enhance learning outcomes and facilitate consistent evaluation. The variation in measurement methods across studies poses a challenge when attempting to make direct comparisons, whether it is comparing simulation methodologies or assessing teamwork and competency outcomes.
CONCLUSIONS AND FUTURE WORKThe use of either higher or lower fidelity simulation by health care providers and trainees is equally beneficial for team training. If resources permit the use of higher fidelity simulation, then this has been shown to be more popular with participants.
Based on the observations from this review, there are several possibilities for future research. More robust comparative studies are needed to address the paucity of high-quality literature on this important research question. Cost comparisons and analyses are needed to determine the feasibility of different simulation approaches. All of this requires the development of an evaluation framework that provides a standardized format for defining and measuring desirable outcomes in simulation-based interprofessional education.
Addressing these research priorities will contribute to the advancement of simulation-based education and ensure consistent and effective implementation of interprofessional learning experiences.
ACKNOWLEDGMENTSThe authors would like to thank Danielle Gerberi (information specialist) for her help with this review. We would also like to thank the leadership team from the Society for Simulation in Healthcare (Dimitrios Stefanidis, Sharon Decker, Sharon Muret-Wagstaff, David Cook, Mohammad Kalantar, Mohammed Ansari, Kathy Adams, and Kristyn Gadlage) for their support and guidance in this process.
REFERENCES 1. Lioce L, Loprieato J (Founding Ed), Downing D, et al; the Terminology and Concepts Working Group. Healthcare Simulation Dictionary. 2nd ed. Rockville, MD: Agency for Healthcare Research and Quality; 2020. 2. Lefor AK, Harada K, Kawahira H, Mitsuishi M. The effect of simulator fidelity on procedure skill training: a literature review. Int J Med Educ 2020;11:97–106. 3. Norman G. Where we've come from, where we might go. Adv Health Sci Educ Theory Pract 2020;25(5):1191–1201. 4. Norman G, Dore K, Grierson L. The minimal relationship between simulation fidelity and transfer of learning. Med Educ 2012;46(7):636–647. 5. Burke CS, Salas E, Wilson-Donnelly K, Priest H. How to turn a team of experts into an expert medical team: guidance from the aviation and military communities. Qual Saf Health Care 2004;13 suppl 1(suppl 1):i96–i104. 6. Beard RL, Salas E, Prince C. Enhancing transfer of training: using role-play to foster teamwork in the cockpit. Int J Aviat Psychol 1995;5(2):131–143. 7. Hamman W. The complexity of team training: what we have learned from aviation and its applications to medicine. In: Simulation in Aviation Training. Routledge; 2017:451–458. 8. Helmreich RL, Merritt AC, Wilhelm JA. The evolution of crew resource management training in commercial aviation. In: Human Error in Aviation. Routledge; 2017:275–288. 9. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev
留言 (0)