
記住我






Standardized patients (SPs) are extensively used in health care education evaluation and research to portray real patients and simulate symptoms or problems.1 The SPs are frequently used to teach communication skills.2–4 Communication is foundational for ensuring optimum patient health outcomes5,6
Still, there is a dearth of high-quality comparative studies with meaningful outcome measures, providing little evidence to support the effectiveness of SP methodology in teaching communication objectives compared with other modalities.7 Furthermore, recent advancements in manikin-based technology and virtual reality raise questions regarding the superiority of the SP modality in teaching communication skills. Without this information, evidence-based practice guidelines cannot be established to provide educators, researchers, and clinicians the needed recommendations for effective integration and usage of SPs in education and training environments.
The research question guiding this study was, “Among health care professionals, does the use of SP methodology as a means of teaching communication skills result in improved learner knowledge, skills, attitudes, and/or patient outcomes when compared with other simulation methodologies?” The purpose of this review was to search, extract, and synthesize research completed in the last 10 years to report the current state of the science related to the use of SPs in teaching communication skills. This review also sought to identify gaps in simulation-based research in this area.
METHODS Eligibility Criteria and DefinitionsThis review was planned, conducted, and reported in line with Preferred Reporting Items for Systematic Reviews and Meta-Analyses.8 The inclusion criteria were broad to complete a comprehensive search of the literature. For a study to be eligible, it had to:
Be original research that compared simulation using an SP to another simulation methodology. Evaluate communication knowledge, skill, attitude, and/or patient outcome with an academic or practicing health care professional. Meet specific definitions as defined by the Bloom Taxonomy.9 o Knowledge was defined as mental skills.9 o Skills were defined as manual or physical skills.9 o Attitude was defined as growth in feelings or emotional areas.9 o Patient outcomes was defined as end outcomes or the results from some action of event.10The exclusion criteria included narrative reviews, expert opinions, simulation cases, and letters to the editor. Unpublished literature and studies not in the English language were excluded. Studies that did not meet the definitions of the outcome criteria as well as any study that did not specify the SP was formally trained before participating in the simulation were deemed ineligible.
Information Sources and Search StrategyThe literature was searched by a medical librarian for the concepts of communication with standardized patients in a simulation setting. Search strategies were created using a combination of keywords and standardized index terms. Searches were run on October 21, 2021, in CINAHL via EBSCO (1963+), Ovid Embase (1974+) and Ovid Medline (1946+ including epub ahead of print, in-process, and other nonindexed citations), and Scopus (1823+) using a search strategy designed by a research librarian (see Table, Supplemental Digital Content 1, which provides the complete librarian-designed search strategy, https://links.lww.com/SIH/B9). Initially, no beginning date cut-off was used to allow for a broad search.
Selection ProcessThe years of search were limited to 2011–2021 to include articles from the last decade. Three reviewers (T.R.H., A.H., T.P.N.) screened and selected articles for inclusion using an in-depth analysis. Each title and abstract were screened by 2 independent reviewers. A decision to err on inclusion in this initial stage was made before any screening. Then, each full-text article was screened for inclusion by 2 reviewers who worked independently. In cases of disagreement, a third reviewer was consulted as an arbiter who independently screened the article for a final decision.
Data Extraction Process and Data ItemsA data extraction form, used previously by 1 reviewer (T.R.H.), was piloted and revised as needed to extract data for 4 study outcomes: knowledge, skills, attitude, and patient outcomes. Additional data items reported from each article included study design, purpose, number and type of participants, setting, intervention, control, measurement instruments, conclusions, and limitations. Extracted data items were checked by a second reviewer for accuracy, and in the event of a discrepancy, consensus was reached by discussion among all 3 reviewers. There were no missing data from any article and no reviewing tools used for the data items extracted.
Two authors (T.R.H., A.H.) reviewed articles and completed a quality appraisal using the Medical Education Research Study Quality Instrument,11 which evaluated each article based on design, sampling, type of data, validity evidence, data analysis, and outcome. The reviewers were not blinded to the journal name, study title, authors, or institutions. Differences in quality assessment were reconciled between the 2 reviewers.
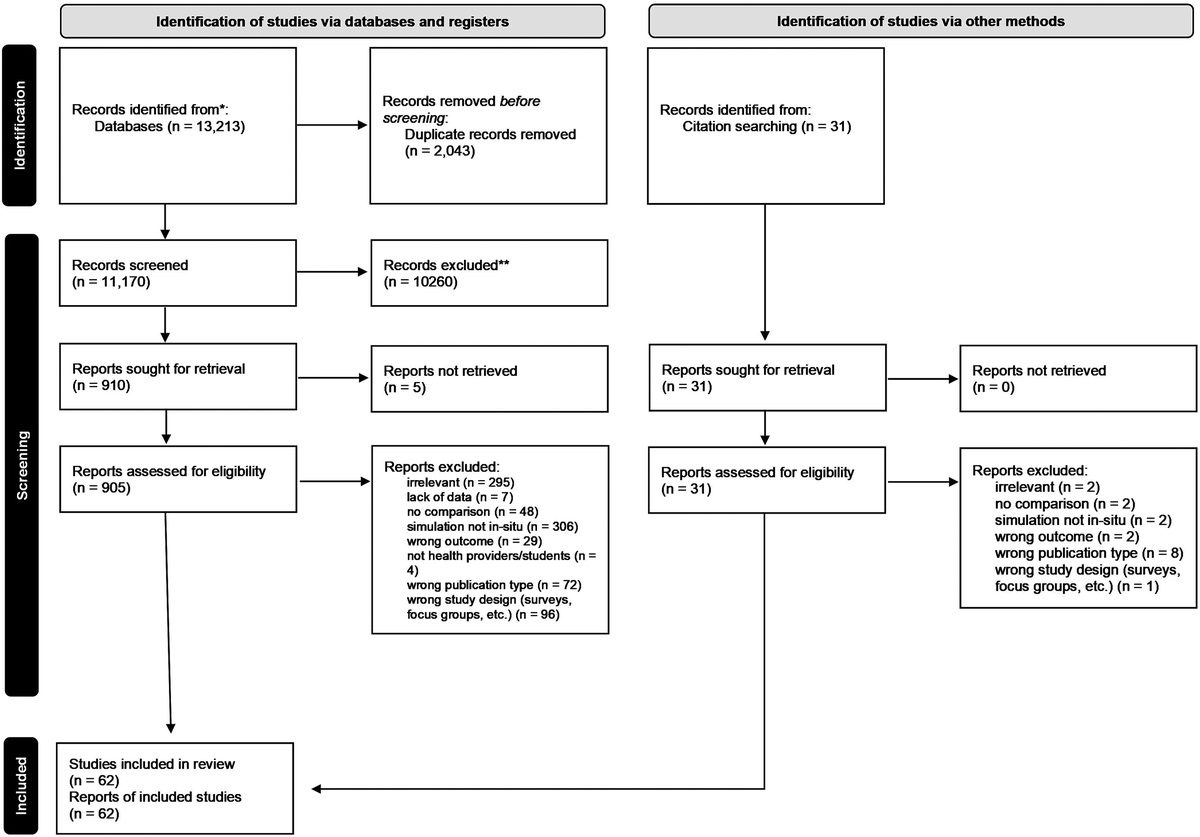
RESULTS Study SelectionThe database search strategy yielded a total of 8058 citations. Deduplication was performed in Covidence, leaving 6606 citations. The results were narrowed to 18 articles. References of the final 18 articles were reviewed for additional studies, but no additional articles were added to the final count. An illustration of study selection is presented in Figure 1.
 FIGURE 1:
FIGURE 1: Flow diagram.
Quality AppraisalIn the 18 articles included for review, the mean Medical Education Research Study Quality Instrument score was 12.5 (range, 9.5–14.5). Only 7 articles were randomized controlled trials (39%). There were no studies conducted at more than 1 institution, and no study reported complete validity evidence (content, internal structure, and relationships to other variables) for their evaluation instruments. Scores of each article are provided (Table 1).
TABLE 1 - Quality Appraisal of Articles Using the Medical Education Research Study Quality Instrument (MERSQI) Article MERSQI Score Agago et al 11.0 Alfes et el 12.0 Aper et al 13.5 Bagacean et al 12.5 Bosse et al 13.5 Coffey et al 11.5 Gillette et al 12.0 Herchenrother et al 13.5 Ignacio et al 14.5 Johnson et al 13.0 Karadas et al 12.5 King et al 12.5 Kleinsmith et al 11.5 Koponen et al 13.0 O'Rourke et al 12.5 Paramasivan et al 9.5 Park et al 13.5 Schlegel et al 12.5The SP methodology was compared with role play (n = 10, 56%), manikin (n = 5, 28%), and virtual SP (n = 3, 17%). Key study characteristics of the 18 individual articles are summarized in Table 2.
TABLE 2 - Study Characteristics by Comparative Simulation Methodology Citation Design Setting (Hospital/unit, country) N/Type of Participants Outcome Measured (K = Knowledge,The SP methodology was compared with role play in 10 (56%) of the 18 studies.12–21 Six (60%) studies used a quasi-experimental design,12–14,16,18,19 and 4 (40%) were randomized controlled trials.15,17,20,21 Eight (80%) studies were conducted in an academic setting.12–16,18,20,21 Most (90%) studies were conducted outside the United States.12–15,17–21 The sample sizes ranged from 15 to 220, and all participants were students from either medicine (n = 7, 70%),12,14,15,17–20 nursing (n = 2, 20%),13,21 or pharmacy (n = 1, 10%).16 No study included interprofessional disciplines.
Outcome MeasuresHalf (50%) of the studies evaluated more than 1 outcome.14,15,17,20,21 Knowledge was evaluated in 3 (30%) studies,13,17,20 and all (100%) used written test questions as the method of evaluation. Skill was evaluated in 8 (80%) studies,12,14–17,19–21 and most (60%) used an Objective Structured Clinical Examination (OSCE) as the measurement instrument.12,15–17,20,21 Attitude was an outcome measured in 5 (50%) studies,14,15,18,20,21 all (100%) of which used a questionnaire as the measurement instrument.
Compared with role play, SP methodology was superior in 1 (33%) study where knowledge was measured.20 The SP methodology was superior to role play in 6 (75%) studies where skill was measured,12,14,16,19–21 whereas SP methodology was superior in only 1 (20%) study where attitude was measured.18 No study evaluated patient outcomes.
ManikinThe SP methodology was compared with a manikin in 5 (28%) of the 18 studies.22–26 Two (40%) studies were randomized controlled trials,23,26 and 3 (60%) were quasi-experimental designs.22,24,25 Four (80%) studies took place in an academic setting,23–26 whereas 1 (20%) study was completed in a hospital.22 The countries in which the studies were completed were England,22 Singapore,23 United States,24 Canada,25 and Turkey.26 The number of participants in the studies varied from 6 to 100. All participants were students in the following disciplines: nursing (n = 5, 100%), medicine (n = 1, 20%), social work (n = 1, 20%), respiratory therapy (n = 1, 20%), and physiotherapy (n = 1, 20%). Only 2 (40%) studies were interdisciplinary.22,25
Outcome MeasuresOnly 1 (20%) study evaluated more than 1 outcome.24 Johnson et al24 measured skills and attitudes. No study evaluated knowledge, but skill was an outcome measure in all studies (n = 5, 100%). Attitude was measured in only 1 (20%) study.24 Skill was measured mostly (n = 3, 60%) by a checklist,23,24,26 whereas attitude was measured by a scale.24 Compared with a manikin, SP methodology was superior in 3 (60%) studies22,24,26 where skill was the outcome measured and in the 1 (100%) study that measured attitude.24 No study evaluated knowledge or patient outcomes with a manikin.
Virtual SPThe SP methodology was compared with a virtual SP in 3 (17%) of the 18 studies.27–29 Only 1 (33%) study was a randomized controlled trial,27 whereas 2 (67%) were quasi-experimental (67%) studies.28,29 All 3 (100%) were completed at a college or university setting with medical students. The sample size ranged from 60 to 196 participants.
Outcome MeasuresOnly 1 (33%) study measured knowledge.27 Two (66%) studies measured skill,28,29 and 2 (66%) measured attitude.27,29 Knowledge was measured using a video case scenario,27 whereas skills were measured using checklists,28,29 and attitudes were measured using scales.27,29 The SP methodology was superior to virtual SP methodology in the 1 (100%) study that measured knowledge.27 Compared with a virtual SP, SP methodology was also superior in 1 study29 where skill was measured (n = 2, 50%). However, virtual SP methodology was superior to SP in both (n = 2, 100%) studies evaluating attitude.27,28 No study using a virtual SP measured patient outcomes.
Table 3 shows the number of times of the number of eligible studies that the SP methodology was better than the comparison simulation methodology (role play, manikin, or virtual SP) by the outcome (knowledge, skills, or attitude) measured.
TABLE 3 - Number of Times Per Number of Studies SP Methodology Was Better Than the Comparison Simulation Method by Outcome Outcome Knowledge Skills Attitude Patient Outcomes Comparison Simulation Method Role play 1/3 6/8 1/5 0/0 Manikin 0/0 3/5 1/1 0/0 Virtual SP 1/1 1/2 0/2 0/0Health care professionals must convey complex medical information, understand patients' needs and concerns, and build trust to ensure the best possible care. However, learning and mastering these skills in a real clinical environment can be challenging because it involves real patients, time constraints, and ethical considerations. Simulation-based training has emerged as a powerful tool to bridge this gap. The choice of simulation modality, whether it be SPs, role play, manikins, or virtual SPs, is pivotal in shaping the quality of this training. The optimal method/modality of teaching communication remains unknown. Overall, there is a lack of research in this area, with only a few randomized controlled trials completed to compare simulation methodologies. Most studies were completed in an academic setting, leaving little known about the use of SPs to teach communication in the practice setting. The sample sizes varied, with many studies failing to state if a power analysis was completed, leaving questions as to whether the findings of the study were genuine or due to chance.
Health care disciplines such as nursing, pharmacy, respiratory therapy, physiotherapy, and social work were minimally represented, whereas occupational therapy, physical therapy, ministry, and patient relations were completely lacking from this review. There is a lack of interprofessional education (IPE), which is surprising but perhaps expected considering the low number of health care disciplines represented overall.
In most studies, SPs were compared with role play. Role play may be a more preferred simulation methodology due to feasibility, especially if students are used. Role play also does not require training. But the exact reasons why it was most often used remain unclear. The SP methodology was superior to role play in knowledge and skills but not attitude. This is a surprising finding considering SPs have been trained to provide feedback and individuals in role play have not. Perhaps the choice of measurement tools used to evaluate attitude was not sensitive enough to detect subtle differences. Alternatively, the training provided to SPs may have focused more on knowledge and skills, potentially neglecting the development of attitudes.
It was an unexpected finding that not all studies found SPs superior to manikins in skills. Manikins communicate using a transmitted human voice that often sounds mechanical to learners. On the other hand, SPs provide regular face-to-face human dialogue, making SPs seem like the more ideal methodology to use for communication. The findings here may suggest differently, but a larger number of studies are needed to know.
The SPs were compared with virtual SPs in the least number of studies. This could be because role play and manikins have existed longer. Researchers have had less time to study the true effects of virtual SPs. Still, no real conclusions can be drawn due to the overall low number of studies (n = 3). Once evidence starts accumulating, it will be essential to continuously evaluate and update the recommendations for simulation modality selection. Health care education is dynamic, and emerging technologies and teaching methods may influence the choice of modalities.
A glaring gap in the literature is the effect(s) of an SP compared with role play, manikin, or virtual SP on patient outcomes. This gap hinders educators in making evidence-based decisions when choosing the optimum simulation modality to enable learners to acquire communication knowledge, skills, and attitudes to improve patient outcomes. Without robust evidence on which simulation modality works best in various contexts, educators may resort to arbitrary choices, potentially missing out on the most effective teaching methods. Researchers should consider not only the effectiveness of training but also the long-term retention of skills and their application in real clinical settings.
No study compared the costs between an SP, role play, manikin, and virtual SP. Although role play may be the least expensive, it may also be the least effective in achieving the stated goal. Although SPs may offer a rich learning experience, they often require ongoing training and compensation. Institutions with more capital may be able to offer a broader range of specific services, assistive technologies, and support staff. As a result, their execution of SP education may be more comprehensive compared with organizations with restricted resources.30 In contrast, manikins or virtual SPs may have a lower initial cost but can incur maintenance and software licensing fees. Health care education institutions often operate under budget constraints. The ability to justify resource allocation for simulation equipment, training, and maintenance is crucial. Evidence-based decision-making can provide insights into not only which modality is most effective but also which represents the best return on investment.
LimitationsThere are several limitations to this systematic review. First, studies not in the English language were excluded, which could have added more scientific merit to the studies included. The inclusion and exclusion of studies were determined by reviewers' judgment. Although efforts were made to ensure consistency through arbitration, some level of subjectivity may have influenced the selection process. The study selection was limited to articles published between 2011 and 2021. Although this timeframe allows for a review of the most recent research, it may exclude older studies that provide important historical context or trends in simulation-based education. The study does not consider potential advances in simulation technology beyond 2021. Rapid developments in virtual and augmented reality, for example, could have significant implications for simulation-based education.
CONCLUSIONIn summary, studies show a weak indication that SP-based education is superior to other simulation methodologies in most contexts. However, more rigorous studies with larger sample sizes, validated instruments, and effects on patient outcomes are needed to definitively determine the optimal method/modality for teaching communication to health care professionals. The gap in evidence-based decision-making for choosing the optimum simulation modality in communication skills training represents a significant challenge for health care educators and institutions. Addressing this gap requires a concerted effort from educators, researchers, and institutions to conduct rigorous studies, share knowledge, and prioritize patient-centered outcomes. By closing this gap, educators can better prepare health care professionals to deliver empathetic, effective, and patient-centered care, ultimately improving the quality of health care delivery and patient outcomes.
REFERENCES 1. Lioce L, Lopreito J, Downing D, et al, eds. Healthcare Simulation Dictionary. 2nd ed. Rockville, MD: Agency for Healthcare Research and Quality; 2020. 2. Kaplonyi J, Bowles KA, Nestel D, et al. Understanding the impact of simulated patients on health care learners' communication skills: a systematic review. Med Educ 2017;51(12):1209–1219. 3. Bearman M, Palermo C, Allen LM, Williams B. Learning empathy through simulation: a systematic literature review. Simul Healthc 2015;10(5):308–319. 4. Pascucci RC, Weinstock PH, O'Connor BE, Fancy KM, Meyer EC. Integrating actors into a simulation program: a primer. Simul Healthc 2014;9(2):120–126. 5. Kwame A, Petrucka PM. A literature-based study of patient-centered care and communication in nurse-patient interactions: barriers, facilitators, and the way forward. BMC Nurs 2021;20(1):158. 7. Rutherford-Hemming T, Alfes CM, Breymier TL. A systematic review of the use of standardized patients as a simulation modality in nursing education. Nurs Educ Perspect 2019;40(2):84–90. 8. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:1–9. 9. Bloom BS, Engelhart MD, Furst EJ, Hill WH, Krathwohl DR. Taxonomy of Educational Objectives: The Classification of Educational Goals. Handbook I: Cognitive Domain. Philadelphia, PA: David McKay Company, Inc; 1956. 10. Lang NM, Marek KD. The classification of patient outcomes. J Prof Nurs 1990;6(3):158–163. 11. Cook DE, Reed DA. Appraising the quality of medical education research methods: The Medical Education Research Study Quality Instrument and the Newcastle-Ottawa Scale evaluation. Acad Med 2015;90(8):1067–1076. 12. Agago TA, Wonde SG, Bramo SS, Asaminew T. Simulated patient-based communication skills training for undergraduate medical students at a university in Ethiopia. Adv Med Educ Pract 2021;12:713–721. 13. Alfes CM. Standardized patient versus role-play strategies: a comparative study measuring patient-centered care and safety in psychiatric mental health nursing. Nurs Educ Perspect 2015;36(6):403–405. 14. Bagacean C, Cousin I, Ubertini AH, et al. Simulated patient and role play methodologies for communication skills and empathy training of undergraduate medical students. BMC Med Educ 2020;20(1):1–8. 15. Bosse HM, Schultz JH, Nickel M, et al. The effect of using standardized patients or peer role play on ratings of undergraduate communication training: a randomized controlled trial. Patient Educ Couns 2012;87(3):300–306. 16. Gillette C, Rudolph M, Rockich-Winston N, Stanton R, Anderson HG Jr. Improving pharmacy student communication outcomes using standardized patients. Am J Pharm Educ 2017;81(6):1–8. 17. Herchenröther J, Tiedemann E, Vogel H, Simmenroth A. Which teaching method is more effective in a communication course—role-playing versus simulated patients, taught by tutors or faculty staff? A randomized trial. GMS J Med Educ 2021;38(3):1–18. 18. Koponen J, Pyörälä E, Isotalus P. Comparing three experiential learning methods and their effect on medical students' attitudes to learning communication skills. Med Teach 2012;34(3):e198–e207. 19. Paramasivan A, Khoo D. Standardized patients versus peer role play—exploring the experience, efficacy, and cost-effectiveness in residency training module for breaking bad news. J Surg Educ 2019;77(2):479–484. 20. Park KY, Park HK, Hwang HS. Group randomized trial of teaching tobacco-cessation counseling to senior medical students: a peer role-play module versus a standardized patient module. BMC Med Educ 2019;19(1):1–9. 21. Schlegel C, Woermann U, Shaha M, Rethans JJ, van der VC. Effects of communication training on real practice performance: a role-play module versus a standardized patient module. J Nurs Educ 2012;51(1):16–22. 22. Coffey F, Tsuchiya K, Timmons S, Baxendale B, Adolphs S, Atkins S. Simulated patients versus manikins in acute-care scenarios. Clin Teach 2016;13(4):257–261. 23. Ignacio J, Dolmans D, Scherpbier A, Rethans JJ, Chan S, Liaw SY. Comparison of standardized patients with high-fidelity simulators for managing stress and improving performance in clinical deterioration: a mixed methods study. Nurse Educ Today 2015;35(12):1161–1168. 24. Johnson KV, Scott AL, Franks L. Impact of standardized patients on first semester nursing students self-confidence, satisfaction, and communication in a simulated clinical case. SAGE Open Nurs 2020;6:1–7. 25. King J, Beanlands S, Fiset V, et al. Using interprofessional simulation to improve collaborative competences for nursing, physiotherapy, and respiratory therapy students. J Interprof Care 2016;30(5):599–605. 26. Karadas MM, Terzioglu F. The impact of the using high-fidelity simulation and standardized patients to management of postpartum hemorrhage in undergraduate nursing students: a randomized controlled study in Turkey. Health Care Women Int 2019;40(5):597–612. 27. Aper L, Reniers J, Koole S, Valcke M, Derese A. Impact of three alternative consultation training formats on self-efficacy and consultation skills of medical students. Med Teach 2012;34(7):e500–e507. 28. Kleinsmith A, Rivera-Gutierrez D, Finney G, Cendan J, Lok B. Understanding empathy training with virtual patients. Comput Hum Behav 2015;52:151–158. 29. O'Rourke SR, Branford KR, Brooks TL, Ives LT, Nagendran A, Compton SN. The emotional and behavioral impact of delivering bad news to virtual versus real standardized patients: a pilot study. Teach Learn Med 2020;32(2):139–149. 30. Chua WL, Rahim NRBA, McKenna L, Ho JTY, Liaw SY. Intraprofessional collaboration between enrolled and registered nurses in the care of clinically deteriorating ward patients: a qualitative study. Aust Crit Care 2022;35(1):81–88.
留言 (0)