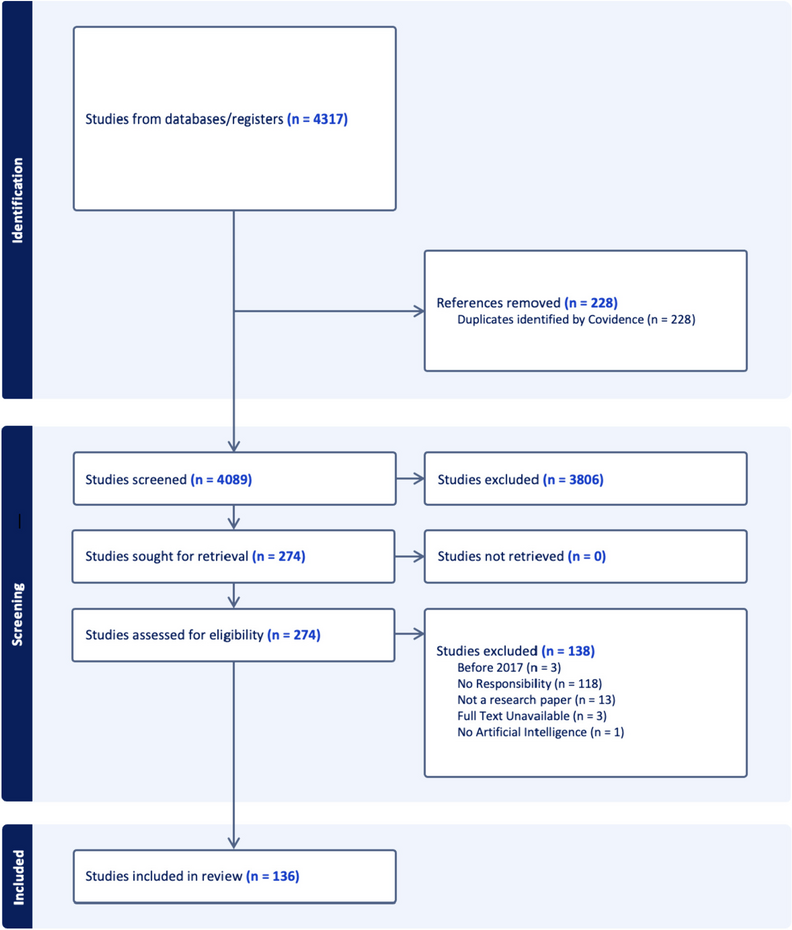
The majority of court cases examined in this study comprised situations in which the man and woman were in conflict over the use or disposal of a gamete. The exceptions included case E, which related to postmortem conception, and cases G and H, which involved procedural errors by a medical institution. Moreover, cases C and D, which resulted in the birth of a child, raise important questions regarding the recognition of a legal parent–child relationship between the male partner who did not consent to the embryo transfer and the child that was born.
These results suggest that carefully considering the role of the male partner’s consent is necessary to minimize conflict in ART procedures. We believe that minimizing such conflict is important for protecting the rights of both women and men, as well as for avoiding complications related to the legal status of the unborn child. We discuss these issues below, along with the contextual background that contributes to the lack of male consent.
Implications for the Reproductive Rights of the Male Partner as a Result of Lack of Consent
As aforementioned, Japanese guidelines on ART stipulate that consent by the male partner is required for every thawed embryo transfer. However, our results show that there are cases where this consent is not always obtained. Furthermore, Japanese courts do not require the consent of the male partner when determining the legal parent–child relationship of a child born through ART. Thus, the male partner would be obligated as a legal parent if a child is born using his gametes, even if he is not at all involved in the thawed embryo transfer. Does this not constitute an infringement on the reproductive rights of the male partner? This proposition requires a clarification of what exactly men’s reproductive rights are.
As explained by the Programme of Action from the International Conference on Population Development (1999), reproductive rights “recognize the right of all couples and individuals to be free and responsible for determining the number, spacing, and timing of their children, and to have the information and means to do so, as well as the right to the highest possible standard of sexual and reproductive health”. The right to decide with whom to have a child can be considered an aspect of reproductive rights. While this applies to both men and women, the focus of reproductive rights is often centered on women (Culley et al. 2013), particularly in terms of women’s fundamental human rights; it is often questioned whether the right to “bear a child or not” is a direct reproductive right of men (Tsuge 2000; Tsujimura 2021). This is for several reasons, including the notion that womenFootnote 8 are often the ones who bear a greater physical burden (e.g., pregnancy and childbirth), as well as the persistence of widespread inequality between men and women in many parts of society. In particular, intense debate on the right to abortion has further highlighted the clear need to protect women’s reproductive rights.
However, while abortion involves procedures that directly affect the woman’s body, the male partner’s refusal to consent to the transfer of embryos does not. Furthermore, the tendency to view reproduction, contraception, and childbirth as inextricably linked with women leads not only to an unequal burden of reproductive responsibility, but also to the marginalization of the role of the male partner in parenthood and the violation of the reproductive right to decide whether to have children (Annandale and Clark 1996). In other words, efforts to protect women’s reproductive rights should not come at the cost of overlooking men’s reproductive rights. Furthermore, the inclusion of discourse on men’s reproductive rights is an important aspect of protecting the rights of both women and men, as well as avoiding complications regarding the legal status of the unborn child.
The decisions of the court cases analyzed in this study indicate that transferring embryos without consent violates the male partner’s right to self-determination. In civil case [D], the court held that the man’s “right to self-determination as to whether or not to have a child with the said woman [ex-wife]” existed and was violated. It was stated that “because bearing and raising children is a fundamental part of the right to personal survival for those who wish to do so, the right to decide whether or not to bear and raise children should be respected as a right that constitutes a component of personal rights in light of the legal intent of Article 13 of the Constitution, which guarantees the right to the pursuit of happiness.” Several other court decisions have also held that “whether or not to bear and raise children” falls within personal rights, regardless of gender (Sendai District Court 2019). This can be interpreted to include the “right to not bear and raise children,” that is, the right of a male partner to “not desire a pregnancy (by means of a fused embryo transfer)” with the woman in question, as a subject of legal protection.
The concept of the male partner’s right to choose whether to have a child is not unique to Japan. In the USA, there is active debate about whether the rights of an individual that does not wish to become a genetic parent of a child born from frozen embryos should be recognized (Cohen 2008). The European Court of Human Rights has also dealt with a case in which the man sought to dispose of embryos after the end of the couple’s relationship and the woman sought an injunction against it (European Court of Human Rights 2007). In this case, the woman had her ovaries removed after the frozen embryos were created, meaning that if the frozen embryos were discarded, the woman in question would lose any means to have biological children. However, while noting the woman’s plight, the court stated that the rights both “to be a parent” and “not to be a parent” must be respected and allowed the man to request the disposal of the frozen embryos. This statement shows consideration of the reproductive rights of the male partner “not to be a parent”: What is protected here can be understood to be the right of the male partner to self-determination.
Furthermore, a case resulting in the birth of a child and recognition of the legal parent–child relationship without consent can be considered a violation of the right to self-determination, not only as a personal right, but also as a property right (Osaka Family Court 2019). Some countries have planned for such situations and have stipulated laws in advance. For example, regarding the use of frozen embryos after divorce, the Uniform Parentage Act of 2000 in the USA specifies “that the former spouse shall not be the parent in the event of divorce prior to conception, unless otherwise expressly agreed.” This law states that a man has neither rights nor obligations as a legal father. However, in countries and regions where there is no such legal provision, if the male partner is recognized as the legal father of the child, he bears the financial burden of child support and other support obligations. The child would also be entitled to inheritance rights. Both issues can have a significant influence on a man’s life for a long period after the child is born. While there are numerous situations in which the reproductive rights of women have not yet been secured, failing to protect the reproductive rights of men also has significant consequences.
Significance of Consent: Does Consent for Frozen Embryo Creation not Include Consent for Embryo Transfer?
There is a suggestion that additional consent at the time of embryo transfer is not necessary in ART procedures. It has also been suggested that consent for the birth of the child is implied at the time of the initial consent for embryo creation (Inaba 2021). However, there are two main reasons for requiring additional consent at the time of transferring frozen embryos.
First, ART procedures are a “medical intervention,” and frozen embryo creation is a medical treatment for both the female and the male partner. Article 6 of the Universal Declaration of Human Rights on Bioethics and Human Rights states that “any preventive, diagnostic, and therapeutic medical intervention is only to be carried out with the prior, free, and informed consent of the person concerned, based on adequate information” (UNESCO 2005). The consent should, where appropriate, be expressed and may be withdrawn by the person concerned at any time and for any reason without disadvantage or prejudice. Consent for medical intervention must be free, explicit, and revocable. Furthermore, considering the time gap between the separation of the gametes from the body and embryo transfer, it follows that individual consent is required even at the time of embryo transfer.
Second, the consent obtained at the time of frozen embryo creation differs from the consent obtained at the time of embryo transfer. In other words, the male partner’s consent at the time of frozen embryo creation can be considered as consent to the medical treatment of separating gametes from the body and creating a frozen fertilized embryo. Certainly, frozen embryo creation is performed with the initial intention of having a child; however, there is no possibility of pregnancy or birth if the embryo remains frozen (Purvis 2021). In contrast, embryo transfer is a specific medical treatment that leads to pregnancy and childbirth. The consent by the male partner at this point can be defined as the desire or willingness to allow the gamete to be implanted into the woman’s uterus, resulting in pregnancy and delivery. This is different from the purpose of obtaining consent for frozen embryo creation.
Examining examples from other countries reveals that in some cases, such as Italy (Italian Constitutional Court 2023),Footnote 9 the withdrawal of consent by the male after fertilization is restricted. In other cases, there are disputes over interpretations of the time length that consent can be withdrawn. For example, in Switzerland the consent of both partners is required for reactivation of cryopreserved fertilized eggs, but it has been interpreted that withdrawal of consent by the male partner is not possible after reactivation of the cryopreserved fertilized eggs for transfer (Ministry of Justice Japan 2021). However, the two points discussed above suggest that the male partner should be allowed to withdraw his consent for the use of embryos after their creation.
Background to the Male Partner’s Absence from Medical Practice
To protect the right of the male partner to self-determination regarding “whether or not to become a parent,” their consent must be reaffirmed at the time of “embryo transfer.” This requirement is clearly stated by Japanese guidelines. However, as shown in some of the cases reviewed in this study, consent from the male partner is not always confirmed at the time of transplantation (cases C and D). The common factor in all of these cases is that the male partner was physically absent when the treatment was performed in medical institutions. Such treatments include sperm collection by the institution (cases A and B) and embryo disposal (cases G and H). For example, when one woman received a thawed embryo transfer in the hospital, her male partner was not present. In another case, it was the woman who brought her male partner’s sperm to the hospital and prepared the documentation for sperm disposal. These cases suggest that Japanese men have the tendency to think of ART as an issue not directly related to them.
Despite the lack of male partners’ presence at the medical institution, ART treatments continue. This is remarkable considering that under normal circumstances, it is impossible for a procedure to proceed without a patient being present at the medical institution. Why, then, does this occur only with ART? One reason could be that ART treatment, which is performed to achieve pregnancy, primarily affects women: The average duration of medical facility visits required for ART procedures is 6–12 days for women and only 0–1 day for men (MHLW 2018).
Another factor is medical institutions’ approach to infertility treatment. Previous studies have suggested that medical institutions in Japan tend to perceive infertility as the woman’s problem (Abe and Tomita 2002), and information that should be explained directly to men is sometimes handled by the woman. A Japanese survey reported that in situations where sperm test results are received at an obstetrics and gynecology medical institution, the husband is not present in about half of the cases; instead, the wife receives an explanation from the doctor alone (MHLW 2016). In any other type of medical practice, it would be highly unusual for a stranger (the wife) to be the recipient of an explanation about another patient’s (the husband’s) medical treatment. Even in male infertility treatment, doctors tend to focus more attention on the female rather than the male partner, with the female partner usually more actively involved in the treatment (Takeya 2021b). Based on the perception that infertility treatment is for women, medical institutions themselves give priority to the female partner.
This perception is rooted in deeper societal gender norms, especially in Japan where the work environment perpetuates a traditional gender role division. According to a study published by the OECD in 2020, the gap between paid work time for men versus women in Japan is 1.7 h, which is the highest gap of all countries surveyed. Gender norms and traditional understandings of the division of labor can contribute to the perception that there is no need for men to be involved in ART procedures.
The Male Partner’s Will and Initiative
In addition to the aforementioned factors, the problem of the lack of male consent can also be linked to a lack of awareness amongst men regarding their agency in ART procedures. Japanese surveys have shown that some male parties do not consider fertility treatment to be a problem directly related to them (Takeya 2021a, b). Similarly, cases C and D can also be considered an example of the male partners’ failure to express their intentions to be involved. If the male partners in these cases had requested that the medical institutions prohibit the use of the frozen embryos when the couples’ relationship came to an end, the medical institutions would not have been able to perform the embryo transfer, and the children would not have been born against the will of the male partners. In these cases, the male parties failed to express their desires, despite the fact that they had the “privilege [unlike in the instance of natural pregnancy] of being able to stop ART without harming the woman’s body before embryo transfer and pregnancy” (Inaba 2022).
What then lies behind the lack of the male party’s proactiveness? One factor is that pregnancy and childbirth are physically related to women. Another possible factor is the lack of discussion on what rights are granted to the male party, the “non-childbearing sex,” in reproductive situations in the first place.
Men, who are indispensable to reproduction, should be granted the right to self-determination in the area of sex and reproduction to the extent that it does not infringe upon women’s rights. The specifics of this right to self-determination have not been adequately discussed. However, with the recent development of ART, there are now options for pregnancy and childbirth that did not previously exist, and men are increasingly making reproductive decisions without infringing on women’s rights. For example, in the case of natural conception, it is unacceptable for a man to ask a woman to terminate her pregnancy once she becomes pregnant as this would force her to undergo an abortion procedure, which is a surgical invasion of the body. However, as abovementioned, in ART, there is an opportunity to stop the procedure by way of non-consent to transplantation without directly violating the woman’s body. Other examples of situations in which the man’s will is an issue include whether a couple wishing to have a baby should undergo treatment when the man is the cause of infertility or whether they should choose artificial insemination with donor sperm when artificial insemination with their male partner’s sperm is not an option. Furthermore, what is the position of the male partner in preimplantation diagnosis for selecting embryos that are free of genetic diseases? Moreover, how is a man involved in whether to undergo prenatal diagnosis for the fetus? These considerations are all directly or indirectly connected to a male party having or not having a child and are considered to be important issues concerning the personal interests of the male party concerned.





留言 (0)