Pointers of Genetic Susceptibility in an Infant with Pulmonary Tuberculosis
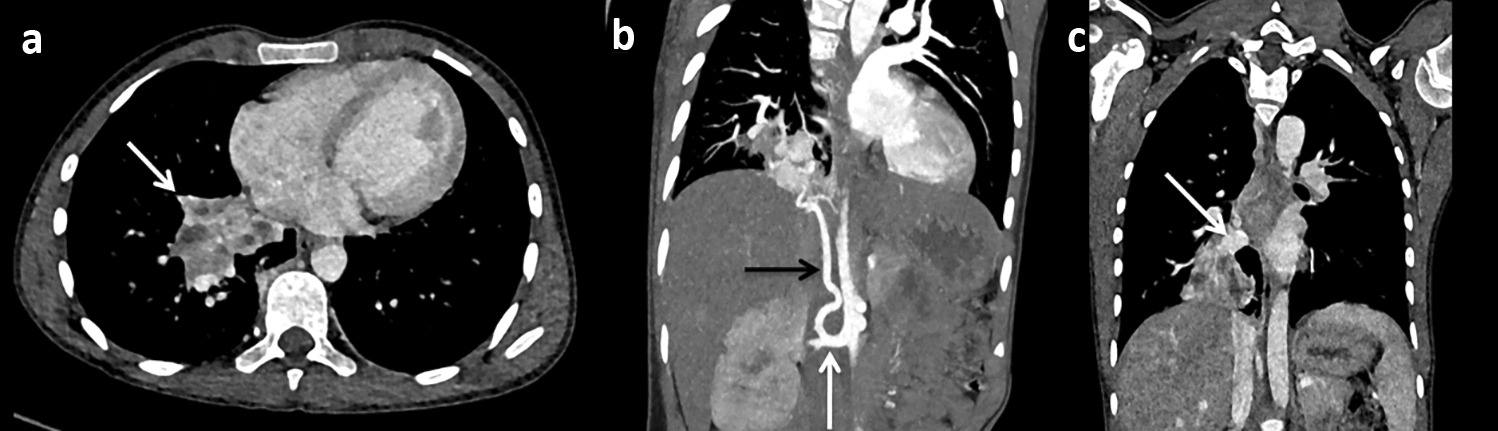
To the Editor: An 8-mo-old boy, a diagnosed case of pulmonary tuberculosis (PTB) presented with features of foreign body; reduced movement and chest expansion on left side with hyperinflation, hyper-resonance notes and crepitation. He had a history of contact with active case of PTB (Grandmother & elder cousin brother). Child received intensive phase anti-tubercular treatment (ATT) for 3 mo. Computed tomography (CT) of chest showed soft tissue density lesions with central necrosis in B/L hilar & para-tracheal lymph nodes with peripheral calcification and soft tissue density lesion in the left main bronchus with hyperinflation of left lung fields. Three samples at different time intervals; two gastric aspirates and one bronchio-alveolar lavage (BAL) fluid revealed acid fast bacilli (AFB) stain and cartridge based nucleic acid amplification test (CBNAAT) positive mycobacterium tuberculosis sensitive to rifampicin and the Lowenstein-Jensen culture was negative. A heterozygous missense variation in exon 7 of the TYK2 gene (chr19:g.10365853C>A;Depth:212x) that results in the amino acid substitution of Histidine for Glutamine at codon 225 (p.Gln225His;ENST00000525621.6) was found. Infant was discharged on three drug ATT and nutritionally recovered with complete resolution of radiological findings at completion of ATT.
Mendelian susceptibility to mycobacterial disease (MSMD) is an inborn error of immunity (IEI) [1]. The susceptibility of infection in MSMD varies from isolated infection of mycobacterium tuberculosis (MTB) or Bacilli Calmette-Guerin (BCG) to concomitant infection with viral and fungal agents. A retrospective cohort of 55 MSMD patients from 10 centers across India reported by Taur et al. revealed clinical, immunological, and molecular characteristics and 17 mutated genes [2]. Persistent CBNAAT and AFB positivity, large granulomatous mediastinal lymph node, strong family history of PTB, delayed response to ATT and large BCG induration and subsequent left axillary adenitis and TYK2 gene mutation suggested genetically predisposed infant for low or high virulent MTB, BCG vaccine and secondary infection. CT scan thorax and bronchoscopy have a diagnostic role in mediastinal and endo-bronchial PTB as demonstrated in the present case [3, 4].


留言 (0)