
記住我










Objectives: To study the mechanisms of injury, clinical manifestations, radiological findings, management, and outcomes of traumatic retropharyngeal hematoma (RH).
Methods: We used the Preferred Reporting Items of Systematic Reviews guidelines to carry out a systematic literature review to identify all published cases of traumatic RH by searching the PubMed database. Articles published between 1988 and 2022 that reported traumatic RH were included. However, articles that reported non-traumatic RHs and non-English articles were excluded from this study.
Results: Of the 62 articles screened, 56 were included. Most patients (55%) were above the mean age of 61.7. The majority of patients were male (69.7%). The main symptom was dyspnea (66.6%) and symptoms usually presented within 24 hours. Among the patients, 90.9% did not take anticoagulants or have coagulation disorders, and the main injury mechanism was falling (54.5%). Most of the computed tomography findings reported retropharyngeal (38%) and prevertebral (15%) hematoma. Meanwhile, magnetic resonance imaging revealed 2 masses in the retropharyngeal space and 2 RHs. With several treatment modalities, more than 50% of the cases were only observed (44 cases), and endotracheal intubation was the most commonly used airway management method (n=35).
Conclusion: Traumatic RH is often caused by falls, particularly in elderly patients. Dyspnea is the primary symptom, usually appearing within 24 hours. Cervical vertebral fractures are the leading cause, and observation is the most common treatment approach.
PROSPERO Reg. No.: CRD42022349010
Keywords:Retropharyngeal hematoma (RH) is a potentially fatal condition where the airway is entirely blocked by the expanding hematoma.1-8 It may be noticed in a variety of ways based on their size and rate of emergence.9-13 The deep and medium layers of the cervical fascia are separated by the retropharyngeal space, which extends from the base of the skull to the superior mediastinum at the level of the second thoracic vertebra. Blood entering this area is what causes RH.11 It can be brought on by a number of conditions, including infection, severe vascular damage, cervical spine fracture, forceful head movements, metastasis, parathyroid adenoma hemorrhage, iatrogenic injury, and ingestion of a foreign material.14-23
Spontaneous RH is an uncommon type of RH that arises without a known cause.8,19,21,24,25 Particularly, anticoagulation therapy or hemorrhagic diathesis may predispose individuals to RH.26,27 Retropharyngeal hematoma is frequently found in trauma patients, particularly those with cervical injuries. According to Penning et al,28 the prevertebral gap is wider in 60% of individuals with cervical injury. However, RH only causes airway obstruction in 1.2% of patients.29 Predominantly, traumatic RH occurs after a cervical vertebral fracture and is generally higher than C6.30-34 According to one research, the most common RH-related injuries included skull fractures, rib fractures, long bone fractures, mandibular fractures, thoracic aortic dissection, lung contusion, brachial plexus damage, and cranial nerve VI palsy.35
Initial symptoms include pharyngitis, dyspnea, odynophagia, and dysphagia (which can occur alone or in various combinations) while bruising, pain, and increasing neck swelling can occasionally clarify the diagnosis. Cervical trauma frequently happens in patients for a number of causes, from severe car accidents to minor falls.9-13 However, RH is typically difficult to diagnose owing to its scarcity and lack of distinct indications and diagnostic laboratory evidence in the majority of patients.19,20,24 Patients with RH have a fair prognosis for recovery, with only a few reported cases of fatal outcomes.5,36,37 The first step in clinical care is securing a patient’s airway, followed by clinical examination and radiographic investigations to obtain a diagnosis. Treatment is determined by the size and clinical course of the hematoma.38 This study aimed to investigate the mechanism of injury, clinical presentation, radiological findings, management, and outcomes of traumatic RH.
MethodsThis study was designed in accordance with the Preferred Reporting Items of Systematic Reviews (PRISMA) criteria for recommended reporting items for systematic reviews and meta-analyses. We searched the PubMed database, supplemented by manual reference searches for all published research articles, using the following keywords: [(“traumatic retropharyngeal hematoma”) AND (“case report”)] and [(“retropharyngeal hematoma”) AND (“case report”)] and (“fall”) and [(“retropharyngeal hematoma”) AND (“case report”)] AND (“accident”)] and [(“traumatic retropharyngeal hematoma”) AND (“motor vehicle collision”)] to decrease the possibility of missed cases. The search was carried out by 7 investigators. We included all studies published between 1988 and 2022. We excluded: I) non-English studies; II) systematic reviews, review articles, and randomized control trials; and III) spontaneous and non-traumatic RH. The following data was independently gathered by 4 authors from the included studies: author, publishing year, age, gender, anticoagulation/coagulopathy, mechanism of injury, presenting symptoms, time from injury to symptoms (hours), associated injuries, associated findings in computed tomography (CT) scan, associated findings on magnetic resonance imaging (MRI) scan, techniques for controlling airways, treatment modality, acute complication, The reason of death, and intensive care unit (ICU).
ResultsA total of 62 articles were identified using PubMed (Figure 1), and the manual reference search yielded 21 additional articles. After excluding 3 duplicate papers, 80 were reviewed by title and abstract. A total of 9 records with apparently non-traumatic or irrelevant subjects and 3 records with no abstract were removed. We evaluated the remaining 68 articles according to the eligibility criteria. The following factors led to the exclusion of another 12 articles: insufficient information (n=8) and in languages other than English (n=4). Finally, a total of 56 articles were included (Figure 1).
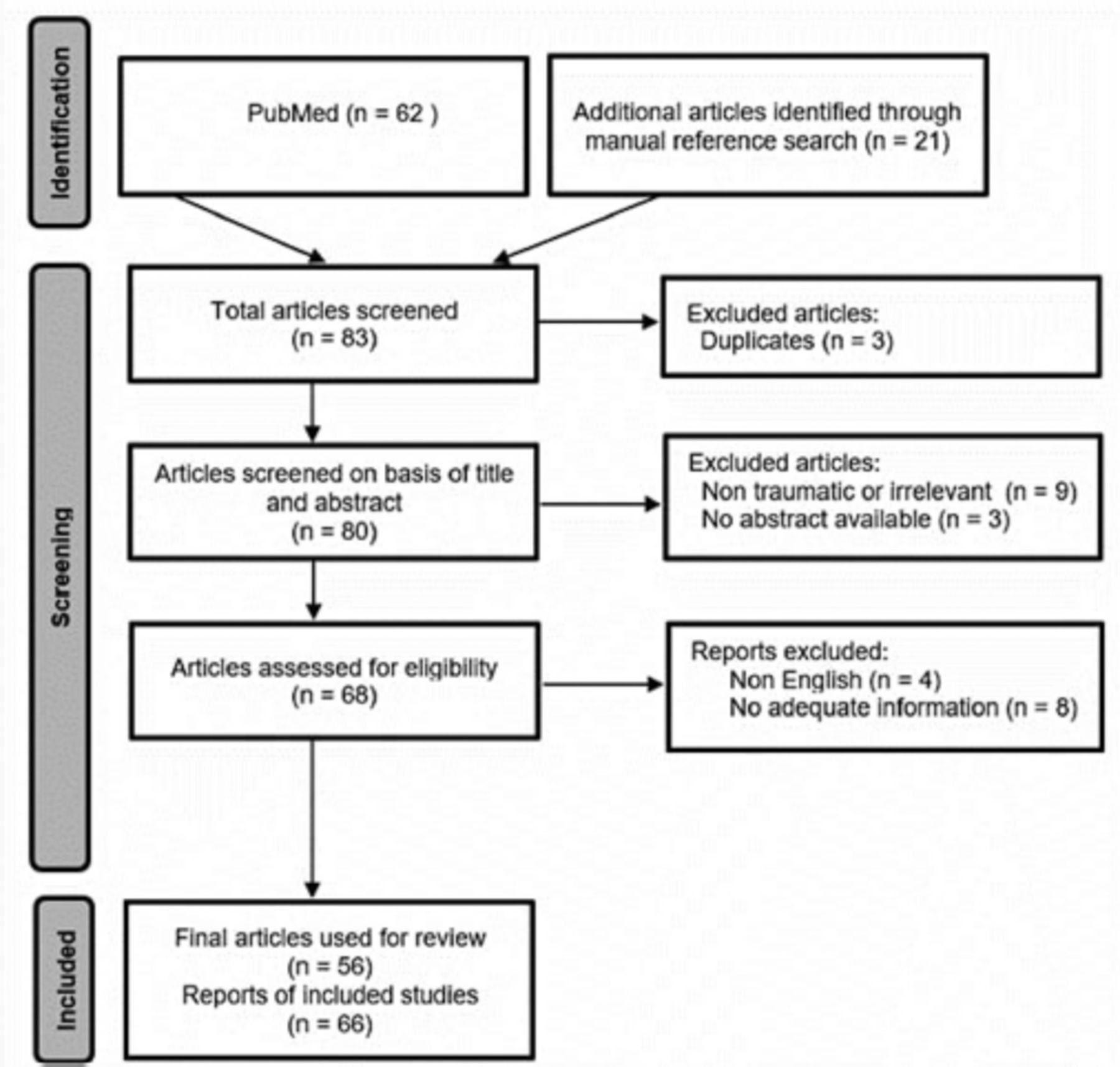 Figure 1
Figure 1 - The Preferred Reporting Items of Systematic Reviews guidelines flow diagram.
Patients ranged in age from 4-94 years (median: 68 years). Most patients (56.5%) were above the mean age of 61.7. Furthermore, in line with the patterns observed in most trauma reports, there was a clear male predominance among patients diagnosed with traumatic RH, with males accounting for 69.7% of the cases compared to females, who accounted for 30.3%. Most patients (90.9%) were not taking anticoagulants or diagnosed with coagulation disorders, but 9.1% were taking warfarin or heparin. The main injury mechanism was falls (54.5%), followed by traffic accidents (34.8%). Common symptoms of RH were dyspnea (66.6%), dysphagia (31.8%), neck swelling (31.8%) and pain (30.3%), stridor (25.7%), hoarseness (22.7%), altered mental status (18.2%), and cyanosis (12.1%, Figure 2). Where time to symptoms was recorded, symptoms presented within the first 24 hours (Table 1).
 Figure 2
Figure 2 - Common symptoms for patients with traumatic retropharyngeal hematoma.
Table 1- Characteristics of the included patients in reviewed articles.
A total of 52 articles reported radiological CT findings and found the following number of cases: hypoattenuating retropharyngeal collection (n=1, 2%), prevertebral soft tissue swelling (n=10, 15%), prevertebral hematoma (n=10, 15%), cervical fractures (n=9, 13%), occipital condylar fractures (n=2, 3%), retropharyngeal soft tissue swelling (n=4, 6%), RH (n=26, 38%), a pharyngeal mass (n=5, 7%), and cervical spondylosis (n=1, 2%, Table 2).
Table 2- Radiological findings of reported cases of RPH.
Out of 12 articles that used MRI, one showed a low-signal retropharyngeal collection on T1, 2 showed a low-signal mass in the retropharyngeal space, and one showed a slightly high-signal at C4 and C5. On T2, one showed a high-signal retropharyngeal collection and one showed a heterogeneous mass along the retropharyngeal space, 2 RHs, one retropharyngeal swelling, and one tearing of the anterior longitudinal ligament at C4-5 level (Table 2).
Several treatment modalities were reported: the majority of cases were only under observation (n=44, 63.8%), followed by surgery (n=13, 18.8%), percutaneous aspiration (n=7, 10.1%), and transcutaneous arterial embolization (n=5, 7.2%). Of the 69 cases, only 16 (23%) cases were admitted to the ICU. There were 8 (11.6%) cases of mortality due to multiple system organ failure (n=5, 7.2%), hemodynamic instability (n=1, 1.4%), or withdrawal of life support (n=2, 2.9%, Figure 3).
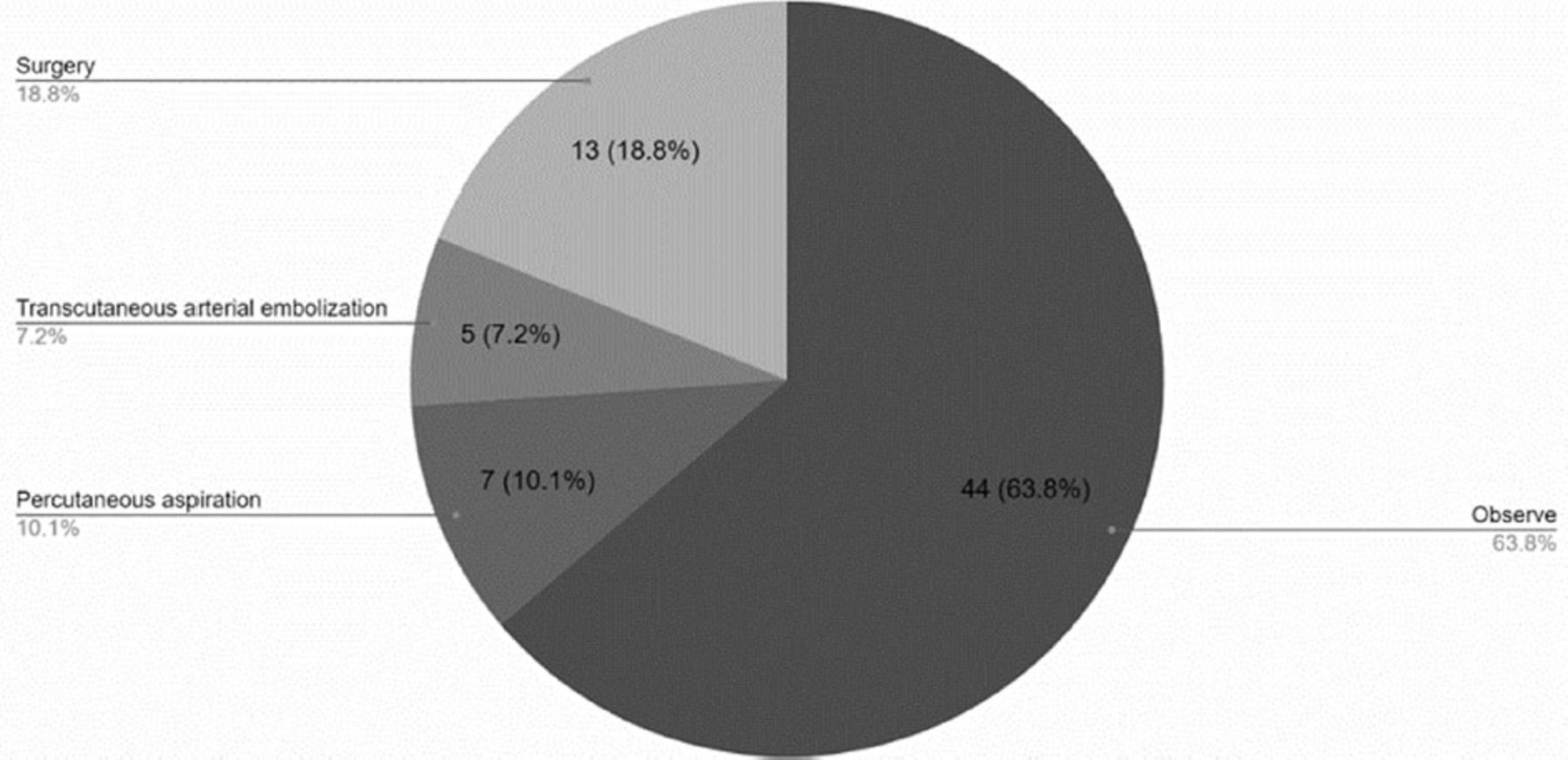 Figure 3
Figure 3 - Treatment modalities.
Only 12 (17.4%) patients suffered from acute complications including pneumonia, pulmonary edema, type 2 respiratory failure, mucosal and submucosal edema of the pharyngeal wall, months of difficulty swallowing, anoxic brain damage, venous thrombus, and stroke.
The most common first option airway management procedure was endotracheal intubation (n=35, 50.7%), which failed in 16 (23.2%) cases (Table 3).
Table 3- Managements and its outcomes.
Tracheostomy was also a first-option procedure (n=7, 10%) but more often used as a second option (n=12, 17.4%) when endotracheal intubation was unfeasible. Cricothyroidotomy was used in only 4 (5.8%) cases, and 8 (11.6%) underwent none of the aforementioned airway management procedures (Figure 4).
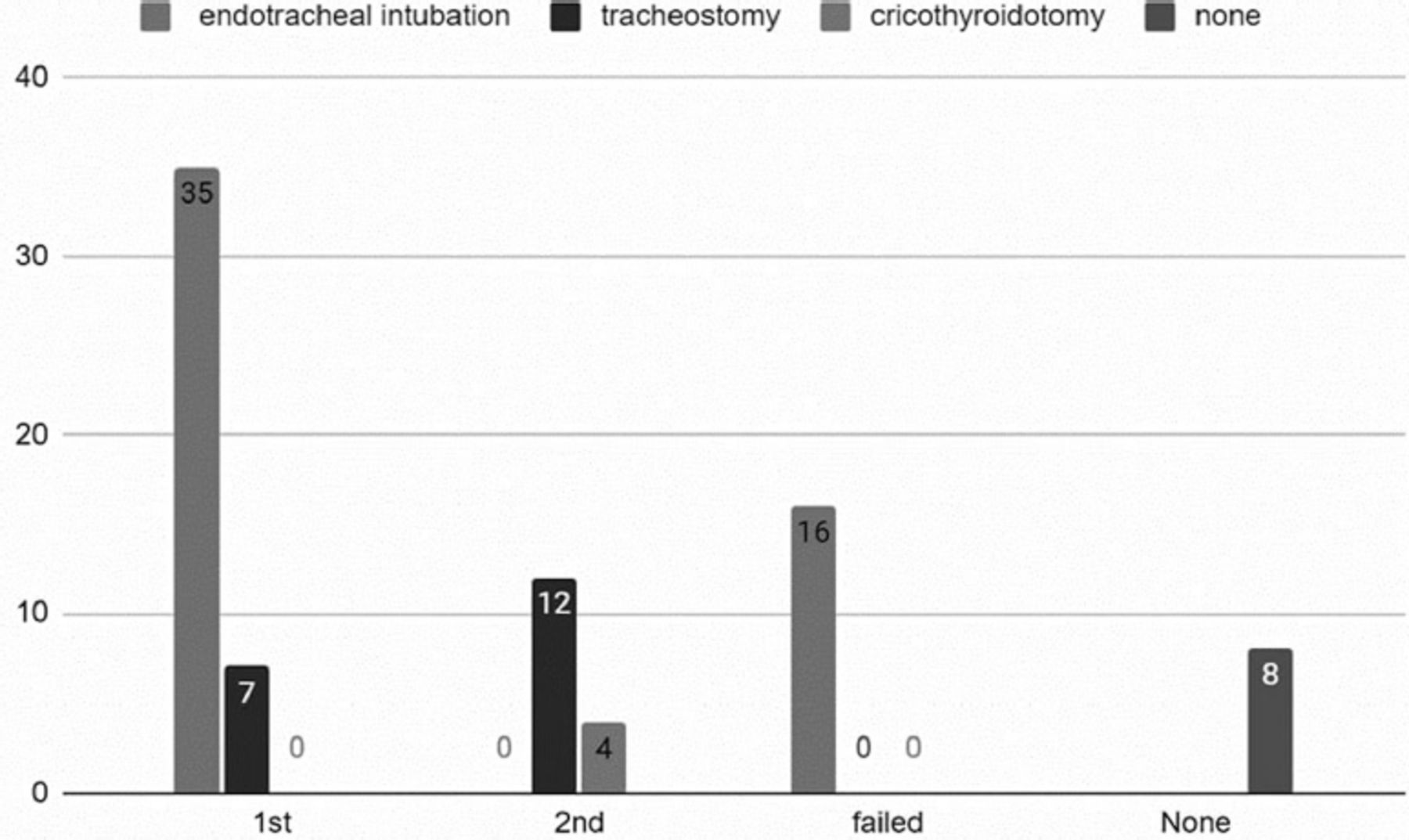 Figure 4
Figure 4 - Patient’s airway management.
DiscussionRetropharyngeal hematomas are life-threatening conditions due to the possibility of progressive obstruction of the upper airways. A spontaneous unprovoked bleeding is highly unusual, and the condition is often associated with underlying conditions such as cervical spinal cord injury, trauma with or without bone damage, and neck surgery. The primary strategy is to protect the airway and to provide intensive care.
In many cases, patients with spinal cord injuries and fractures are suffering from RH, and their clinical course and outcome are determined by the primary injury they have sustained. As a result, the natural clinical course of RH remains unclear.88
Demographics and causesTraumatic RHs are most commonly caused by cervical vertebral fractures, and are generally higher than C6.12,29,89,41,42 According to one study Tsao et al,35 the most common injuries were cervical spinal injuries, traumatic brain injuries, long bone fractures, mandibular fractures, lung contusion, brachial plexus injuries, thoracic aortic dissection, cranial nerve VI palsy, and rib and skull fractures. Additionally, we found that most cases of traumatic RH occurred following a cervical vertebral fracture between C4 and C5. Especially in geriatric patients, falls constitute a significant contributor of morbidity and mortality, which is consistent with our findings (Table 1).
Tsao et al35 found that falling accidents are the leading cause of RH, with symptoms typically appearing within the first 24 hours of blunt trauma. It is therefore critical to monitor patients closely and inform them and their caregivers that symptoms may persist for up to 24 hours after a serious injury.
According to our review, the median age of all cases reported was 68 years, with males constituting the majority. Those receiving anticoagulants or those with coagulation disorders are at an increased risk of bleeding.88 An additional study carried out by Shiba et al88 indicated similar results with a median age of 69 and a male dominance distribution. It was also found in the same study by Shiba et al,88 that high bleeding was associated with international normalized ratio of 4.5 and above. Sagittal CT images demonstrated significantly wider hematomas in the intubated group. A significant number of large hematomas were observed even in patients who did not take antiplatelet or anticoagulant medications.
SymptomsDue to the close proximity to the upper airway, the most common RH symptoms were respiratory symptoms (Figure 2), which usually developed within the first 24 hours, indicating that close monitoring and immediate treatment should be sought during this period.
Radiological findingsAn imaging study of the neck (typically a CT scan or an MRI) is carried out by trauma surgeons and emergency physicians to evaluate whether RH is compromising the airway and the severity of the problem.
Most studies we included reported CT scan findings consistent with our findings, including: cases of RHs (n=26, 38%), prevertebral soft tissue swelling (n=10, 15%), prevertebral hematomas (n=10, 15%), cervical fractures (n=9, 13%), hypoattenuating retropharyngeal collection (n=1, 2%), occipital condylar fractures (n=2, 3%), retropharyngeal soft tissue swelling (n=4, 6%), pharyngeal mass (n=5, 7%), and cervical spondylosis (n=1, 0.2%, Table 2). Shiba et al88 reported a median width of 2.2 cm for the hematoma on sagittal CT images. The presence of a wider hematoma on sagittal CT images indicates that earlier intubation is necessary.88 According to other previous studies, the hematoma diameter in intubated patients ranged from 1.5-3.6 cm.11,32,73 This was similar to the median diameter of the hematoma in the intubated cases in Shiba study.88 These results confirm the predictive value of hematoma size in predicting the need for early intubation. Therefore, a large hematoma on sagittal CT images should be considered a red flag for early intubation.
An additional study carried out by Taso et al,35 found that roentgenography (77.9%) of the neck or cervical spine was the primary diagnostic tool, and only 1 out of 53 images failed to reveal the presence of an enlarged prevertebral space. Other diagnostic methods included CT of the neck (67.6%), a fiberscope (42.6%), angiograms (14.7%), MRI of the neck (13.2%), and autopsy (2.9%).35 Most studies, however, used CT scans as the first line of diagnostic testing.35
In a study by Anagnostara et al,52 MRI findings were similar, with prevertebral edema, and minimal residual hyperdense or hypodense retropharyngeal tissue on T2 and hypointense retropharyngeal collection on T1. In addition to the neurologic examination, an MRI was carried out in order to diagnose spinal cord injury. The clinical assessments were not standardized and were carried out based on the standard of care of each center.35
Treatment modalitiesAccording to several previous studies that have described the time course between trauma and intubation, respiratory collapse usually occurs between 2 and 17 hours after trauma.12,84,89 As soon as RH is diagnosed, intubation should be carried out to prevent sudden airway obstruction. The use of early intubation may be beneficial for patients who are older and have low hemoglobin levels and platelet counts.35,88 The timing of intubation is also determined by physical findings, such as stridor and swelling of the neck.35,88
In our study, the majority of cases were observed (n=44, 63.8%), followed by surgery (n=13, 18.8%), percutaneous aspiration (n=7, 10.1%), and transcutaneous arterial embolization (n=5, 7.2%). Among the 62 cases, only 16 (23%) were admitted to the ICU (Figure 3).
It was reported by Shiba et al88 that approximately half of the intubated patients required tracheotomies, with tracheotomies being carried out on the third day of illness on average. In previous studies, all patients evaluated underwent tracheotomies within 4 days of admission. Laryngoscopy or follow-up imaging was used in some studies to determine whether tracheotomies were necessary. In our current study, most patients underwent intubation (Figure 4).
A study by Karmacharyaya et al1 concluded that 48.65% of cases were managed conservatively, with the remaining requiring cricothyrotomy or intubation, with a resolution time of 7.69±5.44 days.
Over 40% of patients in the Shiba study88 required transfer to another hospital for rehabilitation. Patients discharged to home and those discharged to other hospitals were compared in terms of their baseline characteristics. Baseline characteristics, such as age, intubation, duration of ICU stay, and duration of mechanical ventilation, did not differ significantly between the 2 groups.
Among patients with traumatic RH, acute airway obstruction is one of the leading causes of death. Thus, maintaining airway patency is crucial for the initial care of patients with RH. Endotracheal intubation is the initial step in airway management and observation and conservative management are the most common treatment options for traumatic RH. Despite being a classic method of locating the source of bleeding, halting the bleeding, and removing hematomas, surgery can be complicated when dealing with patients who have sustained injuries to their head and neck. Due to improvements in imaging and endovascular techniques, transarterial embolization and percutaneous aspiration are now commonly used along with nonoperative treatment.
Study limitationsFirst, intubation was determined by each physician, and intubation protocols are not standardized. This has resulted in a lack of clarity regarding the exact indications for intubation. Some patients were also prophylactically intubated. Additionally, our study involved a relatively small number of patients. No data were obtained regarding hematoma expansion time course. Thus, the rate of hematoma expansion could not be predicted or pinpointed, nor could the appropriate time of intubation.
Accordingly, future studies should address and establish a protocol for when intubation should be used in such cases. A comprehensive understanding of the course of Traumatic RH should be achievable by using a larger sample size and more detailed presentation.
In conclusion, traumatic RH is a life-threatening event where a swelling hematoma may fully obstruct the airway. Retropharyngeal hematoma primarily occurs due to cervical trauma, with falling being the most prevalent cause. Most traumatic RHs arise after cervical vertebral fractures. The majority of the injuries (50.0%) were cervical spinal injuries. The majority of patients were older, with a median age of 68 years for all occurrences that were documented. Dyspnea was the most prevalent symptom (66.6%), and the majority of patients presented symptoms during the first 24 hours. Observation was the most prevalent treatment modality for 50% of the patients, and endotracheal intubation was the most common airway management method.
AcknowledgmentThe authors gratefully acknowledge Editage (www.editage.com) for thier English language editing.
FootnotesDisclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
Received July 31, 2023.Accepted November 6, 2023.Copyright: © Saudi Medical JournalThis is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
留言 (0)