
記住我










Objectives: To compare the complications associated with cannulated hip screws (CHS) and dynamic hip screws (DHS) techniques.
Methods: In this multicenter retrospective chart study, we reviewed the records and data of all patients operated upon by DHS or CHS for treatment of Garden type I and type II intracapsular non-displaced femoral neck fracture from January 2017 to December 2022. Patients with incomplete files or follow-ups of less than one year were excluded from the study.
Results: The study enrolled 85 patients, 35 males, and 50 females, with a mean age of 72±5.4 for males and 70.6±7.6 for females. A total of 44 patients were operated upon with DHS, and 41 patients with CHS. The mortality rate of DHS was 15.9% and was 17.1% in the CHS group (p>0.05). Non-union was recorded in 4.5% of the DHS group and 4.9% of CHS patients (p>0.05). Avascular necrosis (AVN) was significantly higher in DHS (9.1%) than in CHS (4.9%, p<0.05). A revision was required in 15.9% of DHS patients and 14.6% of CHS patients (p>0.05).
Conclusion: This study found that DHS was superior to CHS in AVN rate. However, there was no significant difference between both methods regarding mortality, revision, and non-union.
Keywords:According to the Garden classification, intracapsular femoral neck fractures may be incomplete valgus impacted non-displaced (type I), complete non-displaced (type II), or displaced (types III and IV).1 Dynamic hip screws (DHS) or cannulated hip screws (CHS) are considered by many authors to be the treatment of choice in patients with Garden type I and II intracapsular femoral neck fracture.2
Previous studies identified that CHS are superior to DHS in terms of rotation and stress stability, in addition to being less invasive.2-6 However, DHS is better regarding anatomical reduction, maintenance of neck-shaft angle, and reduced liability for implant loosening, especially in osteoporotic patients.3,5,6 Complications of cannulated screws (CS) and DHS include: non-union, avascular necrosis (AVN), and revision.7,8
The pathophysiology of these complications after fixations with no or minimal displacement are poorly explained. However, the initial elevation of intracapsular pressure and the disruption of terminal branches of the medial femoral circumflex arteries from torsion or ripping intracapsular will increase the risk of AVN.9 Hardware failure and revision could be due to the degree of nick angle tilting after the fracture, which may cause this complication.10 Non-union after fixation could be due to insufficient healing and poor fixation techniques.9,10
In this retrospective chart review, we compared the complications associated with CHS and DHS techniques.
MethodsIn this multicenter retrospective chart review, we reviewed the records and data of all patients who underwent DHS or CHS for the treatment of non-displaced intracapsular femoral neck fractures at King Abdulaziz Specialist Hospital in Taif, Al Noor Specialist Hospital, and King Faisal Hospital in Makkah, Saudi Arabia, between January 2017 and December 2022. All data were gathered retrospectively from the medical record database via a review of the outpatient digital records and postoperative notes. The inclusion criteria were as follows: I) Garden type I and II intracapsular femoral fractures; II) patients operated on with DHS or CHS with or without anti-rotational screws; III) follow-up time greater than one year, and IV) age of >50 years. The exclusion criteria were as follows: I) incomplete files; II) pathological fractures of the femoral neck other than osteoporosis; and III) previous femoral neck fractures (Figures 1 & 2).
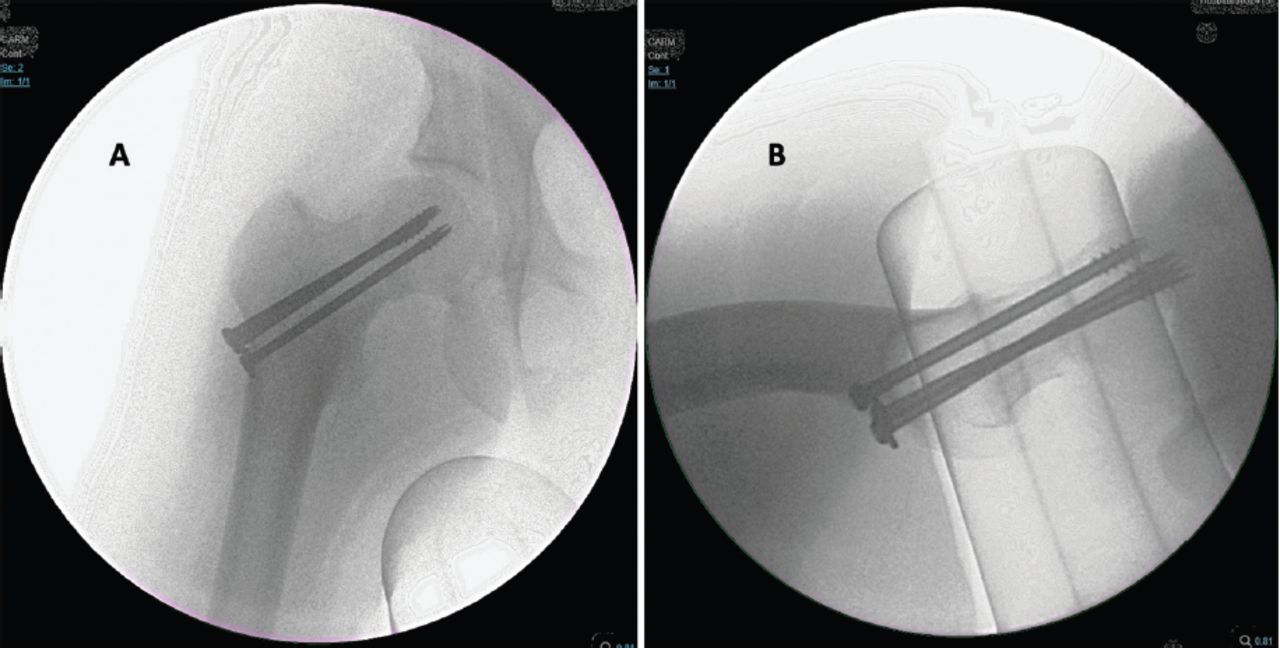 Figure 1
Figure 1 - Intraoperative images displaying right femoral neck fractures fixed by cannulated hip screws. A) Anteroposterior and B) lateral views.
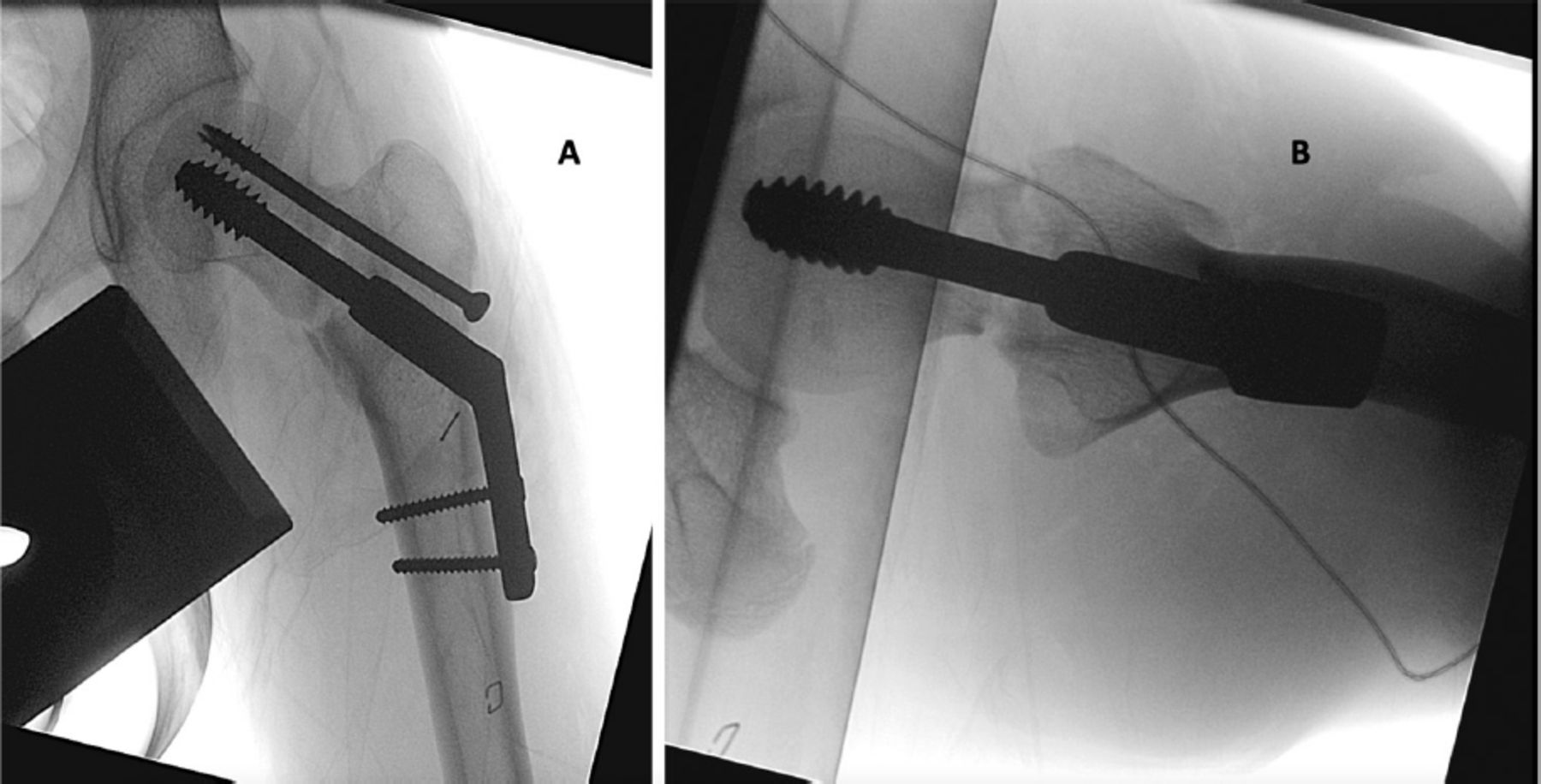 Figure 2
Figure 2 - Intraoperative images displaying left femoral neck fractures fixed by dynamic hip screws with anti-rotational screws. A) Anteroposterior and B) lateral views.
This study was approved by the institutional review board (no.: HAP-02-T-067) at Ministry of Health, Taif, Saudi Arabia. All patients provided informed consent. This retrospective study concerning human participants followed the institutional and national research committee’s ethical standards and the principles of the Helsinki Declaration and its comparable ethical standards.
All post-operative images were evaluated to assess the union and estimate any complications. Plain images of the hip were considered for signs of AVN. In contrast, magnetic resonance images and computed tomography were carried out to help in confirming the diagnosis for ambiguous cases (Figures 3 & 4).
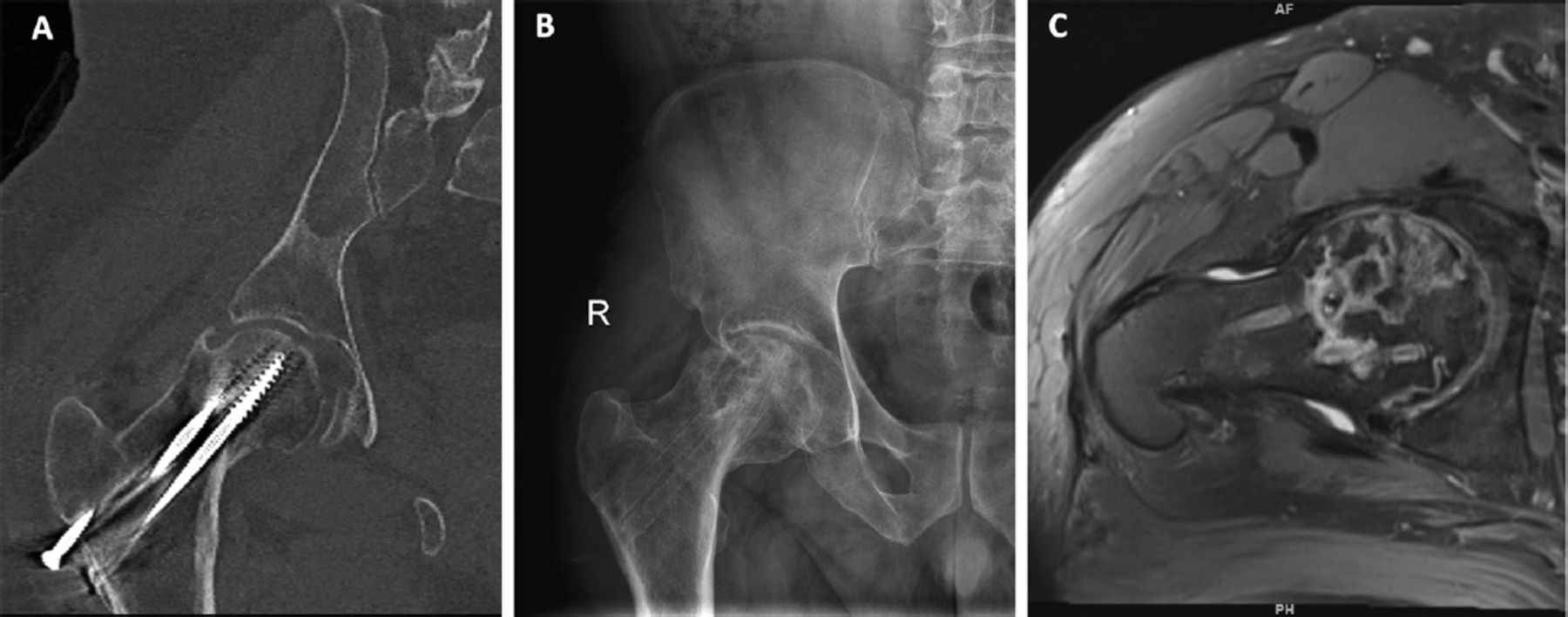 Figure 3
Figure 3 - Postoperative images display a fracture complicated by avascular necrosis of the right femur head. A) Coronal CT; B) an anteroposterior x-ray; and C) an axial MRI views of the right hip.
 Figure 4
Figure 4 - A fixed fractured neck of the femur is complicated by non-union and implant failure on an anteroposterior x-ray view.
The study was carried out after approval from the ethics committee, and written consent was obtained from the patients or the relatives of deceased patients to use data from their hospital records. Outcomes included mortality, AVN, and revision rates.
Statistical analysisResults are expressed as mean ± standard deviation (SD) using the Statistical Package for the Social Sciences, version 23.0 (IBM Corp., Armonk, NY, USA). Statistical significance was set at p-value of <0.05.
ResultsThe study enrolled 85 patients, 35 males, and 50 females; DHS patients were 41; CHS patients were 44; the mean age was 72±5.4 for DHS and 70.6±7.6 for CHS; and the mean follow-up period was 24±5.6 months (Table 1). The reduction quality was evaluated by intra- and postoperative plain radiographs.
Table 1- Patient’s characteristics.
A total of 55 (64.7%) patients underwent surgery on their right hip, while the remaining 30 patients underwent surgery on the left hip. The mean duration from the fracture to operation in both groups was 102.5 hours (range: 24-189 hours). A total of 37 patients had diabetes, while the remaining patients were not diagnosed with the disease. A total of 21 patients were smokers. The mean duration in DHS cases from fracture to operation time was 99.5 hours, while it was 105 hours in CHS (p=0.562). Moreover, the mean operation time was 75 minutes in DHS cases and 80 minutes in CHS (p=0.191, Table 2).
Table 2- Epidemiological data.
The mortality rate of DHS method was 7/44 (15.9%) and 7/41 (17.1%) in CHS method. Moreover, no significant difference between the 2 methods was observed (p>0.05). Non-union was 2/42 (4.5%) in DHS and 2/41 (4.9%) in CHS (no significant difference). The AVN recorded was 4/44 (9.1%) in DHS and 2/41 (4.9%) in CHS. These findings demonstrate that AVN was significantly higher in DHS than in CHS (p<0.05). The mean time for AVN complaints was 29 weeks (range: 20-38 weeks) postoperatively. A revision was required in 7/44 (15.9%) patients of the DHS group and 6/41 (14.6%) CHS patients with an insignificant difference (p>0.05, Table 3). In our present study, the success rate in patients who was treated by CHS was 65.9%, while the success rate in patients who was treated by DHS was 56%.
Table 3- Rate of complications.
DiscussionThe outcomes of CHS and DHS, the most commonly used surgical treatments for intracapsular non-displaced femoral neck fractures, are affected by the pattern of blood supply to the femoral neck.1-3 Defective blood supply increases the risk of complications such as non-union, AVN, implant loosening, and the need for revision.2-6 By the results of our study, Li et al7 concluded in their meta-analysis that DHS and CHS had similar complications; however, they identified that CHS had a significantly lower AVN rate than DHS. However, Lim et al8 discovered in their study that DHS is preferred for vertically oriented femoral fractures because of a lower rate of non-union compared to CHS. Li et al7 emphasized in their meta-analysis that previous studies reporting the advantages of DHS for the management of displaced femoral necks lacked detailed information to compare the difference between both techniques for displaced/non-displaced fractures; they also reported that the number of CS might have an unpredictable bias.
In the current study, the mortality rates were 15.9% for DHS and 17.1% for CHS, similar to the results of Li et al.7 In the studies of Sorensen et al11 and Gupta et al,12 which had different follow-up periods and unequal sample sizes, the range of mortality varied from 0-40%.
In our study, the non-union rate was 4.5% in the DHS group and 4.9% in the CS group, with no statistically significant differences. Li et al7 reported in their study a rate of non-union that was higher than our results; however, concomitant with our results, they identified that DHS and CHS have no significant difference in the non-union rate. Similar results have been reported by Gupta et al,12 Chen et al,13 and Jettoo et al.14 However, Lim et al8 reported in their study that non-union was significantly higher in the CHS than in the DHS for vertically oriented femoral fractures.
In the current study, the rate of AVN was significantly higher in the DHS group (9.1%) than in the CHS group (4.9%). The aforementioned results are similar to those reported by Li et al,7 Gupta et al,12 Nauth et al,15 and Widhalm et al.16 However, a much higher AVN rate for CHS compared to DHS was recorded in a study by Hoshino et al.17 Watson et al18 discovered that the rate of AVN with DHS and CHS was approximately 3%, with no significant difference between the 2 techniques. Li et al7 concluded that CHS involves less soft tissue stripping and is less invasive than DHS with a much lower blood supply insult. They also emphasized that age and fracture type could affect AVN mortality and development.
The rate of revision with internal fixation, hemiarthroplasty, or total hip replacement in our study was 15.9% in DHS and 14.6% in CHS, and this difference was statistically insignificant, which was per the results of previous studies.7,15,16 In the study by Gupta et al,12 the revision rate was much lower than that in our study, even though they discovered a non-significant difference between DHS and CHS. Shehata et al19 reported that the reoperation rates for DHS and CS were the same, whereas Zhang et al20 reported that the reoperation rate for CHS was higher than that for DHS. In conclusion, this study determined that DHS was superior to CS in terms of AVN rate. However, no significant differences were observed between the methods in terms of mortality, revision, or non-union.19,20 Also, the latest study by Bouaicha et al21 compared the 2 types of fixation in 72 patients. They reported significantly improved hip disability and osteoarthritis outcome scores (p=0.001) in CHS patients (n=33) compared to DHS patients (n=39). However, according to Garden classification, they compared all types of femur neck fractures.21
Study limitationsIts retrospective design and the lack of randomization in assigning the treatment option to the patient. Probably, we would have seen more powerful associations if we had included functional scores in our study.21 In addition, the management of CHS was inconsistent; some were 2, and others were 3 screws. Also, not all the DHS cases had anti-rotational screws. Further prospective randomized control trial studies are needed to evaluate the long-term clinical outcomes of both techniques.
In conclusion, this study found that both types of fixations for femur neck fracture (DHS and CHS) have similar complications, including mortality, revision rate, non-union, and AVN. However, DHS was superior to CHS on the AVN rate. No statistically significant association was found between both methods regarding mortality, revision, and non-union. However, further research is needed to evaluate the long-term clinical outcomes of both techniques.
AcknowledgmentThe authors gratefully acknowledge Taif University, Taif, Saudi Arabia, for supporting this study. The authors also would like to thank all participants for their valuable time in this study. Also, they would like to thank Editage (www.editage.com) for English language editing.
FootnotesDisclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
Received November 20, 2023.Accepted December 11, 2023.Copyright: © Saudi Medical JournalThis is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
留言 (0)