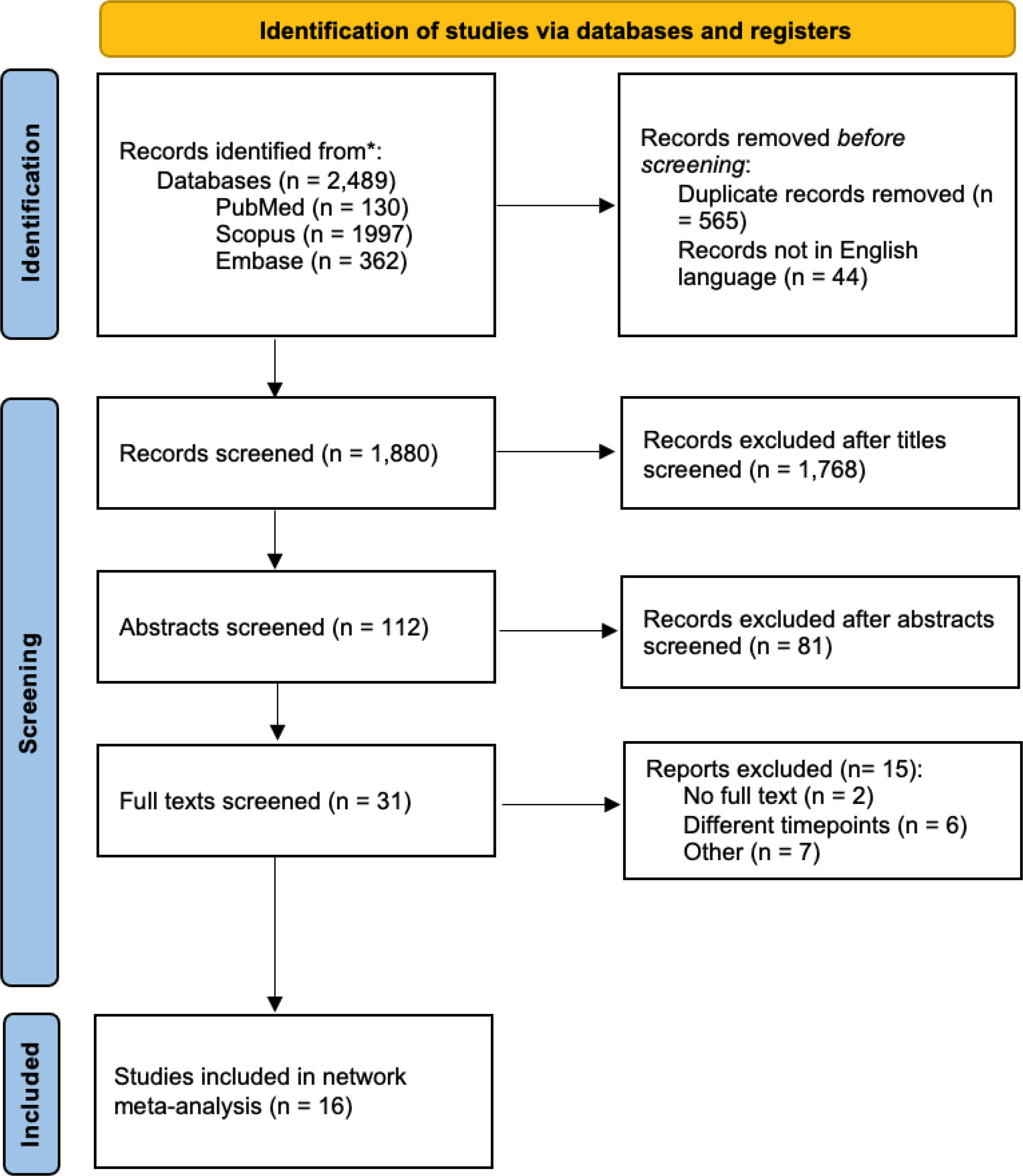
This study, including 3213 patients and 8 RCTs [2, 4, 14, 15, 17,18,19,20,21,22,23,24], is, to our knowledge, the largest meta-analysis of randomized controlled trials conducted thus far encompassing an adult population.
The results demonstrate that antibiotic therapy as a first-line treatment has a failure rate of 29.5% during the initial hospitalization, 35.4% at 1-year follow-up, a non-statistically significant difference in terms of length of stay (LOS), a comparable rate of complications and significantly lower costs compared to surgical treatment.
Several meta-analyses over the previous years have highlighted that surgical treatment is associated with an increased rate of complications, such as the study by Podda et al. [25], published in 2019. On the contrary, two recent studies [6, 26] did not observe a lower rate of complications in the conservatively treated group. Our study aligns with these latter findings. This is likely attributed to the higher number of laparoscopic appendectomies performed more recently. As compared to open technique, laparoscopic appendectomy has been shown to significantly reduce wound infection rates [27]. In our analysis the rate of laparoscopic appendectomies performed was 68.44%, as reported by 6 RCTs. Furthermore, recent trials included in our study predominantly analyzed laparoscopic appendectomies, with a percentage of 100% for a trial [14], 96% [21], and 90% [17], respectively. In contrast, previous studies, particularly the Antibiotic Therapy vs Appendectomy for Treatment of Uncomplicated Acute Appendicitis (APPAC) trial and the study conducted by Styrud et al., primarily consisted of open procedures.
Another important factor that could influence these results is the presence of appendicoliths. In the CODA trial, participants who were randomized to antibiotic medication and had an appendicolith experienced problems with a rate of 14% compared to 2% in those who did not [21]. This latter trial and the study by Vons et al. [22] included patients with appendicoliths diagnosed by CT scan. The other trials had a heterogeneous diagnostic protocol, so several patients with appendicoliths may have remained unrecognized.
In conclusion, we can affirm that NOM is safe, as it has a comparable rate of complications to laparoscopic appendectomy. However, there was heterogeneity in diagnostic assessment, antibiotic regimens and treatment duration among the various studies, which could impact the results.
The higher number of laparoscopic appendectomies may have also influenced the outcome regarding LOS. It is well-established in the literature that LOS is shorter when the procedure is performed laparoscopically, leading to an equivalence in LOS with conservative treatment [27]. It was not possible to perform a subgroup analysis due to lack of the necessary data. However, it would be important, in the future, to have RCTs that perform totally laparoscopic appendectomies, as Ceresoli et al. did, or that perform a subgroup analysis to explore the differences between laparoscopic and laparotomy appendectomies for this outcome.
However, this result is certainly influenced by significant heterogeneity in the implementation and management of conservative therapy. Indeed, there is inconsistency among the studies regarding the type of antibiotic used, the duration of intravenous administration, and subsequent oral administration. For example, in the CODA trial [21], an initial bolus, administered on the first day, was followed by oral therapy from the second to the tenth day. On the other hand, O’Leary et al. [17] continued that the antibiotic therapy until a clear clinical improvement of the patient was achieved.
Regarding the results concerning the complication-free treatment success during the initial hospitalization, they significantly favor surgical intervention. The conservative treatment has an efficacy rate of 71.84% in the index hospitalization.
Undoubtedly, a clear advantage of appendectomy is the ability to remove the pathogenic cause with a negligible risk of stump appendicitis [28]. Conversely, this is not possible with conservative treatment, which carries a significant risk of lifetime recurrence, estimated between 6.7% and 8.6% [29].
The treatment effectiveness assessed at one-year follow-up demonstrates a greater effectiveness of surgery compared to conservative treatment; this latter has an efficacy of 67.3% at one year compared to 97.4% for appendectomy.
It is important, therefore, to determine whether a conservative treatment with a lower efficacy measured at one-year follow-up and with comparable rates of complications, can be considered acceptable and feasible as a first-line treatment. It is true that approximately one-third of patients experience a recurrence within the first year. However, according to the 5-year follow-up results of the APPAC trial, patients can be successfully treated again with antibiotic therapy, and if surgery is required, it does not appear to be associated with increased complications or technical difficulty.
In fact, when Salminen et al. [30] published the 5-year follow-up findings of the APPAC randomized clinical trial in 2018, they addressed the issue of the paucity of research on the long-term clinical efficacy of antibiotics, which had previously been seen as one of the most significant barriers to the widespread adoption of NOM for uncomplicated appendicitis. Only 2.3% of patients undergoing surgery for recurrent appendicitis were found to have complicated forms of the disease and the overall complication rate was significantly lower in the antibiotic group than in the appendectomy group (6.5% vs. 24.4%, P = 0.001) among patients who were initially treated with antibiotics for uncomplicated appendicitis.
Recently, Pàtkovà et al. have published a cohort study regarding the long-term outcomes of NOM [31]. This study drew patients from two RCTs included in this meta-analysis: Eriksson et al.'s study [4] published in 1995 and Styrud et al.'s study [19] published in 2006. The article concludes that over the course of two decades, more than half of the patients treated through NOM did not experience recurrences, and there is no evidence of long-term risks associated with NOM, except for the recurrence itself. The long-term follow-up confirmed the feasibility of NOM as a surgical alternative. It would be very important to have new RCTs that analyze the results of the comparison between NOM and OM in the long term, in order to draw more robust conclusions on the topic.
Therefore, given these circumstances, an informed patient choice is crucial, in our opinion. In a study published by Hanson et al. [32] in 2018, 9.4% of the surveyed population responded that they would opt for nonoperative management (NOM) in the case of appendicitis. This number increased to 14.5% when asked about choosing for their children. The study focused on discussing the failure rates of NOM, and indeed, the authors themselves speculate that different numbers would have been obtained if the success rates were presented to patients. A more recent study, published in 2021 by Bom et al., presents very different results. Approximately half of the participants in the average population sample expressed a preference for antibiotics as a treatment for uncomplicated appendicitis, even if it entailed a higher risk of recurrence, in order to avoid surgery initially. Additional rigorous qualitative research will be necessary to investigate the factors behind the strikingly different outcomes observed in these two studies and to gain a deeper understanding of patient preferences in various situations.
We are faced with two therapies that are equivalent in terms of safety, with one being less expensive, less effective, and non-invasive, while the other is more expensive, more effective, and invasive. Beyond the decision of which therapy should be considered first-line, the outcome that could matter the most is the patient's quality of life.
Regarding this latter outcome, the diversity of presented results highlights the need for more literature. To establish more reliable analyses, it is crucial to use homogeneous scales across various trials. It is interesting to notice, despite the limitations outlined above, that in the three studies examined in one case, there is no difference in QoL between NOM and OM, and in the remaining two, the surgery appears to be associated with higher QoL.
Interpreting these results for clinical application requires consideration of several limitations. The significant heterogeneity limits confidence, variations in intervention expertise and the broad timespan of included RCTs may introduce confounding factors. Our study encompassed RCTs spanning a significant time frame from 1995 to 2022. Over this period, there were significant advancements in surgical techniques, diagnostic imaging, and antibiotic selection, resulting in noticeable variations in treatment protocols across the included studies. These variations were evident in the use of different antibiotics and the progression of surgical techniques from predominantly open appendectomies to primarily laparoscopic procedures throughout the chronology of the included RCTs. These variations have resulted in a high degree of heterogeneity among the studies, which constitutes a significant limitation, potentially biasing the analysis.





留言 (0)