
記住我
A 9-month-old girl presented to the UDN with features felt to be due to Jeune syndrome. She was conceived via in vitro fertilization (IVF) and was born at 31 weeks and 4 days gestation due to premature rupture of the membranes to a 31-year-old gravida 2, para 1 mother. The delivery was vaginal, vertex, and uncomplicated. Polyhydramnios occurred during pregnancy and a 20-week prenatal ultrasound showed fetal hepatosplenomegaly, ventriculomegaly, total body edema, thickened nuchal fold and echogenic kidneys. Amniocentesis was performed for microarray, karyotype, and fluorescence in situ hybridization (FISH) for trisomy 13, 18, and 21 which were all normal.
The Apgar scores were 6, 1, and 8 at 1, 5, and 10 minutes of life respectively. The infant required positive-pressure ventilation for cyanosis and apnea. She was noted to have extensive lymphedema, dysmorphic features, and hypotonia on initial exam. Chest X-rays showed a severe bell-shaped chest, handle-bar clavicles, thin ribs, and left lung atelectasis. Abdominal X-ray was notable for hepatomegaly, bilateral acetabular dysplasia, and flaring of iliac wings (Fig. 1). Initial cranial ultrasound was unremarkable except for extensive scalp edema and a spinal ultrasound was concerning for a tethered cord. Cardiac echocardiogram showed patent foramen ovale (PFO), patent ductus arteriosus (PDA), mild right atrial enlargement and a mildly dilated right ventricle with normal systolic wall motion. She passed her newborn hearing test at 3 months old.
Fig. 1: Clinical features of the patient.
A Shortly after birth, the “coat hanger” rib deformities are seen. B Supine view demonstrating the impact of her rib cage and scoliosis on her abdominal content. C A seated view of the impact of the rib cage and scoliosis on her abdominal contents. D The acetabular dysplasia is seen on this view and the progression of the scoliosis. E Toddler and F infant views of the child. Her full cheeks and small chin can be observed. The patient’s family consented to publication of these photographs.
She was admitted to the NICU for 3 months. On the 45th day of life she underwent surgery for placement of a tracheostomy for respiratory failure and gastrostomy tube for dysphagia. Her neonatal course was further complicated by non-ketotic hypoglycemia, hyperinsulinemia, nephrotic syndrome, and MRSA bacteremia and tracheitis. An immune evaluation was performed due to her infections and was normal. After discharge, she was ventilator-dependent for another 6 months. Her neonatal problems resolved, and she started receiving Early Intervention Services: physical therapy, speech therapy, occupational therapy and feeding therapy; with good progress.
Physical exam findings were significant for small chin, low set/posteriorly rotated ears, narrow and bell-shaped chest, rhizomelic appearing limbs, ulnar deviation at wrists, bent 3rd finger on left hand, hepatomegaly, contractures of extensor tendons on dorsum of feet, mild scaphocephaly, horizontal nystagmus, intermittent R > L esotropia, hypertelorism and shallow coccygeal dimple (Fig. 1). There was concern for increasing head circumference and a brain MRI showed ventriculomegaly involving lateral and third ventricles. She also was found to have collapsed long thoracolumbar scoliosis measuring over 50 degrees when she was sitting. Our patient had some features consistent with KOS1 (Supplemental Table) although her rib features were more severe than most published cases.
She is now 46 months old and was decannulated at 27 months of age. Her bell-shaped chest and respiratory status have improved. Her scoliosis continues to progress and is in the moderate range. She is developmentally delayed in gross and fine motor skills but has been walking independently since 20 months of age and said her first words at 12 months of age. Her receptive language is thought to be normal. She is making progress with oral feeds even though she is still dependent on G-tube feeds. After KOS was diagnosed, her medical regimen has been simplified. She recently had a normal abdominal ultrasound and serum α-fetoprotein level of 3 (<20 ng/mL) and will be regularly screened for hepatoblastoma, an unquantified risk in KOS.
Diagnostic evaluationsThe patient was seen in the UDN at 24 months of age. Previous post-natal genetic testing included a non-diagnostic skeletal dysplasia panel (Invitae Skeletal Dysplasia Panel) with multiple variants of uncertain significance in 5 different genes (none felt to be candidates), a negative trio WES (GeneDx XomeDxPlus), negative mitochondrial DNA analysis (GeneDx), and a negative deletion/duplication analysis of skeletal dysplasia genes (Custom testing at Division of Medical Genetics, UPMC Children’s Hospital of Pittsburgh). The reanalysis of WES data by the UDN team was non-diagnostic. Upon review by the UDN team, including an ad hoc member specializing in thoracic dystrophy, we concluded that thoracic dystrophy was unlikely, and we expanded our testing to WGS and DNA methylation. The WGS official report was negative but commercial testing of DNA methylation (Greenwood Genetic Center) was abnormal suggesting a methylation defect. Reanalysis of WGS on site revealed a 203 bp de novo deletion (hg38 chr14: 100825924-100826126/NC_000014.9:g.100825924_100826126del) overlapping the MEG3 transcript and the promoter region which was later confirmed by long-read sequencing (Figs. 2 and 3). MEG3 is a noncoding RNA and is typically not covered in WES. The small deletion was not reported on the WGS report as it was below the resolution of the reportable deletions (typically about 3 kb). The short-read sequencing could not establish the parent-of-origin of the 203 bp deletion, therefore long-read sequencing was performed. The MEG3 region was phased using informative heterozygous SNVs (read-based phasing using whatshap) and the parental origin of the two haplotypes were determined using the nearest paternally inherited SNV revealing the deletion on the maternal allele. Methylation profiling using long-read sequencing also revealed that the DNA methylation of the maternal allele was also aberrant. With this information, we established the diagnosis of KOS in this patient, determined that the deletion was apparently de novo, and based on the etiology were able to provide the family with important recurrence risk information.
Fig. 2: Long-read sequencing.
A A schematic diagram of the deletion revealed though long-read sequencing. The paternal variant is shown in the right-hand section which allowed phasing of the de novo deletion, which is shown in the left block of reads on the maternal allele. Long-reads were phased using heterozygous variants in the genome and the maternal/paternal haplotypes were differentiated using the previously existing parental WGS data. B The methylation profiles from Illumina Epic 850k array. The proband is the red tracing and six controls from a publicly available dataset (GSE153211) are shown in gray. C The phased methylation probabilities identified from PacBio data. The solid lines show the patient data while an internal control is shown as dashed lines. The patient data shows the hypermethylation of maternal allele confirming the diagnosis of Kagami–Ogata syndrome. D Visualization of methylation probabilities along the reads in the MEG3:TSS-DMR region. Each line represents a read and regions shaded in red are methylated while blue are unmethylated. Unshaded regions denote the lack of methylation data. CpG islands in the region are displayed as green horizontal bars.
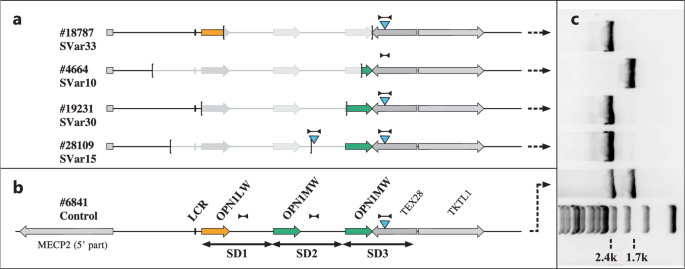
Fig. 3: Genomic locations and sizes of deletions causing Kagami–Ogata syndrome.
A comparison of the 203 bp de novo deletion in our patient is shown in red (hg38 chr14: 100825921-100826123/NC_000014.9:g.100825921_100826123del) and previously reported deletions causing Kagami–Ogata syndrome. Paternally expressed genes are labeled in blue. The length of each deletion is specified on the right.
留言 (0)