
記住我
Inborn errors of immunity (IEI) associated with atopy provide valuable insights into the pathophysiology of the immune system and pathways responsible for atopic disease. Atopy is a recognized component of a growing number of IEI as wider phenotypes are defined, and in some may be the predominant manifestation. Given atopy-related manifestations of these diseases may present to a range of clinical specialists across infancy to adulthood, we set out to summarise recent developments in this field. We highlight novel genetic conditions that may present at this interface, including gain of function mutations in the IKAROS transcription factor [1▪▪], and autosomal dominant gain of functions (GOF) in signal transducer and activator of transcription 6 (STAT6) [2▪▪,3]. Finally, we propose an updated mechanistic framework for the development of atopy at the interface of IEI whilst highlighting pitfalls for associated complications, and opportunities for precision therapy.
 Box 1:
Box 1: no caption available
MATERIALS AND METHODSWe conducted a rapid literature review using the search terms ‘Atopy AND primary immunodeficiency’ OR ‘atopy’ AND ‘inborn errors of immunity’ in PubMed, considering articles published between 1 January 2020 and 1 June 2023. Particular attention was given to monogenic disorders added to the International Union of Immunological Societies (IUIS) 2022 update of IEI [4▪]. We included disorders where case reports described clinically significant features of allergic rhinitis, asthma and atopic dermatitis (eczema), elevations in IgE or hypereosinophilia. Two independent reviewers classified each monogenic disorder within the predominant category of mechanism. Where disagreement arose regarding classification, a consensus was agreed with the wider team. We identified new genes with reported atopic presentations within the most recent 2022 IUIS IEI update combined with a rapid literature review. The dates these disorders were reported is shown in Fig. 1, and clinical phenotypes summarized in Table 1, adapted from Lyons et al. [5], and Nelson et al. [6▪]. Table 2 illustrates a comprehensive overview of all IEI associated with atopy, adapted from Lyons et al. [5], Nelson et al. [6▪] and IUIS update [4▪].
 FIGURE 1: Updated timeline of genes discovered responsible for inborn errors of immunity associated with atopy [1▪▪,2▪▪,4▪,17,19–27].
Table 1 -
Novel IEIs with atopic manifestations – diagnostic features, atopic prevalence and clinical pitfalls
References
Total cases described
Age of diagnosis (years)
Key features
Atopic features
Clinical pitfalls
STAT6 GOF
Sharma et al.[2▪▪]
16
3–60
Early-onset atopy within the first year of life
FIGURE 1: Updated timeline of genes discovered responsible for inborn errors of immunity associated with atopy [1▪▪,2▪▪,4▪,17,19–27].
Table 1 -
Novel IEIs with atopic manifestations – diagnostic features, atopic prevalence and clinical pitfalls
References
Total cases described
Age of diagnosis (years)
Key features
Atopic features
Clinical pitfalls
STAT6 GOF
Sharma et al.[2▪▪]
16
3–60
Early-onset atopy within the first year of lifeLyons et al.[5] proposed seven broad categories of inborn errors of immunity favouring development of atopy. Our adaptation has been modified to include the following eight categories, summarised in Fig. 2: impaired skin and mucosal barrier function; cytoskeletal abnormalities; aberrant TCR signalling; disrupted cytokine signalling; decreased T cell repertoire diversity and thymic development disorders; regulatory T cell (Treg) disorders; innate cell effector mechanisms; and metabolic disorders.
 FIGURE 2:
FIGURE 2: Categories of pathogenic mechanisms of atopy in inborn error of immunity.
We describe an expansion in both the number of IEI with associated atopic manifestations and in the mechanistic categories underpinning the pathogenesis. This highlights the importance of awareness and early recognition of atopy as a manifestation of a growing number of IEI.
Cytoskeletal abnormalitiesCytoskeletal disorders include Wiskott-Aldrich syndrome (WAS), Wiskott-Aldrich syndrome protein (WASP) WAP interacting protein (WIP), Dedicator of cytokinesis 8 (DOCK8) deficiency and Serine/threonine kinase 4 (STK4) deficiency. These cause a combined immunodeficiency with atopic features. WAS, DOCK8 and STK4 are also linked to a higher rate of autoimmunity and malignancy, illustrating the broad effects of immune dysregulation in IEI [4▪,5,6▪]. Deficiencies in the Nck-associated protein 1-like (NCKAP1L) gene, also known as hematopoietic protein 1 (HEM1), were first reported in humans by Castro et al.[17]. The gene encodes a haematopoietic lineage specific regulator of the actin cytoskeleton, vital for downstream signalling of activated Rac to stimulate F-actin polymerization in response to engagement of immune receptors [B cell receptor, TCR, Toll like receptor (TLR) and cytokine receptors] and is responsible for actin cytoskeleton reorganisation. Disruption to mechanistic Target of Rapamycin (mTOR) 2 and F-actin control results in immune dysregulation. Nine patients have been reported, for which a cohort of five patients from four unrelated families described by Cook et al.[16], had atopic and inflammatory diseases, chronic hepatosplenomegaly, lymphadenopathy with elevated IgE in 4 patients. Other features included recurrent bacterial and viral skin and respiratory infections and specific antibody deficiencies. Lymphoproliferation, cytokine overproduction, lymphadenopathy, hyperinflammation and autoimmune manifestations were also reported [17].
Variants in the MSN gene have recently been described as the cause of X-linked moesin-associated immunodeficiency (X-MAID). Sixteen cases have been reported worldwide. Patients with hemizygous mutations in the MSN gene present with lymphopenia, impaired T-cell proliferation, hypogammaglobulinemia, altered migration and adhesion capacities and susceptibility to bacterial and viral infections of the respiratory and gastrointestinal systems. Eight patients had skin manifestations mainly of eczema, molluscum contagiosum and atopic dermatitis [18,19]. MSN, ezrin and radixin are members of the ezrin-radixin-moesin (ERM) family which modulates the actin cytoskeleton and plasma membranes [42].
Aberrant TCR signallingDefective TCR signalling is evident in CARD11, BCL10, MALT1, CARML2, ZAP70, LAT and RLTPR deficiencies. Presentations consist of CID/severe combined immunodeficiency (SCID) with atopic features such as eosinophilia and high IgE. TCR signalling can either be absent or of reduced strength. Low strength signals between the TCR and major histocompatibility complex (MHC) complex have previously been demonstrated to skew naive T cell differentiation toward a T helper cell (Th) 2 response, promoting atopy [4▪,5,6▪]. Depending on the type of defect in CARD11, presentation can differ. Dominant negative mutations are associated with atopy, including moderate to severe dermatitis, high IgE and CID, like MALT1 deficiencies [5,6▪]. ZAP70 deficiency may manifest as atopic disease before the immunodeficiency becomes apparent [6▪].
RLTPR deficiency causes aberrant TCR signalling, by interfering with CD28 stimulation in T-cells [7]. Patients present with CID, recurrent bacterial, fungal and mycobacterial infections, and skin manifestations such as diffuse and recurrent warts. Atopic features include dermatitis, eosinophilic oesophagitis, asthma, food allergy, cold urticaria and high IgE [4▪,5,6▪].
Disruption of cytokine signallingGenetic defects causing ineffective cytokine signalling include IL6RA, IL6ST, STAT3 and ZNF341.
Patients with dominant negative loss of function mutations in STAT3, present with recurrent infections, atopic dermatitis, eosinophilia, food allergy and high IgE. ZNF341 is involved in STAT3 gene expression and presents in a similar fashion. This condition promotes atopy, as STAT3 phosphorylation leads to suppression of Th2 responses and favours Th17 responses, thereby reducing the propensity for atopy. Mutations in STAT3 diminish this effect, resulting in increasing Th2 responses [6▪].
Autosomal dominant STAT6 GOF variants associated with early-onset (<12 months) severe atopy have been reported by multiple groups [2▪▪,3,43–45]. Treatment-resistant atopic dermatitis and food allergies were most common, followed by asthma, eosinophilic gastrointestinal disease and anaphylaxis. Elevated IgE levels and eosinophilia were noted [2▪▪]. STAT6 is an intracellular transcription factor downstream of IL4 and IL4R/JAK-kinase signalling cascade and a central node of immune polarization and a key modulator for the risk of allergic disease in humans and mice [3,46]. Translocation of STAT6 to the nucleus, activates a pattern of gene expression mediating Th2 cell differentiation, M2 macrophage polarization, promotion of B cell survival and IgE class switching [47–50].
Seven kindreds were reported as sporadic, and three kindreds followed an autosomal dominant pattern of inheritance. Clinical features of wider immune dysregulation included recurrent nonfatal skin, respiratory, and viral infections identified in half of the cohort. Similar to characteristics of DN STAT3 LOF, short stature, pathologic fractures and generalised hypermobility were described. One patient died due to anaphylaxis at aged 20 and the other aged 35 secondary to a cerebral aneurysm, demonstrating the severity of the multisystem disease in this cohort [2▪▪]. It is notable that somatic activating mutations in STAT6 have been associated with B cell lymphoma [51–53]. The oldest patient in the cohort, experienced recurrent B cell lymphoma with follicular lymphoma aged 49 with subsequent relapse with a transformed follicular lymphoma (diffuse large B cell lymphoma) aged 60 [2▪▪].
Decreased T cell repertoire diversityThis mechanism manifests as Omenn syndrome, a type of leaky SCID, associated with multiple genetic defects including recombination activating gene (RAG)1, RAG2 and adenosine deaminase (ADA). Hypomorphic mutations in the responsible genes result in a limited number of T cells which undergo oligoclonal expansion. These T cells preferentially differentiate into the Th2 lineage, causing the classical presenting symptoms of hepatosplenomegaly, lymphadenopathy, erythroderma, eosinophilia and high IgE [4▪,5,6▪].
Two hypotheses exist to explain how a reduced diversity of T cells can result in atopy. The first suggests that reduced T cell diversity causes a lack of Tregs and loss of regulation of Th2 with subsequent atopy. The second hypothesis suggests low strength TCR signalling leading to skewing of Th2 differentiation. Due to reduced thymopoiesis, there is a lack of T cells with high affinity receptors which leads to a preferential expansion of T cells with low affinity receptors that differentiate into Th2 cells, thus promoting atopy [5].
Altered balance of conventional T cells and regulatory T cellsReduced numbers of Tregs leads to a failure of tolerance and presents as autoimmunity and features of immune dysregulation such as atopy [5,6▪].
FOXP3 is the master transcription factor for Tregs, and its deficiency is responsible for immunodysregulation polyendocrinopathy enteropathy X-linked (IPEX) syndrome. IPEX presents as autoimmunity with severe atopic dermatitis, food allergy, asthma, eosinophilia and high IgE [4▪,5,6▪].
IL2RA loss of function mutations lead to atopic features such as dermatitis, elevated IgE with autoimmunity and immunodeficiency. Tregs express the most IL2RA and fail to survive in its absence. IL-2 signalling through its receptor on Tregs promotes production of IL-10, promoting tolerance. Deficiencies in IL2RA result in loss of survival signals for Tregs and loss of suppressive function, favouring atopy [5,6▪].
IKAROS gain-of-function mutationsGermline heterozygous IKAROS GOF mutations presented with profound autoimmunity and immune dysregulation (75%, 6/8) with an age of onset of less than 1 to over 40 years. The regulation of IKZF1 is required for T helper cell, Treg and plasma cell differentiation [1▪▪].
Patients developed autoimmune diseases including type 1 diabetes mellitus, enteritis, autoimmune hepatitis, Hashimoto thyroiditis, leukocytoclastic vasculitis, vitiligo and alopecia with autoantibodies. GOF patients showed an absence of effector Treg and increased T follicular cell population, suggesting T-cell differentiation is compromised by abnormal IL-2 production. Autoimmune manifestations may be due to abnormal IL-2 production and effector Treg populations in these patients, as with other IEI patients with impaired Treg numbers and/or function IPEX syndrome and cytotoxic T-lymphocyte antigen 4 (CTLA-4) haploinsufficiency [54]. T cells expressing GOF mutations showed increased IL-4 (Th2) production, and decreased IL-2 and IFNγ production (Th1) [1▪▪,55].
Features also included atopy, lymphoproliferation and generally nonsevere bacterial infections. Whole-exome sequencing identified two patients with apparent autosomal dominant inheritance, as well as de novo occurrences. One patient harbouring a GOF mutation did not present with any clinical manifestations, demonstrating variable immunological penetrance.
Patients had mostly normal B-cell numbers, with normal to elevated immunoglobulin and IgE levels. Presentations of atopic disease included asthma, rhinitis, dermatitis, food allergy and eosinophilic oesophagitis. These are postulated to be due to increased Th2 differentiation with increased eosinophils, and production of IL-4 [56]. Increased IL-4 may result in Th2 and T follicular helper cell (TFH)2 skewing through negative regulation by IL-2 and/or hyper-IgE likely contributes to the development of allergic manifestations. Plasma cell hyper-proliferation was reported. Three patients had IgG4-related diseases demonstrated by an increased infiltration of the IgG4-positive plasma cells in the lymph nodes, intestine or bile duct [1▪▪].
Skin barrier defectsMultiple genes are associated with disrupted skin barrier function and infection, summarized in Table 2.
The ‘atopic march’ is characterized by early onset eczema predisposing to developing allergic rhinitis, then subsequently asthma and food allergies [6▪]. It is suggested that increased skin permeability from eczema, leads to cutaneous antigen-presenting cells (APCs) being exposed to increased amounts of usually innocuous environmental antigens. This leads to sensitisation, and production of Th2 associated pro-inflammatory cytokines, consequently initiating the allergic response [5,6▪]. Skin barrier disruption alongside downregulation of protective antimicrobial peptides, increases infection risk [6▪].
Pro-inflammatory type 2 cytokines also downregulate filaggrin, an important protein for skin barrier integrity [57], due to its role in producing natural moisturising factor, essential for hydration, during normal skin desquamation [58]. Therefore, disturbances in filaggrin production result in dry, flaky skin, increasing skin permeability, allowing increased exposure to antigens, and so the cycle continues [5]. This is observed in ichthyosis vulgaris, due to a homozygous LOF mutation in filaggrin, resulting in early onset (first months of life) severe atopy with elevated IgE [5,6▪].
Selective IgA deficiencySelective IgA deficiency (sIgAD) has similarly been postulated to result in impaired mucosal barrier function resulting in greater sensitisation and propagation of allergy. Up to 40% of sIgAD patients have allergy as a presenting or only symptom [37,38], with up to 84% of patients having some form of allergic manifestation, asthma being the commonest [35], others include allergic rhinitis, eczema and food allergy [35].
Ectodermal dysplasia and NF-κB essential modulatorAtopic features have been described in ectodermal dysplasia, including scalp dermatitis, atopic dermatitis and elevated IgE with positive skin prick tests [59].
Children with ectodermal dysplasia syndromes experience atopic symptoms more frequently compared to the general paediatric population, including asthma, food allergies, allergic rhinitis and eczema [40] due to skin barrier disruption [60] and hypohidrosis or anhidrosis, fuelling their atopic march [61].
NEMO deficiency is associated with eczema and erythroderma [62].
Thymic development disordersAtopy in chromosome 22q11.2 deletion syndrome (22q11.2del) is proposed to be related to T-cell lymphopenia and homeostatic pressure driving Th2 polarization [63]. Atopy has been associated with low T-cell receptor excision circles, with low T cells conferring nearly a three-fold increased risk of allergy [64,65], with patients presenting with asthma, rhinitis/conjunctivitis, food allergy and atopic dermatitis. Other IEI in this category are PAX1, EXTL3 and FOXN1.
Metabolic disordersMutations in MAN2B2 and PGM3 are congenital disorders of glycosylation (CDGs) [22,66].
Biallelic mutations in MAN2B2 have been shown to result in a CID, characterised by recurrent pneumonia, thrush, chronic diarrhoea and elevated IgE. Extra-immunological manifestations included small vessel vasculitis and thrombotic stroke [4▪,22].
PGM3 deficiency is regarded as a HIES [4▪]. Patients suffer from recurrent bacterial and viral infections, commonly affecting the skin and respiratory tract, low T cells and reduced memory B cells. Autoimmunity, along with severe atopy, including severe atopic dermatitis, food allergies and asthma have been reported, accompanied by marked eosinophilia and high IgE. Extra-immunological manifestations include neurological impairment, such as sensorineural hearing loss, low IQ, developmental delay and facial dysmorphism [4▪,66].
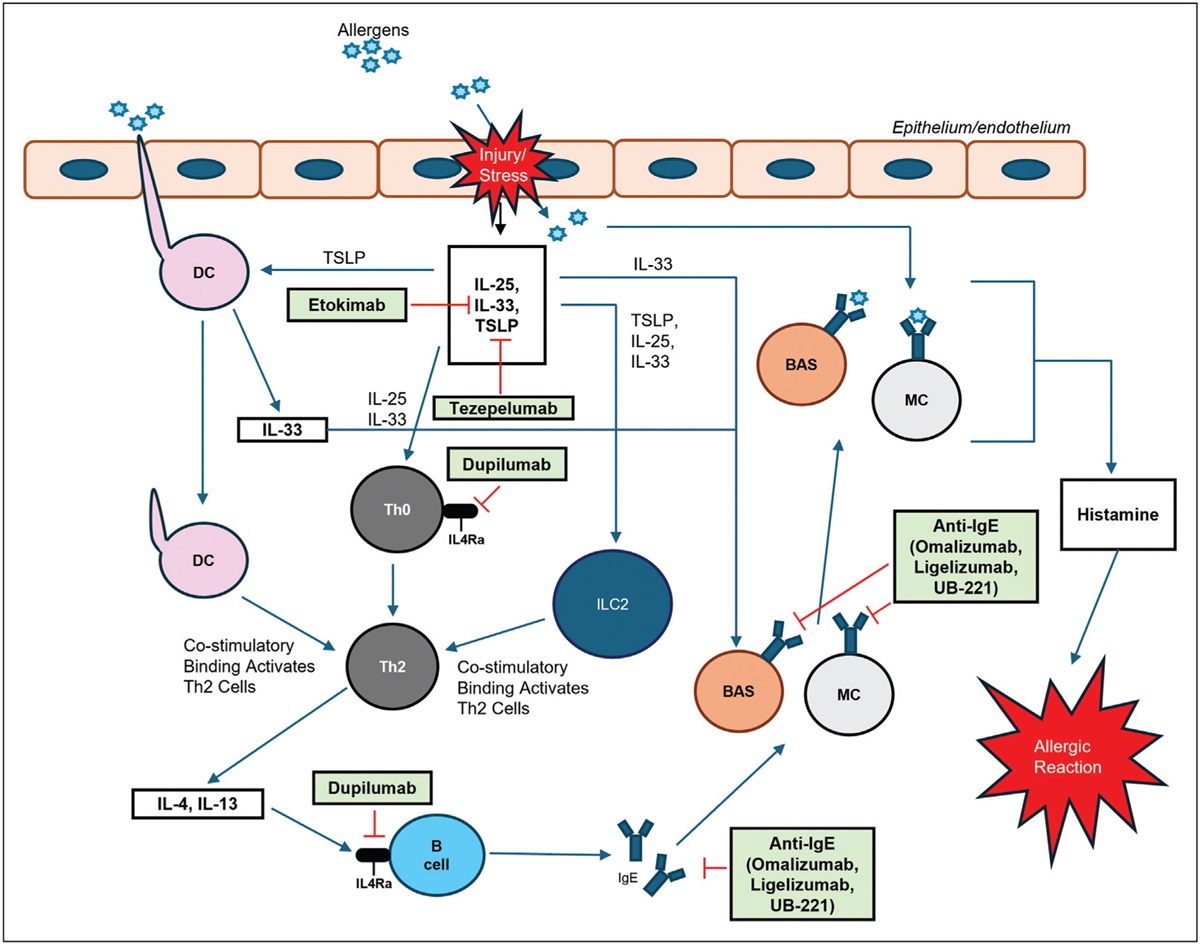
TREATMENT UPDATES – FOCUS ON PRECISION THERAPIESImprovements in genetic analysis have facilitated early diagnosis and options for precision therapy to modulate these defects. An expanding range of biologics and small molecule drug inhibitors are available for asthma or eczema, such as Mepolizumab (anti-IL5), Dupilumab (anti-IL4Rα) and Tezepelumab (antithymic stromal lymphopoietin) with potential for translational repurposing to rare diseases.
Dupilumab has been shown to be well tolerated and effective in a number of atopic diseases, especially refractory eczema. The IL-4α receptor antagonist inhibits the IL-13/ IL-4/ STAT 6 axis, disrupting IL-4 signalling and the allergic type 2 cytokine signature [67].
Dupilumab was highly effective in the three patients with STAT6 GOF variants, demonstrating clinical and immunological biomarker and cutaneous improvement with increased growth velocity and weaning or discontinued oral corticosteroids. Preclinical data have suggested that Janus kinase (JAK) inhibitors such as Tofacitinib and Ruxolitinib may be beneficial [2▪▪]. Phase II studies are ongoing with Bruton's tyrosine kinase inhibitors (BTKi) in atopic dermatitis [68].
Dupilumab used in autosomal dominant AD
留言 (0)