
記住我
Although the prevailing opinion is that food allergies have continued to increase worldwide in the 21st century [1,2], recent studies have challenged this notion. Spolidoro et al.[3▪]conducted a systematic review and meta-analysis of studies on the prevalence of eight major food allergies (cow's milk, hen's egg, wheat, soybean, peanut, tree nuts, fish, and shellfish) in Europe, and found that there were generally no significant changes in their prevalence between 2000–2012 and 2012–2021.
Over the past 20 years, food allergy prevention strategies in various countries have changed from ‘delayed introduction’ to ‘nondelayed introduction’ of allergenic foods, followed by a more recent paradigm shift toward ‘early introduction’ based on the findings of several randomized controlled trials (RCTs) [4–6] and research syntheses [7–12]. These changes may impact the prevalence and distribution of food allergies.
This review provides an outline of important studies published in 2022–2023 that addressed strategies to prevent childhood food allergies.
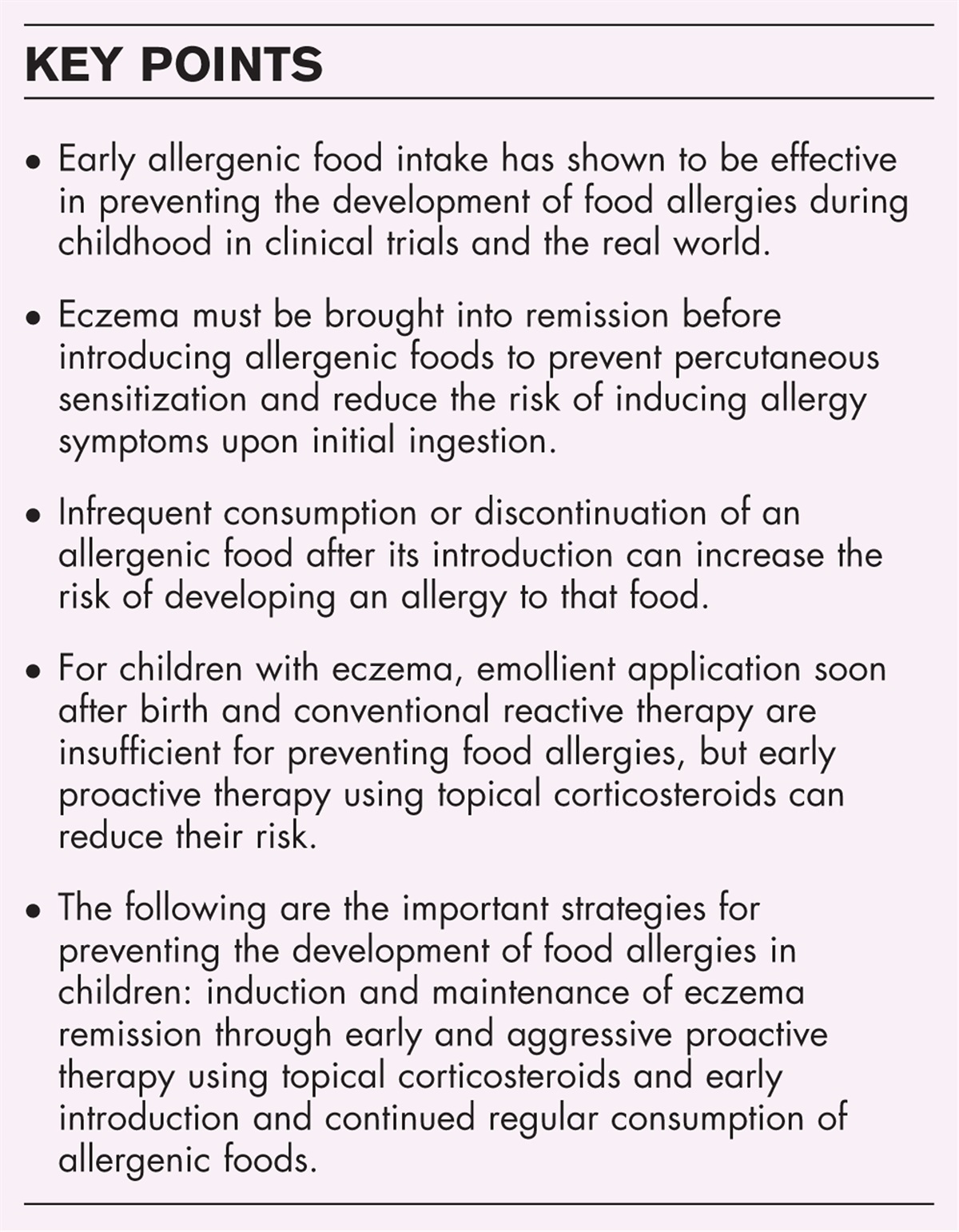
 Box 1:
Box 1: no caption available
EARLY INTRODUCTION OF ALLERGENIC FOODS: MULTIPLE FOODS, PEANUT, AND HEN'S EGGNumerous studies have examined the preventive effects of introducing multiple foods, peanut, and egg to infants at an early stage. Skjerven et al. conducted a large-scale RCT (Preventing Atopic Dermatitis and ALLergies, or PreventADALL study) involving a skin intervention (emollients) from 2 weeks of age and a food intervention (early introduction of multiple foods such as egg, cow's milk, wheat, and peanut) from 3 months of age in 2397 newborns from the general population in Norway and Sweden [13▪▪]. The food intervention [odds ratio: 0.4, 95% confidence interval (CI) 0.2–0.8] but not the skin intervention (odds ratio: 1.3, 95% CI 0.7–2.3), was significantly associated with a lower prevalence of food allergy at 3 years of age.
In an RCT conducted at multiple pediatric practices in Japan, Nishimura et al.[14▪▪] randomly assigned 163 participants aged 3–4 months with atopic dermatitis to a mixed food powder group (who ingested a mixed powder containing egg, cow's milk, wheat, soybean, peanut, and buckwheat) or placebo group (who ingested a placebo powder). The powders were ingested until 6–7 months of age, and the incidence of food allergy episodes by 18 months of age was 8.4% in the mixed food powder group and 23.8% in the placebo group (risk ratio: 0.30, 95% CI 0.12–0.78, P = 0.007). This suggests that even short-term, low-dose ingestion of multiple food antigens can prevent allergies, which deviates from the findings of the Enquiring about Tolerance (EAT) study [5].
Scarpone et al.[15] conducted a systematic review and meta-analysis on studies (including the aforementioned RCTs) that examined the timing of allergenic food introduction and allergies. They found that earlier introduction (2–12 months after birth) of multiple allergenic foods was more effective in preventing food allergy than later introduction (risk ratio: 0.49, 95% CI 0.33–0.74). In addition, early exposure to peanut (3–10 months after birth; risk ratio: 0.31, 95% CI 0.19–0.51) and egg (3–6 months after birth; risk ratio: 0.60, 95% CI 0.46–0.77) was associated with a lower risk of allergies to these foods.
Studies have also examined the real-world effectiveness of early food introduction. Hurley et al. compared the incidences of peanut and egg allergy between two cohorts of infants in Ireland: the Babies After Scope: Evaluating the Longitudinal Impact Using Neurological and Nutritional Endpoints (BASELINE) cohort (born in 2008–2011) and the Impact of Coronavirus Pandemic on Allergic and Autoimmune Dysregulation in Infants Born During Lockdown (CORAL) cohort (born in 2020) [16▪]. When compared with the older BASELINE cohort, the newer CORAL cohort had a higher prevalence of atopic dermatitis, but lower prevalences of peanut and egg allergy. The authors suggest that the lower food allergy prevalences in the CORAL cohort was influenced by the early introduction and continued ingestion of these foods as recommended by revised guidelines.
In Australia, revisions to infant feeding guidelines in 2016 included recommendations for the early introduction of peanut not only for high-risk infants, but for all infants [17]. According to the EarlyNuts study, the proportion of children who consumed peanut before 12 months of age increased from 28.4% in 2007–2011 to 88.6% in 2016–2018 [18]. In a study of children aged 11–15 months, Soriano et al.[19▪▪] investigated changes in peanut allergy before and after the 2016 guideline revision. The prevalence of peanut allergy decreased from 3.1% of 5276 infants in 2007–2011 (prerevision) to 2.6% of 1933 infants in 2018–2019 (postrevision), but this difference was not statistically significant (P = 0.26). However, their study noted that the proportion of children with East Asian ancestry, who are at higher risk for allergies, significantly increased from 10.5 to 16.5% over that time period. It is possible that the early introduction strategy suppressed the development of peanut allergy, but the effect was offset by the increasing proportion of East Asian children.
The early introduction of allergenic foods is not without risks. Mullins et al.[20▪] compared the food-induced anaphylaxis admission rates in Australian children among three periods: 1998–1999 to 2006–2007 (when guidelines recommended delayed allergenic food introduction), 2007–2008 to 2014–2015 (when guidelines stopped recommending delayed introduction), and 2015–2016 to 2018–2019 (when guidelines recommended early introduction). Annual food-induced anaphylaxis admission rates increased nine-fold between 1998–1999 and 2018–2019, with the rate of increase declining in children aged 1–14 years but accelerating in infants aged less than 1 year since 2016. The revised recommendations for early food introduction may have contributed to this increase in infant anaphylaxis.
To examine the impact of Australia's 2016 guideline revision, Chow et al.[21] compared the prevalence of food allergy symptoms and anaphylaxis between 2015 and 2018 among infants aged 4–12 months who visited the emergency department of a single institution. Despite a significant increase in the proportion of emergency visits for food allergy symptoms, the number of anaphylaxis presentations did not increase. The authors suggest that early food introduction to potentially sensitized infants may have caused the development of food allergy to surface earlier.
EARLY INTRODUCTION OF ALLERGENIC FOODS: COW'S MILKCow's milk allergy remains one of the most common food allergies, and as such is the focus of numerous studies. The systematic review and meta-analysis by Scarpone et al.[15] found that ‘early introduction’ of cow's milk, defined as exposure between 1 day and 4 months after birth, did not demonstrate any significant preventive effects (risk ratio: 0.84, 95% CI 0.38–1.87). However, the authors noted that the quality of existing evidence was generally low because of the inconsistent intervention methods employed by the RCTs. In particular, it is difficult to universally define what constitutes ‘early introduction’, as infant formula can be ingested from the first day of life.
The Strategy for Prevention of Milk Allergy by Daily Ingestion of Infant Formula in Early Infancy (SPADE) study was a Japanese RCT that examined the effectiveness of initiating infant formula at 1 month of age to prevent cow's milk allergy [22]. The incidence of cow's milk allergy at 6 months of age was 6.8% in infants who avoided ingesting infant formula, which was higher than expected. A SPADE study subgroup analysis evaluated the risk of cow's milk allergy associated with infant formula discontinuation after early introduction [23]. The results indicated that infants who discontinued ingestion before 6 months of age were significantly more likely to develop cow's milk allergy than those who continued daily or intermittent ingestion (risk ratio: 24.2, 95% CI 5.7–103.1; P < 0.001), and that the risk of developing cow's milk allergy was particularly high in infants who discontinued ingestion during the neonatal period (risk ratio: 65.7, 95% CI 14.7–292.5; P < 0.001). Therefore, the continued ingestion of cow's milk formula, even in low doses, appears to reduce the risk of cow's milk allergy.
This concept is supported by an intervention study from Israel [24▪▪]. In the Cow's Milk Early Exposure Trial (COMEET) study, Lachover-Roth et al. investigated the development of cow's milk allergy during the first year of life by assigning 1992 newborns from the general population to either continued cow's milk formula feeding for the first 2 months of life or exclusive breastfeeding, depending on the mothers’ wishes. The prevalence of cow's milk allergy was 0% in the group that continued formula feeding and 1.6% in the exclusive breastfeeding group (risk ratio: 29.98, P < 0.001). Furthermore, 0% of exclusively breastfed infants who started regularly ingesting formula developed cow's milk allergy, compared with 3.3% of infants who were exposed to small quantities of formula during the first 2 months of life.
REGULAR CONSUMPTION FOLLOWING EARLY INTRODUCTION OF ALLERGENIC FOODSBoth the SPADE study subgroup analysis and COMEET study found that despite early exposure to cow's milk protein, irregular consumption and discontinuation increases the risk of cow's milk allergy [23,24▪▪].
In the EarlyNuts study, the proportion of children who consumed peanut during infancy rose to almost 90% following the revision of Australian infant feeding guidelines in 2016 [18]. However, approximately 50% of infants consumed peanut at least once a week (less than 30% consumed peanut at least twice a week) until 12 months of age, whereas the remaining infants consumed peanut only a few times [18]. This lack of regular consumption may be a reason why subsequent surveys did not find a significant decrease in peanut allergy [19▪▪,25].
In a follow-up of the HealthNuts study cohort (an Australian single-center, population-based longitudinal study on various allergies), Leong et al.[26] identified children who had a negative oral challenge test for peanut at 1 year of age, and retrospectively investigated their peanut intake after the initial challenge test and subsequent development of peanut allergy. Approximately one-third of the children ingested peanut fewer than three times during age 1–4 years, and these children were more likely to eventually develop peanut allergy. However, the intake frequency cut-off in that study appeared to be arbitrary, and future studies are needed to determine the optimal intake frequency and quantity for preventing peanut allergy.
ANTI-INFLAMMATORY TOPICAL TREATMENT FOR ECZEMARecent studies have shown that protecting the skin surface with emollients alone is insufficient to prevent the development of food allergies [27,28], and that anti-inflammatory topical treatments for eczema (including nonlesional skin) are also necessary [29,30].
In the Prevention of Allergy via Cutaneous Intervention (PACI) study, Yamamoto-Hanada et al.[31▪▪] conducted an RCT on 640 infants aged 7–13 weeks with atopic dermatitis. Participants were randomly assigned to an early enhanced proactive treatment group or conventional reactive treatment group. In the former, participants used topical corticosteroids on the entire body (both eczematous and noneczematous areas) twice daily, and continued their use twice weekly after remission. In the latter, participants used topical corticosteroids only for eczematous skin. The incidence of egg allergy at 28 weeks of age was 31.4% in the proactive treatment group and 41.9% in the conventional treatment group, indicating that early and aggressive anti-inflammatory treatment for eczema can help to prevent the development of egg allergy. However, the height and weight of the proactive treatment group may have been partially suppressed, suggesting that anti-inflammatory topical therapy should be set according to each patient's eczema severity, rather than using the same protocol across the board.
The suppression of percutaneous sensitization through early and aggressive eczema treatment could help to reduce symptoms induced by allergen ingestion, which in turn may contribute to the well tolerated prevention of food allergies.
SCREENING FOR SENSITIZATION TO FOOD ANTIGENSPreemptive screening for food sensitization is generally not recommended due to the following disadvantages [25]:
(1) The time it takes to undergo screening and receive the results directly delays the start of food introduction. (2) If a screening result is positive, the caregiver may become anxious and inclined to delay food introduction despite the possibility of a false positive. (3) Screening does not appear to be cost effective.Accordingly, screening should be limited to cases where eczema cannot be brought into remission early or where parents are too anxious to introduce a food at home. In addition, a system is needed to provide prompt access to oral food challenges to obtain a definitive diagnosis for cases where screening results are positive for sensitization [32].
WHO ARE THE PREFERENTIAL TARGETS FOR INTERVENTION?Using data obtained from 1796 participants of the Learning Early About Peanut Allergy (LEAP) study [4] and the EAT study [5], Logan et al.[33▪] examined whether there were differences in the effectiveness of early peanut introduction on preventing peanut allergy according to eczema status and peanut sensitization. They found that early peanut introduction was effective in preventing allergy in children with eczema (regardless of eczema severity), but not in children without eczema. In contrast, the effectiveness of this intervention was not affected by peanut sensitization.
Roberts et al.[34] developed an intervention model for early peanut introduction in a general population based on data from 2137 children who participated in the LEAP screening study and the EAT study, and applied this model to compare the preventive effects of early peanut introduction in various risk groups and at different ages to the whole population. The results showed that it was more effective for this intervention to target the whole population (including lower risk children) than to target only the highest risk children with severe eczema. Furthermore, the preventive benefits of peanut introduction were found to diminish with every month of delay from 4 months of age. The authors recommend that peanut products should be introduced to infants at 4–6 months of age in countries where peanut allergies are common.
Kojima et al.[35▪] investigated the relationship between peanut ingestion during infancy and peanut allergy using data from 74 240 mother–infant pairs who participated in the Japan Environment and Children's Study (JECS), and found that 0.2% of children were allergic to peanut at 4 years of age. Although children who consumed peanut as infants had a lower incidence of peanut allergy than those who did not, this difference was not statistically significant (adjusted odds ratio: 0.53. 95% CI 0.17–1.68). The authors propose that early peanut introduction may not have preventive effects in regions with a low peanut allergy prevalence, such as Japan.
The above studies suggest that the preventive effects of early food introduction are influenced by the prevalence of the corresponding food allergy within a region. For highly prevalent food allergies, it may be more beneficial to introduce whole-population interventions in all children (regardless of eczema status or severity) rather than focusing on high-risk groups.
CONCLUSIONRecent evidence indicates that the following are integral to preventing food allergies in childhood: eczema should be treated promptly and aggressively with anti-inflammatory therapy to achieve remission; screening for food sensitization should be decided with consideration to its disadvantages; foods associated with high allergy prevalence in a region should be introduced to all infants at an early stage; and once an allergenic food is introduced, children should continue its regular consumption. Future research is needed to develop well tolerated, effective, and practical strategies to prevent food allergies.
AcknowledgementsNone.
Financial support and sponsorshipNone.
Conflicts of interestThere are no conflicts of interest.
REFERENCES AND RECOMMENDED READINGPapers of particular interest, published within the annual period of review, have been highlighted as:
▪ of special interest
▪▪ of outstanding interest
REFERENCES 1. Sampath V, Abrams EM, Adlou B, et al. Food allergy across the globe. J Allergy Clin Immunol 2021; 148:1347–1364. 2. Peters RL, Krawiec M, Koplin JJ, Santos AF. Update on food allergy. Pediatr Allergy Immunol 2021; 32:647–657. 3▪. Spolidoro GCI, Ali MM, Amera YT, et al. Prevalence estimates of eight big food allergies in Europe: updated systematic review and meta-analysis. Allergy 2023; 78:2361–2417. 4. Du Toit G, Roberts G, Sayre PH, et al. LEAP Study Team. Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med 2015; 372:803–813. 5. Perkin MR, Logan K, Tseng A, et al. EAT Study Team. Randomized trial of introduction of allergenic foods in breast-fed infants. N Engl J Med 2016; 374:1733–1743. 6. Natsume O, Kabashima S, Nakazato J, et al. PETIT Study Team. Two-step egg introduction for prevention of egg allergy in high-risk infants with eczema (PETIT): a randomised, double-blind, placebo-controlled trial. Lancet 2017; 389:276–286. 7. Ierodiakonou D, Garcia-Larsen V, Logan A, et al. Timing of allergenic food introduction to the infant diet and risk of allergic or autoimmune disease a systematic review and meta-analysis. JAMA 2016; 316:1181–1192. 8. Larson K, McLaughlin J, Stonehouse M, et al. Introducing allergenic food into infants’ diets: systematic review. MCN Am J Matern Child Nurs 2017; 42:72–80. 9. Natsume O, Ohya Y. Recent advancement to prevent the development of allergy and allergic diseases and therapeutic strategy in the perspective of barrier dysfunction. Allergol Int 2018; 67:24–31. 10. Al-Saud B, Sigurdardóttir ST. Early introduction of egg and the development of egg allergy in children: a systematic review and meta-analysis. Int Arch Allergy Immunol 2018; 177:350–359. 11. Burgess JA, Dharmage SC, Allen K, et al. Age at introduction to complementary solid food and food allergy and sensitization: a systematic review and meta-analysis. Clin Exp Allergy 2019; 49:754–769. 12. de Silva D, Halken S, Chris Singh C, et al. European Academy of Allergy, Clinical Immunology Food Allergy, Anaphylaxis Guidelines Group. Preventing food allergy in infancy and childhood: systematic review of randomised controlled trials. Pediatr Allergy Immunol 2020; 31:813–826. 13▪▪. Skjerven HO, Lie A, Vettukattil R, et al. Early food intervention and skin emollients to prevent food allergy in young children (PreventADALL): a factorial, multicentre, cluster-randomised trial. Lancet 2022; 399:2398–2411. 14▪▪. Nishimura T, Fukazawa M, Fukuoka K, et al. Early introduction of very small amounts of multiple foods to infants: a randomized trial. Allergol Int 2022; 71:345–353. 15. Scarpone R, Kimkool P, Ierodiakonou D, et al. Timing of allergenic food introduction and risk of immunoglobulin E-mediated food allergy: a systematic review and meta-analysis. JAMA Pediatr 2023; 177:489–497. 16▪. Hurley S, Franklin R, Murray D, et al. Changes in food sensitization with changing allergy practice in Ireland. Clin Exp Allergy 2023; 53:372–375. 17. Netting MJ, Campbell DE, Koplin JJ, et al. Centre for Food and Allergy Research, the Australasian Society of Clinical Immunology and Allergy, the National Allergy Strategy, and the Australian Infant Feeding Summit Consensus Group. An Australian Consensus on Infant Feeding Guidelines to Prevent Food Allergy: outcomes from the Australian Infant Feeding Summit. J Allergy Clin Immunol Pract 2017; 5:1617–1624. 18. Soriano VX, Peters RL, Ponsonby AL, et al. Earlier ingestion of peanut after changes to infant feeding guidelines: the EarlyNuts study. J Allergy Clin Immunol 2019; 144:1327–1335. e5. 19▪▪. Soriano VX, Peters RL, Moreno-Betancur M, et al. Association between earlier introduction of peanut and prevalence of peanut allergy in infants in Australia. JAMA 2022; 328:48–56. 20▪. Mullins RJ, Dear KBG, Tang MLK. Changes in Australian food anaphylaxis admission rates following introduction of updated allergy prevention guidelines. J Allergy Clin Immunol 2022; 150:140.e1–145.e1. 21. Chow SJ, McWilliam V, Koplin JJ, Perrett KP. Australian Infant Food Allergy Emergency Presentations following updated early food introduction guidelines. J Allergy Clin Immunol Pract 2023; 11:3473–3477. 22. Sakihara T, Otsuji K, Arakaki Y, et al. Randomized trial of early infant formula introduction to prevent cow's milk allergy. J Allergy Clin Immunol 2021; 147:224.e8–232.e8. 23. Sakihara T, Otsuji K, Arakaki Y, et al. Early discontinuation of cow's milk protein ingestion is associated with the development of cow's milk allergy. J Allergy Clin Immunol Pract 2022; 10:172–179. 24▪▪. Lachover-Roth I, Cohen-Engler A, Furman Y, et al. Early, continuing exposure to cow's milk formula and cow's milk allergy: the COMEET study, a single center, prospective interventional study. Ann Allergy Asthma Immunol 2023; 130:233.e4–239.e4. 25. Abrams EM, Shaker M, Stukus D, et al. Updates in food allergy prevention in children. Pediatrics 2023; 152:e2023062836. 26. Leong OWY, Perrett KP, Loke P, et al. Reintroduction of peanut into the infant diet following negative peanut oral food challenges. J Allergy Clin Immunol Pract 2023; 12:779.e1–782.e1. 27. Kelleher MM, Phillips R, Brown SJ, et al. Skin care interventions in infants for preventing eczema and food allergy. Cochrane Database Syst Rev 2022; 11:CD013534. 28. Zhong Y, Samuel M, van Bever H, Tham EH. Emollients in infancy to prevent atopic dermatitis: a systematic review and meta-analysis. Allergy 2022; 77:1685–1699. 29. Pavel AB, Renert-Yuval Y, Wu J, et al. Tape strips from early-onset pediatric atopic dermatitis highlight disease abnormalities in nonlesional skin. Allergy 2021; 76:314–325. 30. He H, Bissonnette R, Wu J, et al. Tape strips detect distinct immune and barrier profiles in atopic dermatitis and psoriasis. J Allergy Clin Immunol 2021; 147:199–212. 31▪▪. Yamamoto-Hanada K, Kobayashi T, Mikami M, et al. PACI Study Collaborators. Enhanced early skin treatment for atopic dermatitis in infants reduces food allergy. J Allergy Clin Immunol 2023; 152:126–135. 32. Koplin JJ, McWilliam V, Soriano VX, Peters RL. Early peanut introduction: to test or not to test? Ann Allergy Asthma Immunol 2023; 130:565–570. 33▪. Logan K, Bahnson HT, Ylescupidez A, et al. Early introduction of peanut reduces peanut allergy across risk groups in pooled and causal inference analyses. Allergy 2023; 78:1307–1318. 34. Roberts G, Bahnson HT, Du Toit G, et al. Defining the window of opportunity and target populations to prevent peanut allergy. J Allergy Clin Immunol 2023; 151:1329–1336. 35▪. Kojima R, Shinohara R, Kushima M, et al. Japan Environment and Children's Study Group. Infantile peanut introduction and peanut allergy in regions with a low prevalence of peanut allergy: the Japan Environment and Children's Study (JECS). J Epidemiol 2023; doi: 10.2188/jea.JE20230210. [Online ahead of print].
留言 (0)