
記住我








The University of Southern California Institutional Review Board approved all study procedures. Participants were recruited from general and veteran-targeted social media websites (Facebook, Instagram, RallyPoint, We Are The Mighty) in February 2020 for a larger study on veteran behavioral health; for details, see Pedersen et al.22 Social media was the primary recruitment method to target veterans recruited outside of additional VA settings. US veterans from the Navy, Air Force, Marine Corps, and Army between the ages of 18 and 40 were eligible. Veterans could also not be currently affiliated with the military via active duty service or in the reserve or guard units. Veterans did not need to have any behavioral health disorders or treatment experience at the VA or outside the VA to participate. A total of 1855 veteran participants were initially enrolled. Efforts to minimize fraudulent participation by computer bots or non-veteran individuals attempting to complete the survey were implemented, including removing participants that failed internal validation checks. The final sample size was N = 1230. To examine veterans’ behavioral health during COVID-19, follow-up surveys were sent at 6 months (August 2020; n = 1025; 83.3% retention), 9 months (November 2020; n = 1006; 81.8% retention), 12 months (February 2021; n = 1005; 81.7% retention), and 18 months (August 2021; n = 967; 78.6% retention) post-baseline. Participants received a $20 gift card for completing each of the baseline and 18-month follow-up surveys. The analytic sample for the current study includes demographic data from the baseline survey and the 18-month follow-up survey. As very few participants reported a gender identity that differed from their sex at birth (n = 2), this study only includes cisgender women (n = 83) and men (n = 882) in the final analytic sample for statistical power and generalizability purposes (n = 965).
After the first follow-up survey in August 2020, a subset of participants completed a 60-min qualitative interview via Zoom to discuss how veterans were coping with COVID-19. Twenty-three participants completed initial interviews. Detailed methods and findings from initial interviews are detailed in other published work.30 Women from the initial interviews were invited for a follow-up interview after completion of the 18-month survey in Fall 2021. Five of the seven women participants who completed the first interview agreed to an additional interview. Seeking to learn more about women veterans’ unique experiences related to behavioral health care, especially due to limited women-focused veteran behavioral health research amid COVID-19, the authors recruited and enrolled an additional 13 women veteran participants by emailing an additional subset of women from the larger study to inquire about interest in completing an additional paid interview with the study team. Thus, 18 women veterans total (22% of the study sample) completed the qualitative interview for the current study, which is generally a sufficient number of participants to reach thematic saturation.31 Participants were compensated with a $50 gift card for completing each interview and a $30 gift card for each follow-up survey. See Table 1 for demographics of the 18 interview participants, and men (n = 882) and women (n = 83) participants who completed the 18-month follow-up survey. This study reports methods and findings from questions unique to the 18-month follow-up interview.
Table 1 Analytic sample (men/women) and interviewee (women only) demographicsSurvey measuresDemographics were assessed at baseline, and measures of behavioral health, behavioral healthcare usage and satisfaction, and barriers and facilitators of treatment were assessed at the 18-month follow-up survey.
DemographicsParticipants reported on age, race and ethnicity, branch of service, and years served in the military.
Behavioral health screening measures DepressionDepression was measured with the 8-item Patient Health Questionnaire,32 which assessed specific depression symptoms (e.g., feeling down, depressed, and hopeless) over the past 2 weeks. Participants rated each item from “not at all” (0) to “nearly every day” (4). A summed score of 10 or more was used as the cutoff for a positive depression screen.32
PTSDPTSD symptom severity was assessed using the 20-item Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5).33, 34 Participants indicated how often they were bothered by 20 symptoms of PTSD in the past month (e.g., hyperarousal, unwanted memories of a traumatic event) from “not at all” (0) to “extremely” (4). A summed score of 33 or more indicated a positive PTSD screen.33
AnxietyAnxiety was assessed using the Generalized Anxiety Disorder 7-item questionnaire (GAD-7). Items assessed how often participants were bothered by anxiety symptoms (e.g., feeling nervous, anxious, on edge; excessive worrying) in the past 2 weeks. Participants rated each item from 0 = not at all to 3 = nearly every day, with a cutoff sum score of 10 indicating probable anxiety disorder.35
Alcohol use disorderParticipants completed the 10-item Alcohol Use Disorder Identification Test (AUDIT).36 The AUDIT assesses the frequency of symptoms of alcohol use disorder in the past year (e.g., failing to do what was normally expected due to drinking, not able to stop drinking once started). A cutoff score of 8 indicated a positive screen for “hazardous drinking,” while a score of 16 indicated a positive screen for alcohol use disorder.37
Behavioral healthcare usage and satisfactionParticipants reported past-6-month behavioral healthcare treatment utilization (defined as appointments for concerns relating to mental health or substance use, including outpatient psychotherapy, inpatient care, medication, and peer support groups). Participants indicated whether or not they received care through (a) VA and/or non-VA services, or via (b) in-person and/or telehealth in the past 6 months at the time of the survey (February 2021–August 2021). If participants endorsed receiving any modality of care, a series of follow-up questions asked about treatment frequency (days in past 6 months), separately for each provider and modality combination (e.g., “How many days in the past 6 months have you attended appointments [IN PERSON/ONLINE] at [the VA/a non-VA provider] to help you with a mental health or substance use concern?”) for all treatments endorsed. Those who received telehealth care were also asked to compare perceived quality of care for in-person vs. telehealth services (i.e., in-person better, telehealth better, both the same, or did not know/could not compare [due to never receiving in-person care]), separately for VA and non-VA services.
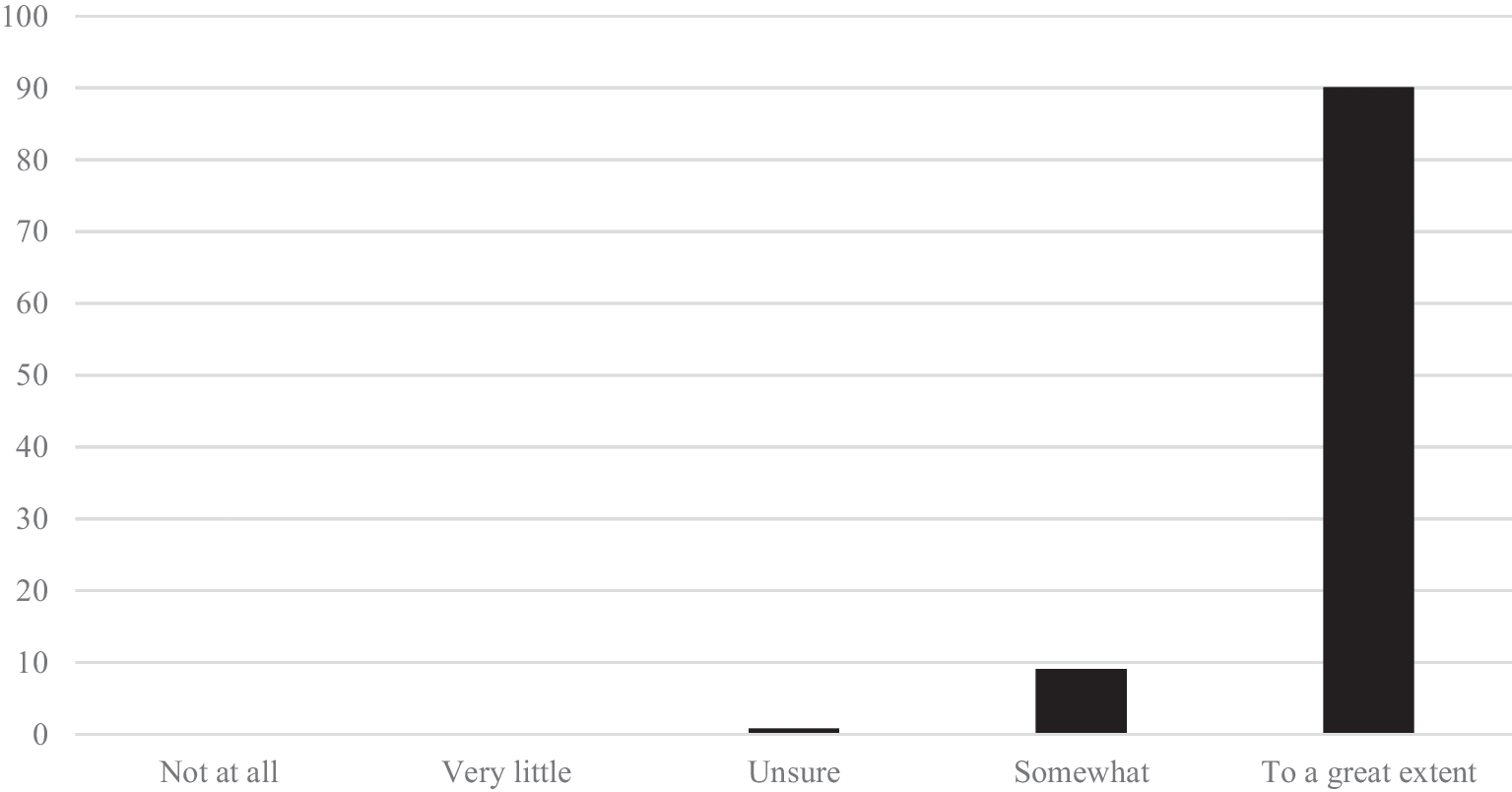
Perceived barriers and facilitators to treatmentBarriers to receiving behavioral health treatment were assessed with the Perceived Stigma and Barriers to Care for Psychological Problems scale, which was developed for use with young adult service members and veterans.38, 39 Items generally assessed perceived stigma from others and asked how each of the six items might affect one’s decision to seek treatment for a psychological problem from a mental health professional (e.g., a psychologist or counselor). Items were rated from “strongly disagree” (1) to “strongly agree” (4). For facilitators of care, participants completed the 6-item RAND Facilitators of Mental Health Care questionnaire,40 which assessed facilitators of receiving care from a behavioral health provider. Items were rated from “not at all” (1) to “very much” (5). Means for both 6-item scales were computed as overall scores for barriers (higher mean is higher agreement with barriers) and facilitators (higher mean is greater endorsement of facilitators). Individual items for the barriers and facilitators scales are listed in Figs. 1 and 2.
Fig. 1
Percent endorsement of barriers to behavioral health care questionnaire. Note. Strongly agree/agree and strongly disagree/disagree responses were combined for the barriers to aid interpretation
Fig. 2
Percent endorsement of facilitators to behavioral health care questionnaire. Note. Response options of very much/quite a bit and somewhat/a little bit are presented together in the figure to aid interpretation of results
Qualitative interview protocolSemi-structured interviews were initially designed to serve either (1) as a follow-up from a round of interviews conducted in 2020 or (2) as an initial interview, which both assessed the same past-year timeframe.30 The purposes of these interviews were to further inform and contextualize quantitative findings from the larger study. Interviews followed a standardized guide and included retrospective questions on behavioral health changes during the COVID-19 pandemic among veterans. Interviews did not specifically probe about behavioral health diagnoses, but rather centered on health, well-being, and access to treatment during COVID-19. In addition, interviewers asked questions regarding women’s perspectives on behavioral healthcare access for women veterans broadly (i.e., both during and prior to the pandemic). Interviews further probed about specific positive and negative experiences with VA care and asked if participants had any further thoughts about how women veterans could be better served.
Analysis plan Survey dataDescriptive statistics on sample demographics, behavioral health screening, treatment utilization, and perceived barriers/facilitators to behavioral healthcare among men and women in the sample are reported. To assess differences in treatment utilization, this study conducted Z-tests to compare the proportion of men and women in the sample who endorsed VA or non-VA treatment in the past 6 months at the time of the 18-month survey. Due to sample size, this study lacked the statistical power to test for differences between smaller treatment subgroups (in-person vs. online within the VA and non-VA). Furthermore, t-tests assessed for mean differences on reported barriers and facilitators of care between men and women.
Interview dataInterviews were recorded following participants’ consent, transcribed, and uploaded into Dedoose.41 The research team created a codebook based on the interview protocol and key research questions. The coding team, which consisted of three graduate-level research assistants supervised by a doctoral level anthropologist, first co-coded two interviews and then refined the codebook and application of codes. The coding team met regularly to discuss any responses that were unclear. After 20% of the interviews were coded, interrater reliability was calculated with a pooled Cohen Kappa coefficient and Cohen Kappa for each of the codes.42 Coding procedures were refined until the pooled Cohen Kappa coefficient and Cohen Kappa for each code was > 0.80, which demonstrates a high level of agreement and consistency across the qualitative analytic team42 and is accepted as a strong level of agreement among coders. Coding was followed by thematic analysis.43, 44 The authors followed standard approaches to identify key themes, or the range of responses under each code, by noting specific words, phrases, and ideas.43 The study team identified additional themes through repetition, metaphors used, and existing literature of sources of veterans’ healthcare-related perceptions.44
留言 (0)