
記住我


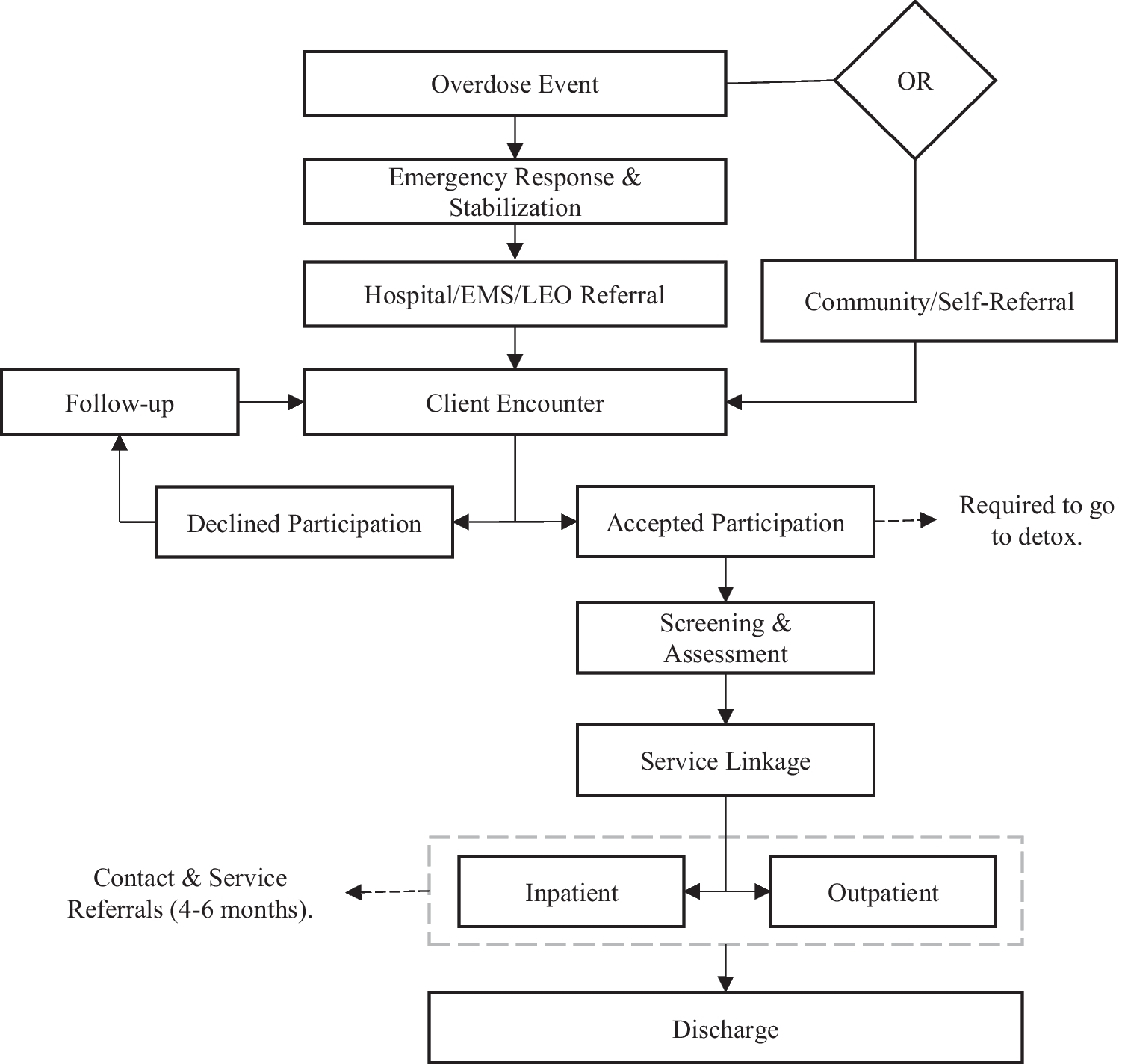
Four major themes and 15 subthemes were identified related to the implementation and potential for scale up of EASE in this setting. They are illustrated in Fig. 1 and outlined below, with illustrative quotes.
Figure 1.
Tree of the four main themes and the 15 subthemes from the qualitative analysis
Theme 1: Perceived Outcomes of the Program for Adolescents and CaregiversMost respondents expressed their positive experiences of participating in EASE, either as intervention participants, providers, or trainers/supervisors. They appreciated the opportunity to attend an activity outside the home, and to share feelings and thoughts with others. One trainer described how “they were happy to have a space where they can go out and talk”. The majority of EASE participants, providers, and trainers/supervisors also reported significant benefits obtained for adolescents, caregivers, and relationships inside and outside the family.
Perceived Outcomes for AdolescentsMost adolescents, caregivers, and providers highlighted positive impacts on adolescents at different levels. At the individual level, adolescents’ behavior improved, particularly regulating their reactions when feeling angry. For example, one adolescent noted that the strategy of slow breathing helped him to remain calm and manage strong emotions.
The slow breathing helped us so much, many times, when I’m angry or upset from someone, I do it and it makes me very relaxed, I do it, if I’m angry I do it, if I’m nervous or scared I do it (adolescent, male).
One female caregiver noted improvements in her adolescent boy:
I felt that he started to play- he even started to go outside the house and come back, he didn’t use to go out- he used to stay inside the house for a month or 20 days… and before I told you that he always I mean cries and do.. no, now he is better, thank god
Some respondents also noted improvement in adolescent’s ability to express themselves; how they can talk about their feelings, their personal strengths, their problems and how to deal with them, their daily life, and their relationships with their communities. One adolescent girl noted:
“before EASE we didn’t know much about solving our problems on our own, and now we know how to solve them”. One provider noted: “There were two girls, they didn’t talk at all, not any word, no reaction, no eye expression, and after the third session, they talked and expressed considerably." (provider, female). At the family level, some caregivers noted improved caregiver-child relationships. These respondents noted that this extended to improvements in relationships with others in the community, including interacting with other children, and reduced bullying or aggression with peers.
Perceived Outcomes for CaregiversMost providers noted positive outcomes regarding parenting behaviors. Several caregivers and providers noted that physical punishment remains an ingrained disciplinary technique. However, EASE taught alternative strategies which many caregivers considered helpful. Additionally, the majority of caregivers noted that they learned the rationale for giving praise and how to effectively deliver it. This was considered helpful, despite not being a well-known concept previously. One caregiver noted: “I stopped the violence, I approached them with nice words, with coping words” (caregiver, female).
Many providers and caregivers also described a positive effect on caregivers’ own wellbeing and behavior. For example, some caregivers used EASE strategies to improve their relationships and communication with their partners. They also applied the strategies of self-care to improve their overall well-being, for example: “They knew that they should have space (take a break) during the day to entertain a little about myself [have some time for themselves], maybe drink a coffee with a neighbor, walk a little…” (provider, female).
Theme 2: Barriers for Engagement, Attendance, and Impact Basic Needs are a Priority for FamiliesOutreach workers, stakeholders, providers, and participants stated the predominant barrier for engagement of adolescents and caregivers with EASE was the predominance of unmet financial and basic needs such as food and housing, where efforts to achieve these needs have made participants “exhausted, not only tired”. With the deterioration of the economic situation in Lebanon, families prioritized direct income generating activities rather than MHPSS interventions (i.e. EASE) that do not provide financial support. Competing scheduling priorities were a major issue for attendance, including families moving for work opportunities, adolescents attending school or work, adolescents or caregivers needing to care for younger children or other family members, or UN agency appointments including for financial support. Since EASE is group-based, scheduling around individual participants’ competing priorities was particularly difficult. “It’s the biggest difficulty we face, that the child doesn’t come when it’s agriculture season…when it’s potato season then no children come” (provider, female). One male caregiver whose adolescent did not complete the program expressed that: “If someone found work, it would be more important than the programme”. In focus group discussions, both outreach workers and providers stressed that recruitment of new participants became even more challenging with wide-scale protests commencing October 2019 causing closures (e.g. of schools, offices) and roads blocks, and subsequent further deterioration of the economic situation. In both male and female adolescent focus groups, participants cited the “roadblocks” as a major barrier causing adolescents to be “afraid” and they “maybe don’t want to go out of house”, or “the place he lives in”. Other barriers by adolescents included medical concerns, work, and other competing priorities (“they might be going to somewhere more important than this”), or lack of need “they might not be in need for it”. Unfortunately, several interviewees noted that the most vulnerable adolescents were even less likely to access the intervention, for example: “…Tripoli and Akkar, where EASE was implemented, have the highest rate of children involved in the worst forms of child labor, long hours in agriculture or on the streets, with those long working hours, they will not have time to attend EASE sessions.” (MHPSS stakeholder).
Importance of Caregiver EngagementDespite the program being offered to adolescents, the consent of both caregivers was considered by respondents as essential for ensuring child attendance. Some caregivers prevented attendance for different reasons including lack of financial support, needing their child to work inside or outside the home, or not wishing their daughter to attend a center at the same time as males. Some outreach workers noted that some Lebanese caregivers refused participation due to feeling that the intervention was for Syrian adolescents. Again, financial considerations played a large role in caregivers preventing their children from taking part, for example, one provider described: “The biggest difficulty is that there’s no financial allowance, the most difficult thing is that the parent tells the child go to work instead of going to play and have fun” (provider, female).
Stigma and Misunderstandings About Mental Health InterventionsMost MHPSS stakeholders stressed the fact that the stigma around accessing mental health interventions is prevalent in the community, and that it affects engagement with interventions like EASE. Different respondents mentioned that it would be very important to have a combination of outreach strategies to present the project in a way that it is not perceived as a “clinical” mental health intervention. This highlights the importance of carefully framing EASE in the wider context of healthcare or other community-based interventions and ensuring it is embedded in routine service provision to make it less stigmatizing.
Stigma is an issue nationally, it’s an issue for all interventions related to mental health and psychosocial support. But I think when we don’t say mental health it’s even easier, for when we say psychosocial support, and when we frame it in the sense that the intervention is not in mental health. (MHPSS stakeholder).
Additionally, challenges of uptake of an intervention known to be for those with heightened distress is “…linked to the stigma of like other people in the community knowing that their children are taking part in such an intervention.” (MHPSS stakeholder).
On the other hand, at times, there were misunderstandings about the nature of the EASE intervention, with some providers, trainers/supervisors, and outreach workers noting that some adolescents believed they were coming to “play,” similar to other psychosocial activities they had attended. Along with MHPSS stakeholders, they emphasized the importance of explaining the intervention clearly during outreach.
Intervention AccessFinding suitable locations for intervention delivery that were close to family homes for easy access was challenging. Families in this study lived in underserved agricultural areas, resulting in long commutes to intervention venues. Buses were provided for transport; however, all adolescents attending one group were picked up at various locations which led to lengthy trips for some adolescents. Some adolescents did not mind the long drives; however, providers noted that it could impact the sessions starting on time and the performance of participants. Additionally, outreach workers and caregivers observed that it required adolescents and caregivers to be out of the home for considerable periods of time.
I received multiple complaints, from the people participating with us, that the distance is too far away for them, also the roads of [agriculture area] are hard, especially in winter, and the bus needs a lot of time to make their way there (outreach worker, male).
Furthermore, finding suitable and comfortable venues with sufficient space for intervention delivery was difficult, and at times, not all activities could be implemented as planned.
It’s a school style, floors, classes, and seats, you enter and you don’t feel that the child is comfortable to enter such a place (provider, female)
Intervention ContentAlthough overall the feedback on the content and structure of the intervention was positive, some aspects were noted to make it challenging for some adolescents and caregivers. Some interviewees felt that the illustrations and story book used in EASE were more suited to younger adolescents than older adolescents. Additionally, one illustration of a character perceived to be male sweeping the floor was perceived to be unrealistic of the setting. Providers and trainers/supervisors stressed that some components of the intervention were complicated for adolescents to grasp, such as explaining the “vicious cycle of unhelpful behaviors and emotions” and the “changing my actions” strategy for changing behaviors in a stepped approach. It was felt that more sessions and more trainings for providers would be needed to cover these strategies adequately with adolescents. Providers additionally reported that the caregiver sessions were very dense with information, which was challenging to deliver and at times caused boredom in caregivers.
Theme 3: Working with Non-Specialist Providers Positive Experience of Providers Delivering EASEThe majority of stakeholders stressed that non-specialist providers are well placed to deliver EASE, and caregivers and children described their experience in working with the providers as “good” and “respectful”. Trainers/supervisors reported that providers were delivering the intervention with high fidelity and competency. This indicates feasibility of using non-specialist providers, if there is a clear package of competency building, with strong supervision and follow-up. Some stakeholders reported that a major benefit for non-specialist providers is that they are “less costly” compared to specialists which may increase the scalability of the intervention to reach more people. In the focus group with providers, they reported positive experiences delivering EASE, with personal benefits including applying some of the strategies in daily lives like “slow breathing”. Moreover, added professional benefits included improving knowledge, enhancing skills, and contributing to career development.
In EASE, it’s the first time I work in such a program. Like detailed to this extent and very specific, then this is for sure, this is so [..] positive for my professional experience (provider, female).
Challenges for ProvidersSeveral role-related challenges were highlighted. Some providers felt that at times, they were unable to meet the needs and expectations of some participants, as they understood providers as trained mental health professionals. Additionally, due to the delivery model, providers were employed on a casual contract basis. Therefore, working hours depended on the schedule of intervention groups, which could be inconsistent and difficult to plan for, leading to frustrations amongst providers. Providers expressed the need for stability in employment and progression in careers, with other stakeholders also stressing that non-financial incentives such arenon-specialist providers. Stakeholders also reported the possibility for providers to be “burned out” (MHPSS Stakeholder,) in these roles, as they are working with distressed young adolescents, and emphasized the importance of promoting self-care amongst providers.
Training and Supervision NeedsThe EASE training package was perceived by providers and trainers/supervisors to be notably different from other MHPSS trainings. The strong focus on role plays was perceived to soundly prepare providers for eventualities in sessions and enhance their problem-solving skills for challenging scenarios. The focus on individual provider competencies, in terms of highlighting existing strengths and focusing on further development of specific competencies when needed, was considered highly effective. Some respondents advised that additional trainings could be helpful on topics including types of distress adolescents experience, communication skills, and complaint and reporting mechanisms. Furthermore, respondents reported that rather than one intensive 10-day training, it may be more effective if training were spaced out to make it less tiring for providers and trainers.
Many providers, trainers/supervisors, and MHPSS stakeholders stressed that regular group supervision sessions were important and allowed providers to share their experiences with a specialist supervisor. In parallel, individual coaching or follow-up with providers is needed. Variation in strategies used during supervision (e.g., role-plays) was considered helpful.
Individual coaching or the individual follow up is needed. So the supervision sessions do not mean if I’m doing the [group] supervision sessions, that doesn’t mean I need to make the individual follow up less (MHPSS stakeholder)
Theme 4: Looking Forward-Considerations for Scaling Up EASEWhile the previous themes and sub-themes investigate implementation factors that can facilitate or hamper intervention delivery, this theme focusses specifically on findings regarding planning for future scale up of EASE in Lebanon, including structural and contextual challenges.
Need for EASE to Bridge the Care GapInterviewees, including providers, outreach workers, trainers/supervisors, and stakeholders, stressed that there is a significant need for focused psychosocial support services like EASE for children and adolescents in Lebanon.
EASE was reported to be well designed to meet this need, particularly due to the different levels of distress that people face in Lebanon. The recent successive crises (economic crisis, COVID-19 pandemic, and Beirut blast) have impacted basic needs, security, mental health, and wellbeing of the whole population. This has exacerbated the need for MHPSS interventions.
Now regarding what is happening with Lebanon, it is being crises, political and everything I mean, I feel EASE, it is the time now (outreach worker, female)
Target Group CriteriaWhen reflecting on who EASE should be offered to, there appeared to be a consensus that EASE should be delivered to young adolescents of all nationalities and not focused only on refugee or migrant communities, given the stressors that all young people in Lebanon are facing. Furthermore, some respondents emphasized the need to ensure the inclusion of the most vulnerable adolescents, including working adolescents, those living in Palestinian camps, and those with disabilities. Respondents noted that youth are most impacted by the country’s decline, and stakeholders stressed the need to expand the age range of EASE, considering the mental health needs of older adolescents and young adults, although this may require substantial adaptation of the EASE intervention.
Coordination to Implement EASEThe majority of interviewed stakeholders stressed that EASE “cannot be a stand-alone” intervention (MHPSS stakeholder, female). EASE has to be complementary to other provided services such as educational, recreational, or health care packages. Different interviewees stated that it is important to embed EASE delivery within “structures that are sustainably available” (MHPSS stakeholder, female), such as training at local universities, and delivering in schools, primary healthcare or community mental health centers, grass root organizations, and the referral pathways at the national level. EASE implementation should be in coordination with the overall mental health system in the country, child protection actors, Ministries of Public Health and Social Affairs, and the MHPSS Taskforces. Given the rapidly changing context in Lebanon, the need is not only to implement such an intervention, but also to maintain it longer term, and this would require coordination with other services. Additional support for adolescents requiring more specialized services may be needed as well, and this would require working together with tertiary providers. Some stakeholders additionally emphasized that integrating EASE with existing health or other services is a way to avoid stigma surrounding mental illness.
Quality Assurance and AccountabilitySome respondents stressed the importance of having a system in place to ensure quality implementation and accountability and provided examples of minimum activities needed including regular training on relevant topics and competencies for providers; strong supervision with a specialist supervisor; regular coordination meetings and support for the implementation team; clear processes and guidelines, standard operating procedures, terms of references for each role; clear framework for responding when any responsibilities are breached; monitoring tools for the intervention; and clear reporting lines. Providers felt that having a “monitoring system with complaint mechanisms” is important, alongside setting key performance indicators to monitor and deliver feedback for them in their work.
[For] the intervention to sustainably be maintained with quality, there should be a system around it. There should be a system that guarantees proper training of these providers, proper support (MHPSS Stakeholder)
Lack of Financial ResourcesMost stakeholders and trainers/supervisors emphasized that scaling up is likely to be hindered by lack of financial resources. Government funding for mental health is a major challenge in the context of the economic crisis and political situation, with many competing priorities. International mental health funding is limited, and not a sustainable solution. However, some stakeholders were optimistic and mentioned that the worsening situation in Lebanon might lead to more international interest and funding opportunities for MHPSS interventions including EASE. Nonetheless, lack of sustainable funding pathways was emphasized as a major barrier to scaling up EASE.
留言 (0)