The current report describes a unique synchronous metastatic malignant struma ovarii and cervical PTC after six years of follow-up, alongside molecular analysis that revealed positive RET/PTC1 rearrangement among three different sites, i.e., malignant struma ovarii, cervical thyroid gland, and abdominal wall metastasis.
The coexistence of malignant struma ovarii and cervical thyroid carcinoma is quite rare. Among previous reports, we found eighteen publications that described synchronous malignant struma ovarii and cervical thyroid carcinoma. The characteristics of these reports are shown in Table 2, and treatment and follow-up data are also available in Table 3.
Table 2 Coexistence of malignant struma ovarii and cervical thyroid carcinoma case reports characteristics
Table 3 Coexistence of malignant struma ovarii and cervical thyroid carcinoma treatment and follow-up
The mean diagnosis age of synchronous malignant struma ovarii and cervical thyroid cancer was 48.26 years (range from 30 to 78 years), and most patients complained about abdominal/pelvic symptoms at the onset of the disease. Nevertheless, two patients [11, 19] suffered from neck problems, and the post-total thyroidectomy 131I scan demonstrated the struma ovarii diagnosis. According to pathological evaluation, PTC was the most common histologic subtype in malignant struma ovarii and cervical thyroid gland. Furthermore, molecular analysis was documented in eight reports [2, 7, 8, 10,11,12,13,14]. BRAF (V600E) mutation was the most common genetic evaluation, followed by RAS, KIT, TERT promoter mutations, and RET-PTC rearrangements. However, all evaluation results were negative except for RAS mutations in Gomes-lima et al. [8] and KIT mutation in Ma et al. [10]. Moreover, most patients underwent a similar treatment approach; unilateral or bilateral salpingo-oophorectomy, total thyroidectomy, and RAI ablation. Follow-up data were also available for twelve patients, and the average follow-up time was 23.15 months (range of 6 to 60 months) with no evidence of recurrence or distant metastasis.
The coexistence of malignant struma ovarii and cervical thyroid carcinoma represents synchronous multifocal thyroid-type tumors in distinct anatomical locations without lymphatic connection. This phenomenon may be explained by hypothesized “field cancerization” and early genomic instability. “Field cancerization” or “field effect” refers to prolonged exposure to carcinogens leading to independent genetic alterations at thyroid-type tissue in different topographical sites. On the other hand, the initial genetic instability occurs during embryogenesis, and separated affected cells differentiate into thyroid-type tissue in distinct anatomical locations. Then, lifetime parallel carcinogen exposures lead to independent synchronous tumorigenesis. In other words, genetic predispositions, environmental exposure, and epidemiological factors contribute to multiple preneoplastic lesions arising synchronously [2, 20,21,22].
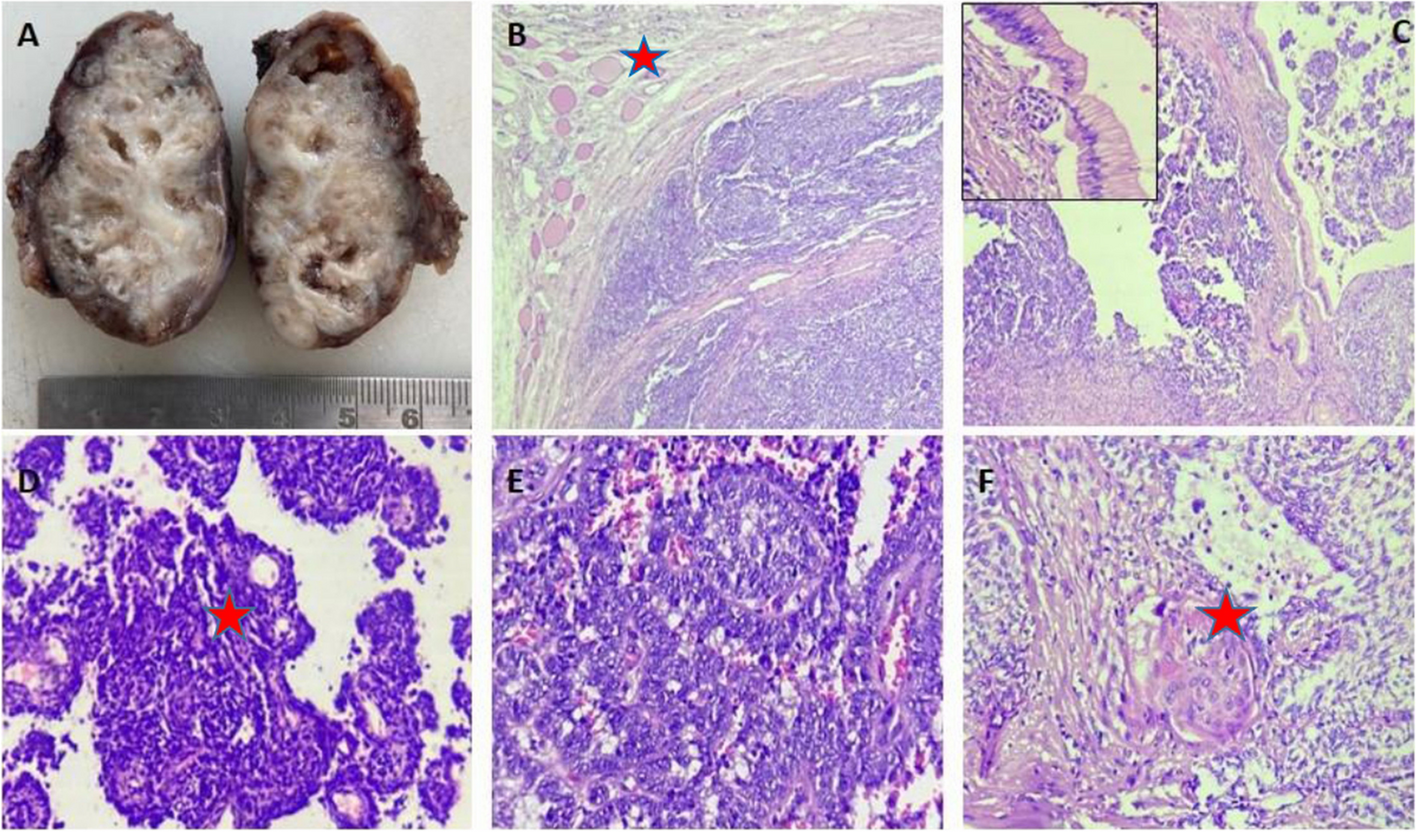
To our best knowledge, only one report presented the coexistence of metastatic malignant struma ovarii and cervical PTC alongside molecular analysis. Leong et al. [2] described a 42-year-old woman with a growing left pelvic mass that underwent total abdominal hysterectomy and bilateral salpingo-oophorectomy. The pathological evaluation revealed papillary thyroid carcinoma arising from struma ovarii, alongside the existence of thyroid-type tumor cells in the peritoneal washing fluid. Then, the total thyroidectomy histological evaluation illustrated bilateral and multifocal PTC along with extrathyroidal extension and metastasis to the perithyroidal lymph node. Similar to Leong et al. study, our patient’s disease presented by abdominal manifestation, then she underwent the same treatment approach, and pathology evaluation revealed PTC among struma ovarii, cervical thyroid gland, and abdominal wall metastasis. Moreover, in contrast to the study of Leong et al., cervical thyroid histological evaluation demonstrated no evidence of extrathyroidal extension or lymph node metastasis, and our patient’s distant metastasis occurred in the abdominal wall, which was not a common site for malignant struma ovarii metastasis. Furthermore, to explore genetic alterations, Leong et al. evaluated BRAF(V600E) and KRAS mutations and RET/PTC 1 and 3 rearrangements, and all results were negative. Conversely, we performed BRAF(V600E), NRAS mutations, and RET/PTC 1 rearrangement among malignant struma ovarii, cervical thyroid gland, and abdominal wall metastasis, and RET/PTC 1 rearrangement was found among all affected tissues. Finally, there was no evidence of recurrence or metastasis during the one-year follow-up of the Leong et al. study and the six-year follow-up of our study.
RET/PTC is defined as intrachromosomal rearrangement of the long arm of chromosome 10. According to previous studies among PTC patients, the incidence of RET/PTC rearrangements was 2.5–67% and had a relatively high prevalence in radiation-induced PTC [23, 24]. Furthermore, RET/PTC rearrangements were associated with advanced tumor stage and a higher risk of distant metastasis [25]. However, the prognostic role of RET/PTC rearrangement in PTC still meets with controversy [23]. Reviewing previous publications, we found only two reports documented RET/PTC rearrangement in struma ovarii; first, Elisei et al. [26] reported a benign struma ovarii with RET/PTC 3 rearrangement in a 59-year-old woman. Second, Boutross-Tadroset et al. [27] described seven RET/PTC rearrangements in follicular variant of PTC within malignant struma ovarii, one patient with RET/PTC 3 and others with RET/PTC 1. To our best knowledge, we present the first RET/PTC 1 rearrangement report in synchronous metastatic malignant struma ovarii and cervical PTC in a patient without previous radiation exposure.
The strength of the current study was a quite rare case of synchronous malignant struma ovarii with abdominal wall metastasis and cervical PTC, along with detection of RET/PTC 1 rearrangement in molecular analysis and a long period of follow-up. Regardless of these strengths, our study had some limitations. First, we did not evaluate other RET/PTC rearrangements and clonal origins of the tumors. Second, immunohistochemistry results were not available.
In conclusion, considering the rarity of synchronous malignant struma ovarii and cervical thyroid carcinoma, finding malignant struma ovarii might be a clue to probable cervical thyroid cancer. Hence, examinations and imaging of the cervical thyroid gland should be considered among malignant struma ovarii patients. Moreover, the post-diagnosis molecular analysis could provide helpful information for understanding the underlying mechanism of coexisting disease, the clinicopathological behavior of the tumors, and the patient’s prognosis.







留言 (0)