

記住我









Globally, the health workforce crisis is a common phenomenon that challenges the healthcare systems’ function (1, 2). Shortage of health workers, poor training modalities, maldistribution of human resources, and poor management of health professionals turnover constitutes a serious challenge for hospitals (1, 3). Workplace hardship in the health delivery set-up may result in professional burnout and poor ‘resilience at work’ (RaW), significantly challenging the health care system’s functioning (4). Clinical personnel who lack self-compassion and mindfulness frequently suffer from burnout and lower levels of RaW that impair the capacity to overcome difficulties (5).
Although there are no generally accepted definitions of burnout, the most commonly agreed definition is an extended exposure to chronic personal and interpersonal stressors on the job as characterized by three dimensions: exhaustion, depersonalization, and professional inefficacy (6). According to Christina Maslach et al., “emotional exhaustion” (EE) is described as the feeling of not being able to offer any more of oneself at an emotional level; “depersonalization” refers to a distant attitude toward work, the people being served by it and among colleagues; and “professional inefficacy” describes the feeling of not performing tasks adequately and of being incompetent at work (7).
Many medical professionals suffer from burnout, which is the psychological syndrome involving emotional exhaustion, feelings of helplessness, depersonalization, negative attitudes toward work and life, and reduced personal accomplishment (PA) (8). Burnout affects the quality-of-service delivery and exacerbates professional shortages in the health system by causing dropout from the place of work and/or profession (9–11).
Burnout is a protracted response to chronic and interpersonal stressors on the job (12), that has negative implications for job performance and social relationships (13). The level of burnout among medical professionals is nearly twice that of non-physician professionals (14). Burnout occurs when health professionals use ineffective coping strategies to protect themselves from work-related stress (15). Developing professional resilience may become an important strategy to minimize emotional distress, burnout, and work dropout. Many personal and demographic factors affect the medical personnel’s level of RaW.
According to Cooper et al., “resilience” is the ability of an individual to positively adjust to adversity, and can be applied to building personal strength (16). According to King et al. (17), resilience is the way individuals, groups/teams, and organizations respond to facing challenges and adversity. Southwick et al. (18) also defined resilience as “the capacity of a dynamic system to withstand or recover from significant disturbances.” It includes the steady trajectory of healthy functioning after an extremely hostile event.
In reliance on varied definitions of resilience, the term ‘resilience at work’, was also described as a dynamic capability that can allow individuals to thrive on challenges, given appropriate social and personal dimensions in their workplace (19). These dimensions include self-efficacy, self-control, the ability to engage in support and help, learning from difficulties, and persistence despite blocks to progress (20). Another definition of ‘resilience at work’ defined by Milton, was a “positive developmental trajectory characterized by demonstrated competence in the face of, and professional growth after, experiences of adversity in the workplace” (Page 3) (21). Resilience at work’ is an important attribute and one which can be learned and improved upon (22, 23).
Burnout is associated with health professionals facing unprofessional behavior, thoughts of suicide, retirement prematurely from their work, and errors during patient care (24). High stress and burnout reduce working performance and recovery from challenges, while highly resilient employees were found to be less affected by variations in working recovery (25, 26).
Ethiopia has been affected by a shortage of health professionals as well as high levels of professional burnout and low levels of resilience among healthcare workers. In response to the critical shortage of human resources in the healthcare system, the Government of Ethiopia invested significant resources in the effort to increase the quantity of the healthcare workforce, utilizing a ‘flood-and-retain strategy’. This strategy involves an accelerated and voluminous increase in the number of students studying health professions. In this regard, the number of health science colleges, as well as the enrollment of health professionals into higher institutions, has been increasing in the last 15 years (27). However, how many of those health professionals are resilient at work is to date not well known.
Therefore, this study is aimed to examine the level of burnout and ‘resilience at work’ among health professionals who are working at the obstetric/gynecologic and surgical care departments inTibebe-Ghion and the University of Gondar comprehensive Specialized referral Hospital (UoGSRH) in Ethiopia. The measurement will enable both the scientific realm and policymakers to understand the current level of burnout and RaW in the setting of a low socio-economic society and highlight components that should be managed to enhance the development of a more resilient healthcare system.
2. Materials and methods 2.1. Type of study and its coursesA facility-based, cross-sectional, quantitative study was conducted at two public teaching hospitals located in the Amhara region of Ethiopia (Tibebe-Ghion and Gondar teaching hospitals).
2.2. Investigated institutionsBahir Dar University College of Medicine and Health Sciences was established in 2007 and is one of the youngest medical training institutions in Ethiopia authorized to provide medical and health professionals training in the past 10 years. The hospital that provides both teaching and clinical services under the college of medicine and health science is known as Tibebe-Ghion Campus. The hospital provides both outpatient and inpatient care services, with over 452 beds. A total of 621 health professionals, 128 intern general practitioners, and 211 residents are currently working in the hospital. The surgical and gynecological care department of the hospital consists of 167 clinical staff, of which 25 nurses and 28 surgeons work in the surgical care department. The rest (69 midwifery nurses and 19 gynecologists and obstetricians) work in the gynecologic department. Additionally, 26 different-level anesthesia providers currently work in the two departments.
The second study institution is the UoGSRH which is a teaching hospital under the Gondar University College of Medicine and Health Sciences; established in 1954. UoGSRH is one of the largest specialized hospitals in Ethiopia, with over 540 beds. A total of 986 clinical staff, 141 intern general practitioners, and 243 residents currently work in the hospital. The surgical and gynecological care departments of the hospital consist of 245 health professionals of which 37 nurses and 41 surgeons work in the surgical care department. The rest (101 midwifery nurses and 28 gynecologists and obstetricians) work in the gynecologic department. Additionally, 38 different-level anesthesia providers currently work in the two departments.
2.3. Study populationThe study population included all physicians and residents from the surgical, gynecologic, and obstetric (Gyn/Obs) departments. Midwifery, anesthetic, and all other nursing specialties who are working in the operative sites of the aforementioned hospitals.
Health professionals who are planning to leave their institution due to completion of their residency program, intend to attend a training program in other hospitals, or due to any other reasons within the upcoming 2 years, were excluded from the study. Based on these eligibility criteria, a total of 412 clinical personnel (167 from Tibebe-Gion and 245 from UoGSRH) were eligible for the survey.
2.4. Study variablesLevels of professional burnout (low, medium, high) and levels of resilience at work (low, medium, high) were defined as the dependent variables. The type of profession, work experience, and demographic characteristics were collected as independent variables. Family size, income per family size, and behavioral factors such as chat chewing and cigarette smoking were examined as confounder variables.,
2.5. Study tool and reliabilityTo assess the health professionals’ burnout level, Maslach’s burnout inventory human service survey (MBI-HSS), a tool consisting of 22 items was used. The tool comprises emotional exhaustion (9 items), personal accomplishment (8 items), and depersonalization (5 items) with a seven-point response scale (0 to 6), ranging from 0 = never to 6 = daily (28). The total scores of each dimension were summed and categorized as low, moderate, or high, and the average score was also calculated. The cut-off point score for health personnel’s burnout was as follows: Emotional exhaustion: low (≤16), moderate (17–26), high (≥27); Personal accomplishment: low (≤33), moderate (29–34), high (>39); and Depersonalization: low (≤5), Moderate (6–9), High (≥10). Overall burnout (burnout syndrome) was considered when a health provider displayed high levels of emotional exhaustion and/or depersonalization and low levels of personal accomplishment (35, 36). In this study, the internal consistency of the MBI tool was checked. The overall internal consistency of the 22 items was high (Cronbach’s α = 0.87). Similarly, the domain-specific internal consistency was high for all three components, as follows: EE (Cronbach’s α = 0.89), Depersonalization (Cronbach’s α = 0.85), and PA domains (Cronbach’s α = 0.81).
Resilience at work was measured by using the Win wood ‘resilience at work’ measuring tool” (37). The tool consists of 20 items, classified into seven components with a seven-point response on a Likert scale (0 to 6), ranging from 0 = strongly disagree to 6 = strongly agree. The seven components are; Living authentically (three items), Finding one’s calling (four items), Maintaining perspective (three items), Managing stress (four items), Interacting cooperatively (two items), Staying healthy (two items), and Building networks (two items) (37). The total score of the scale was calculated to obtain a composite resilience value. The levels of resilience at work were calculated using the mean scores. Mean was used to determine whether the current score is lower, consistent, or higher than Win wood’s means core; participants who scored below 61, 61–81, and above 81 were considered as having a low, moderate, and high level of ‘resilience at work’ respectively (29, 38, 39). The internal consistency of the ‘resilience at work’ assessment tool was also assessed, which was high (Cronbach’s α = 0.89).
2.6. Study designAn English version of a self-administered structured questionnaire was used to collect the data on health professionals’ burnout and ‘resilience at work’. Before the actual data collection, the questionnaire was pre-tested among 20 health professionals (5% of the total sample). The pre-test study was conducted in other hospitals (not sampled in the study) that have similar characteristics to the main study participating hospitals.
Four data collectors and two supervisors participated in the data collection process. Intensive training was provided for the data collectors and supervisors before the data collection began. During the training, the trainers gave instructions concerning the questions to be asked, their meaning, ways to ask them, and how to record the answers. Both electronic and hard-copy survey tools were used to fill in the data. The hard copy was used for those participants who lack electronic access or were not interested in using it. The electronically filled data was uploaded directly to excel and exported to the statistical package for social sciences (SPSS, version 23) software for analysis. The hard-copy filled data were entered directly into SPSS-23.
The data collectors approached the respondents by self-introduction, explaining the objectives of the study as well as their autonomic participation in the study. After informed consent was received from each respondent, the questionnaire was distributed by one of the two data collection means. Furthermore, the data collectors supported respondents who needed further assistance during detailing and checked for any missing or incomplete information. For data collected using a hard copy, any missing or incomplete data were corrected by re-collecting the correct information before leaving the respondent.
During the data collection process, the supervisors traveled with the data collection teams, to observe and ensure that their teams provide self-introduction, and explain the objectives of the study, stressing the confidentiality of the information, and the anonymity of participating in the study. Moreover, the supervisors followed the data collectors to take informed consent from each respondent. They also checked and assisted if any additional training or clarifications were needed. Furthermore, the principal investigator checked all the data that was submitted from the field every other day and communicated as needed with the supervisors.
2.7. Data analysisThe collected data were checked for completeness and consistency. Consequently, the data was compiled, cleaned, coded, and then exported/entered into SPSS version 23 for analysis. A descriptive analysis was conducted to summarize the findings. Descriptive statistics comparison was done using a t-test and one-way analysis of variance (one-way ANOVA). Simple linear regression analysis was applied to select the candidate variables for the multiple linear regression model. To control the confounding effect, a variable with a value of p ≤0.2 on a simple linear regression was taken as a candidate variable for multiple linear regression. Multiple linear regression analysis was done via the enter method to identify the independent predictors for burnout for each dimension separately and for the RaW. value of p <0.05 on multiple linear regression analysis was declared a statistically significant predictor for each burnout dimension and resilience and unstandardized-β was used for interpretation. Multiple linear regression assumptions (normality, linearity, and constant variance) were checked. Linear-correlation analysis was used to test the correlation between the three dimensions of burnout and ‘resilience at work’. Additionally, t-test and one-way ANOVA were employed to test the differences in each burnout dimension and ‘resilience at work ‘according to the participants’ demographic and work-related characteristics.
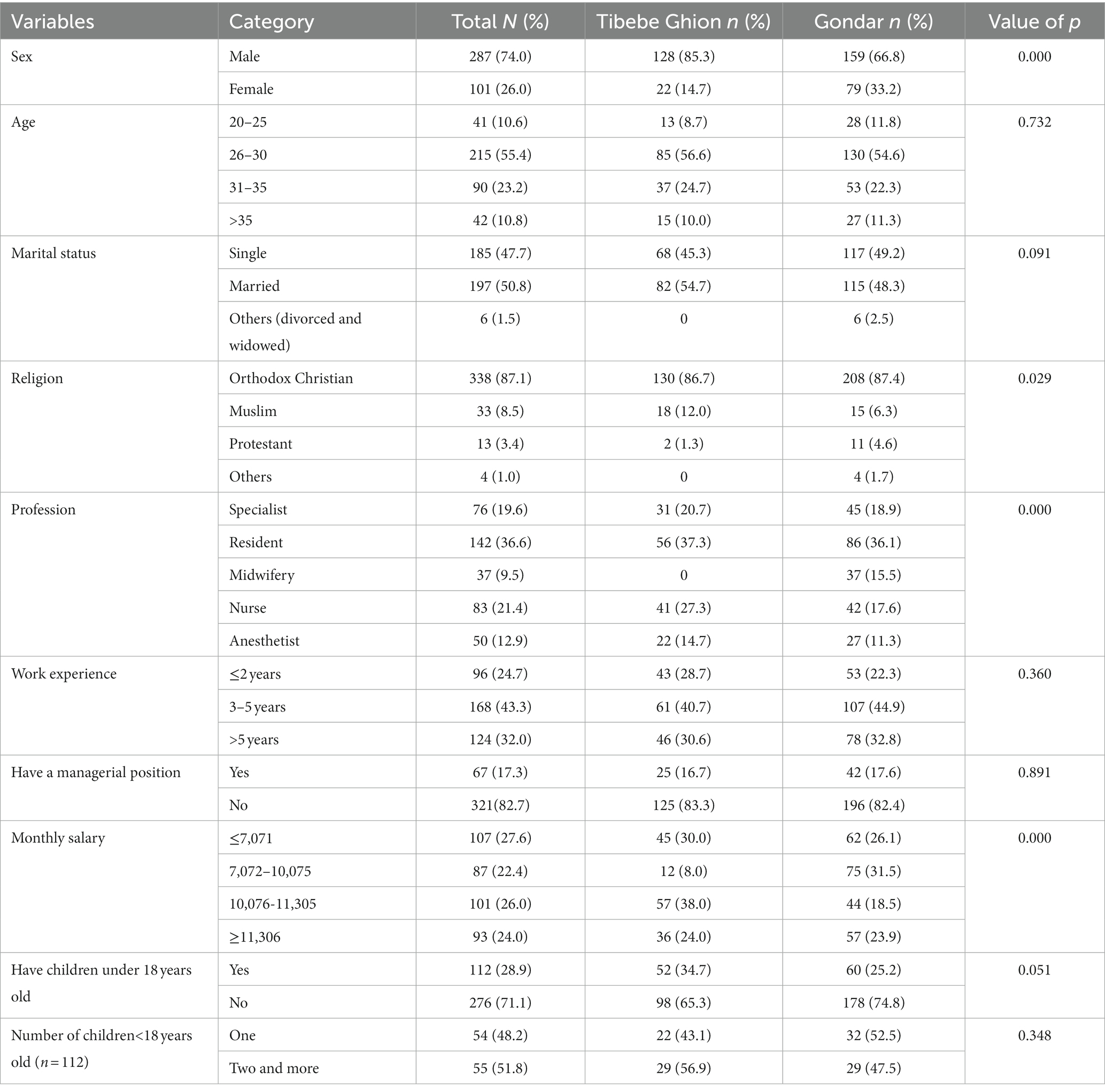
3. Results 3.1. Participants’ socio-demographic characteristicsA total of 388 health professionals participated in the survey with a response rate of 94.2%. Around three-fourths of the respondents, 287 (74.0%) were male. The median age with Interquartile Range (±IQR) of the respondents was 29 (±5) years of age, which ranged from 20 to 49 years. Almost half of the participants, 197 (50.8%) were married. Three hundred thirty-eight (87.1%) respondents were Orthodox Christian followers. Professionally, more than one-third, 142 (36.6%) of the respondents were residents, and 264 (68.0%) respondents have 5 years or below of work experience. The average salary of the respondents in Ethiopian Birr (EBR) was 10,653.6 with a standard deviation (SD) of ±4532.7, while 194 (50.0%) respondents had a monthly salary of 10,075EBR or below (Table 1).
Table 1. Socio-demographic characteristics of health personnel working at the surgical care department; tertiary hospitals, North-West Ethiopia, 2021 (n = 388).
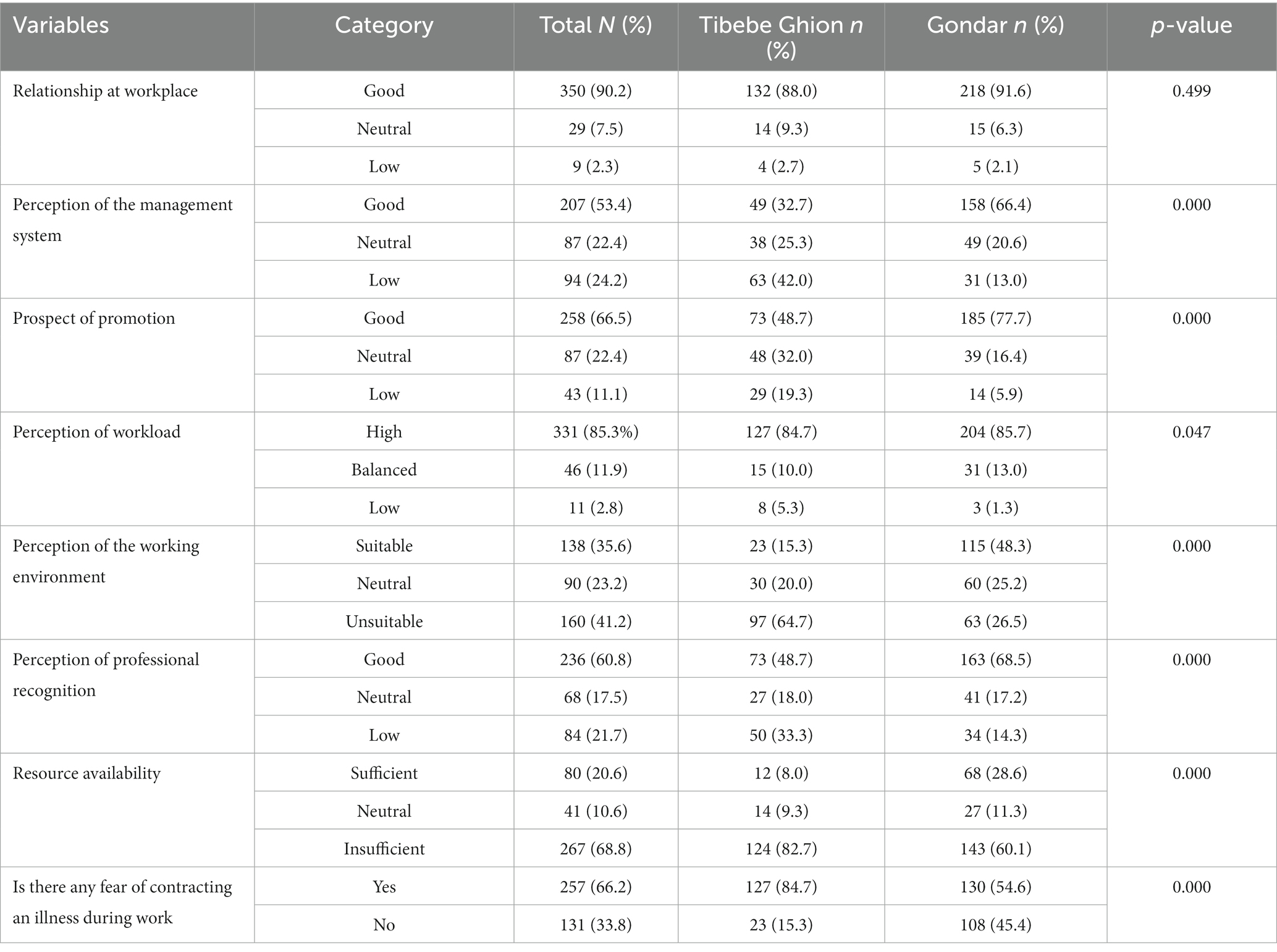
3.2. Working environment-related characteristicsA majority (N = 379, 97.7%) of the respondents reported that they have a good or neutral relationship at work. Three-hundred thirty-one (85.3%) respondents perceived that there is a high workload, while 294 (75.8%) respondents had good or neutral perceptions of the existing management system in their hospitals. Regarding the perception of the working environment, 250 (64.4%) of the respondents have neutral or unsuitable perceptions. More than two-thirds, (N = 257, 66.2%) of the respondents reported that they fear contracting an illness during work (Table 2).
Table 2. Working environment-related characteristics of health personnel working at the surgical care department; tertiary hospitals, North-West Ethiopia, 2021 (n = 388).
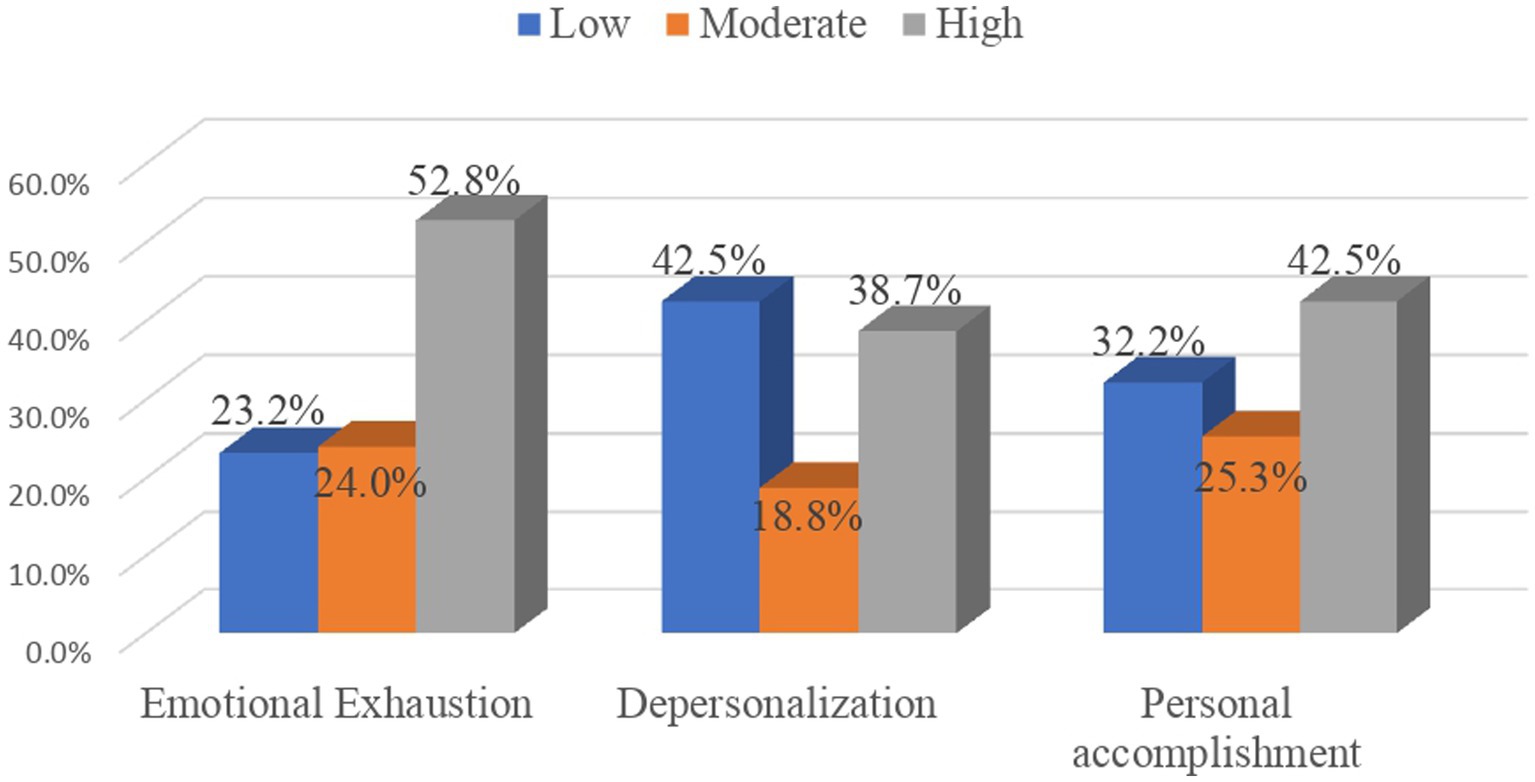
3.3. Magnitude of burnoutBurnout syndrome was shown among 101 (26.0%) study participants; which means they displayed high burnout in emotional exhaustion and/or depersonalization and low personal accomplishment, and 318 (82.0%) of them experienced burnout for at least one dimension. Furthermore, 205 (52.8%), 150 (38.7%), and 125 (32.2%) participants presented high emotional exhaustion, high depersonalization, and low personal accomplishment respectively, i.e., displayed a high level of burnout (Figure 1). The participants’ mean score with standard-deviation (±SD) of emotional exhaustion, depersonalization, the personal accomplishment was 27.28 ± 12.67, 9.78 ± 7.93, and 36.19 ± 7.80, respectively.
Figure 1. Maslach burnout subscale levels among health personnel working at the surgical care department; tertiary hospitals, north-west Ethiopia, 2021 (n = 388).
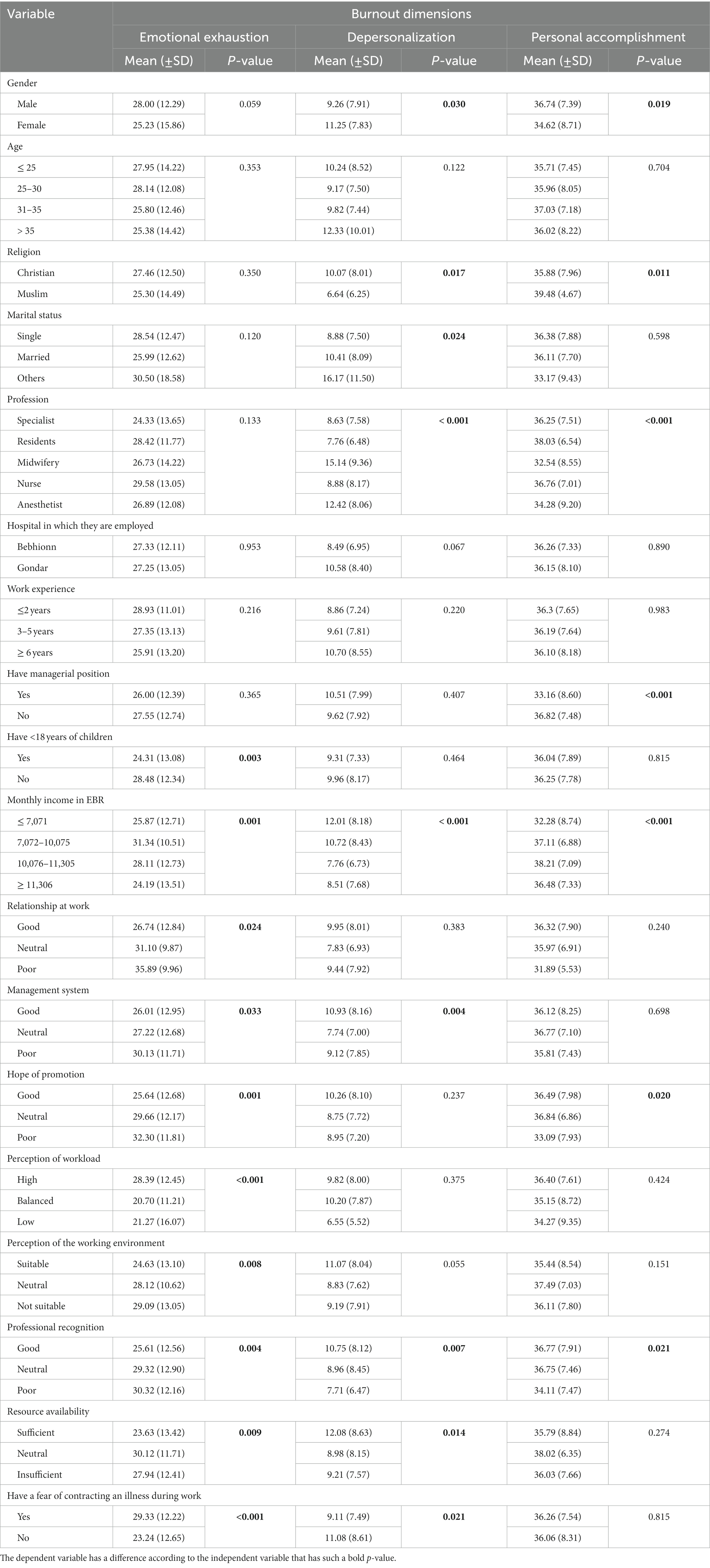
3.4. Comparison of burnout sub-scales according to participants’ demographic characteristicsTable 3 shows the comparison of the participants’ burnout levels according to the demographic and work-related variables.
Table 3. The mean score of the three burnout dimensions based on the participants demographic and work-related variables of health personnel working at the surgical care department; tertiary hospitals, North-West Ethiopia; 2021 (n = 388).
Using the independent t-test statistical analysis, a higher mean score of emotional exhaustion was found among participants who did not have children under 18 years compared to those who had such young children (28.48 ± 12.34 vs. 24.31 ± 13.08 respectively; p < 0.01). The analysis of variance (ANOVA) showed a significant difference in the mean score of EE by participants’ monthly income; most especially, the difference was noted between respondents whose monthly income was above 11,306 EBR or between 7,072–10,075 EBR (24.19 ± 13.51 vs. 31.34 ± 10.51 respectively; p < 0.01). Participants who had a poor relationship at work had a higher mean score of EE compared to those who had a good relationship at work (35.89 ± 9.96 vs. 26.74 ± 12.84 respectively; p = 0.024). A high mean score of EE was also observed among participants who had a high perceived workload compared to those who had a low perceived workload (28.39 ± 12.45 vs. 21.27 ± 16.07 respectively; p < 0.01). Moreover, participants who had poor hope of promotion had a high EE mean score compared to those who had good hope of promotion (32.30 ± 11.81 vs. 25.64 ± 12.68 respectively; p < 0.01). Relatively, a higher EE mean score was found among males compared to females (28.00 ± 12.29 vs. 25.23 ± 15.86 respectively) but this difference was not found to be significant (p > 0.05). The mean score of EE did not show a significant difference by the type of hospital in which the clinicians were employed (27.33 ± 12.11 for Tibebe-Ghion vs. 27.25 ± 13.05 for Gondar; p > 0.05).
Burnout levels in the dimension of depersonalization were higher among females compared to males (11.25 ± 7.83 vs. 9.26 ± 7.91 respectively; p = 0.030). The mean score of depersonalizations was also higher among Christians compared to Muslims (10.07 ± 8.01 vs. 6.64 ± 6.25 respectively; p = 0.017). There was a significant difference in the mean score of depersonalizations by profession; most especially the difference was observed between midwifery and residents (15.14 ± 9.36 vs. 7.76 ± 6.48 respectively; p < 0.01). A significant difference in the mean score of depersonalizations was also noted concerning the participants’ monthly income; particularly, these differences were noted between participants who received a monthly income below 7,071 EBR compared to those who earn 10,076–11305EBR (12.01 ± 8.16 vs. 7.76 ± 6.73 respectively; p < 0.01). However, the difference in the mean score of depersonalizations was not observed by the participants’ work experience, having children under 18 years old, relationships at work, and hope of promotion (p > 0.05).
Concerning burnout levels in the dimension of personal accomplishment, a higher mean score was reported among males compared to females (36.74 ± 7.39 vs. 34.62 ± 8.71 respectively; p = 0.019), and among Muslim religion, followers compared to Christians (39.48 ± 4.68 vs. 35.88 ± 7.96 respectively; p = 0.011). Significant differences in the mean score of PA were found according to the profession of the respondents; most especially the difference was noted between residents and midwifery as well as between specialists and midwifery (38.03 ± 6.54 for residents, 36.25 ± 7.51 for specialists’ vs. 32.54 ± 8.55 for midwifery; p < 0.01). The mean score of PA was lower among respondents who hold a managerial position compared to those who do not hold such positions (33.16 ± 8.60 vs. 36.82 ± 7.48 respectively; p < 0.01). Significant differences in PA mean score were also observed in participants ‘monthly income; most notably, it was lower among respondents whose monthly income was below 7,071 EBR compared to those whose monthly income was between 10,076–11,305 EBR (32.28 ± 8.74 vs. 38.21 ± 7.09 respectively; p < 0.01). From the work-related variables, there was a significant difference in the mean score of PA according to participants’ perceived hopes of promotion and professional recognition. Particularly, participants who have poor hope of promotion have lower levels compared to those who have good and neutral levels of hope (33.09 ± 7.93 vs. 36.49 ± 7.98 and 36.84 ± 6.86 respectively; p = 0.020). The same trend was identified among those who have a poor perception of professional recognition compared to those with a good perception (34.11 ± 7.47 vs. 36.77 ± 7.91 respectively; p = 0.021).
The three burnout domains were not found to be significantly different according to the participant’s age, work experience, or the hospital in which they are employed (p > 0.05; Table 3).
3.5. The magnitude of ‘resilience at work’ (RaW)The participants’ mean resilience at work score with standard deviation (±SD) was 78.36 ± 17.78. In this study, 53 (13.7%), 141 (36.3%), and 194 (50.0%) respondents have low, moderate, and high levels of resilience at work, respectively.
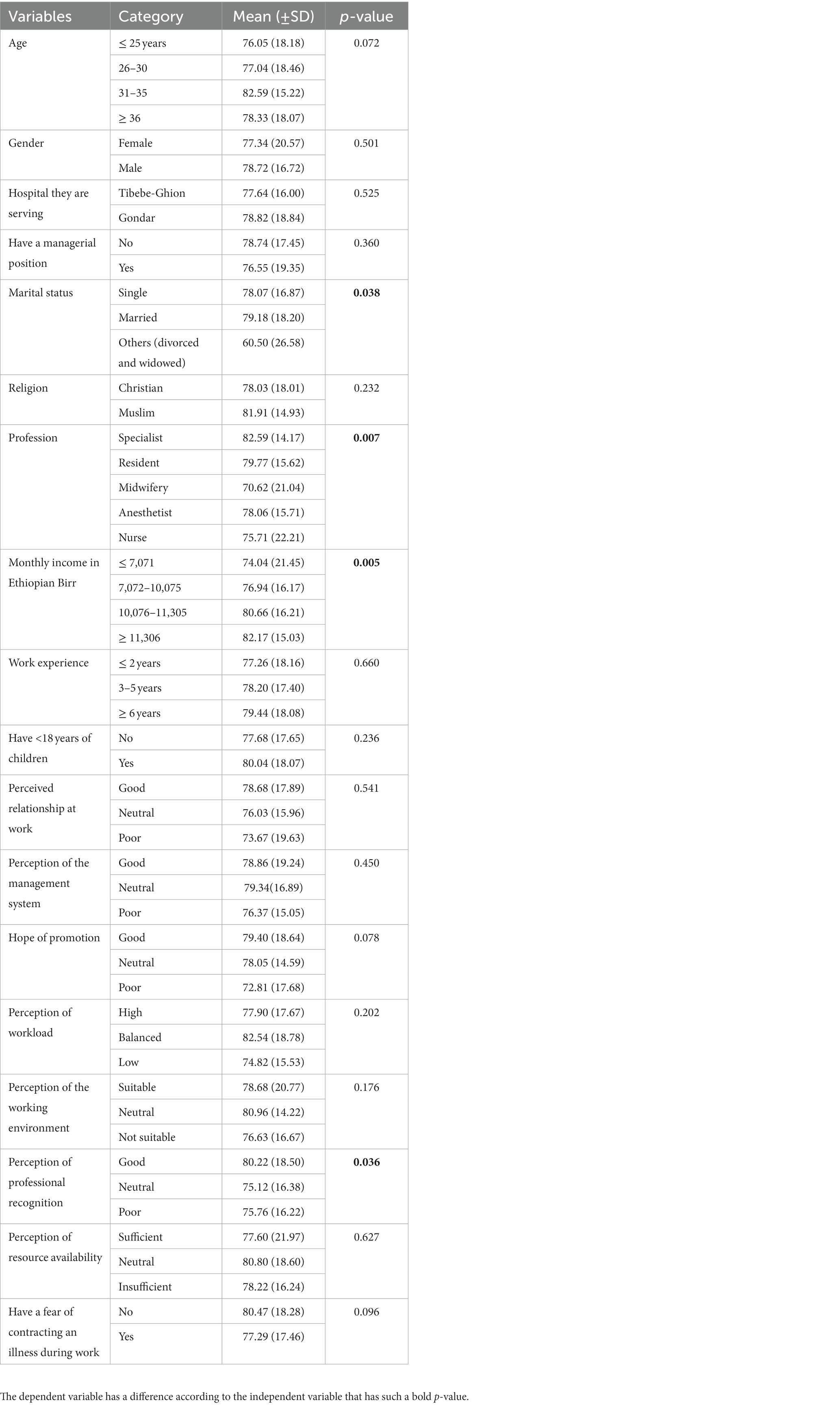
The mean resilience score has a significant difference across the participants’ marital status, profession, and monthly income. Married women have a high resilience mean score compared to those who are not married (either divorced or widowed together) (79.18 ± 18.20 vs. 60.50 ± 26.58 respectively; p = 0.038). Professionally, specialists have the highest (82.59 ± 14.17) resilience mean scores compared to other professionals, and the lowest level of resilience at work was found among Midwives (70.62 ± 21.04; p < 0.001). Similarly, the mean score of resilience was found to be higher according to the income level of the respondents. The mean score for income <7,071, 7,072–10,075, 10,076–11,305, and > 11,305 was 74.04 ± 21.45, 76.94 ± 16.17, 80.66 ± 16.21, and 82.17 ± 15.03 respectively; p < 0.01.
Resilience at work had no significant difference according to the hospital in which the clinicians are employed (77.64 ± 16.00 for Tibebe-Ghion vs. 78.82 ± 18.84 for Gondar hospital; p > 0.05). Relatively, the mean score of resilience at work was higher among participants in the age group between 31 and 35 years compared to those whose age was below 26 years (82.59 ± 15.22 vs. 76.05 ± 18.18 respectively; p > 0.05). Resilience at work had no significant difference by the sex of the respondents (77.34 ± 20.57 for females vs. 78.82 ± 16.72 for males; p > 0.05). Moreover, the score of resilience at work had no significant difference according to the respondents’ work experience, managerial position, workload, working environment’s suitability for work, and resource availability (p > 0.05; Table 4).
Table 4. Mean scores of RaW according to the participants’ demographic and working environmental-related variables of health personnel working at the surgical care department; tertiary hospitals, North-West Ethiopia; 2021 (n = 388).
3.6. Correlation between burnout sub-scales and resilience at workResilience at work was found to be associated with all three burnout dimensions (Pearson correlation between −0.139 to 0.479; p < 0.05). The Pearson correlation analysis showed that resilience at work has a negative association with emotional exhaustion and depersonalization, and in contrast, a positive association with the personal accomplishment burnout sub-scale.
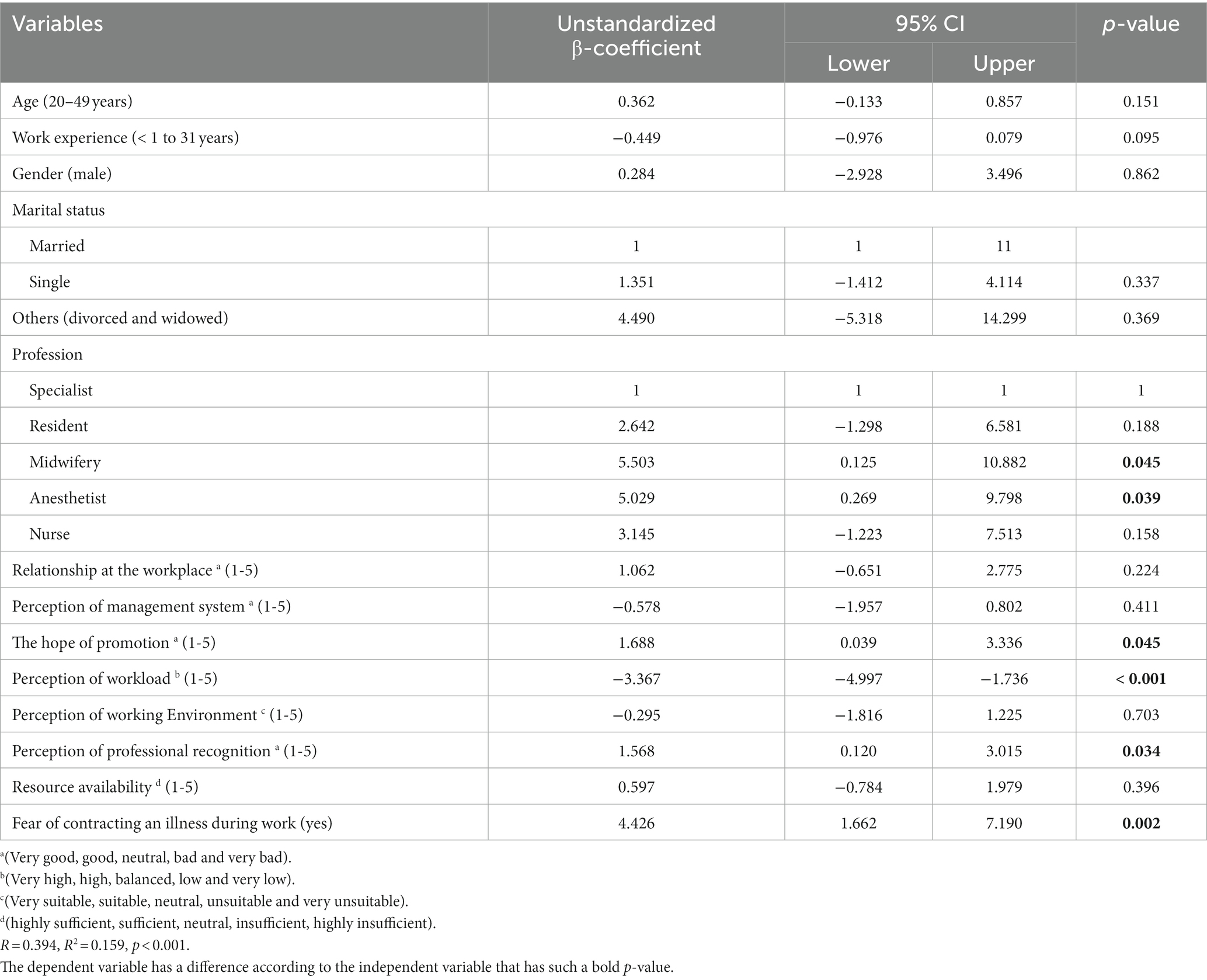
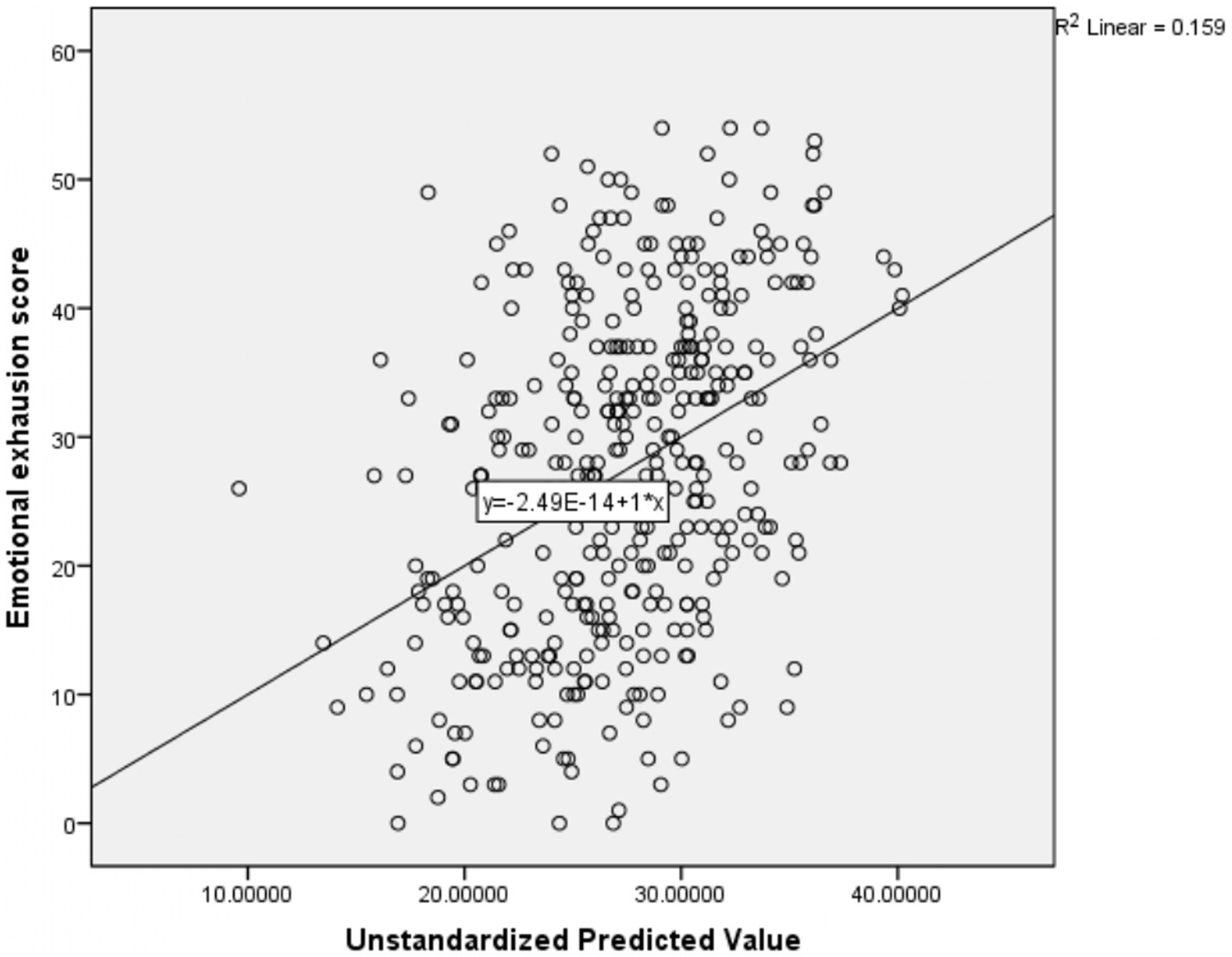
3.7. Factors associated with burnout and ‘resilience at work’ 3.7.1. Factors associated with emotional exhaustionMultiple linear regression results revealed that midwifery professionals [β: 5.503, 95%CI: 0.125, 10.882], anesthetic professionals [β: 5.029, 95%CI: 0.260, 9.798], the hope of promotion [β: 1.688, 95%CI: 0.039, 3.336], perception of professional recognition [β: 1.568, 95%CI: 0.120, 3.105] and fear of contracting illness during work [β: 4.426, 95%CI: 1.662, 7.190] were positively associated with the emotional exhaustion score. In contrast, the perception of workload [β: -3.367, 95%CI: −4.997, −1.736] was negatively associated with the emotional exhaustion score (Table 5). The R-square of this regression model was 0.159; which means that 15.9% of the dependent variable (emotional exhaustion) mean variation is explained by these independent variables collectively (Figure 2).
Table 5. Factors associated with emotional exhaustion among health personnel working at the surgical care department; tertiary hospitals, North-West Ethiopia; 2021 (n = 388).
Figure 2. Scatter plot showing the amount of mean variation of emotional exhaustion score explained by the independent variables together.
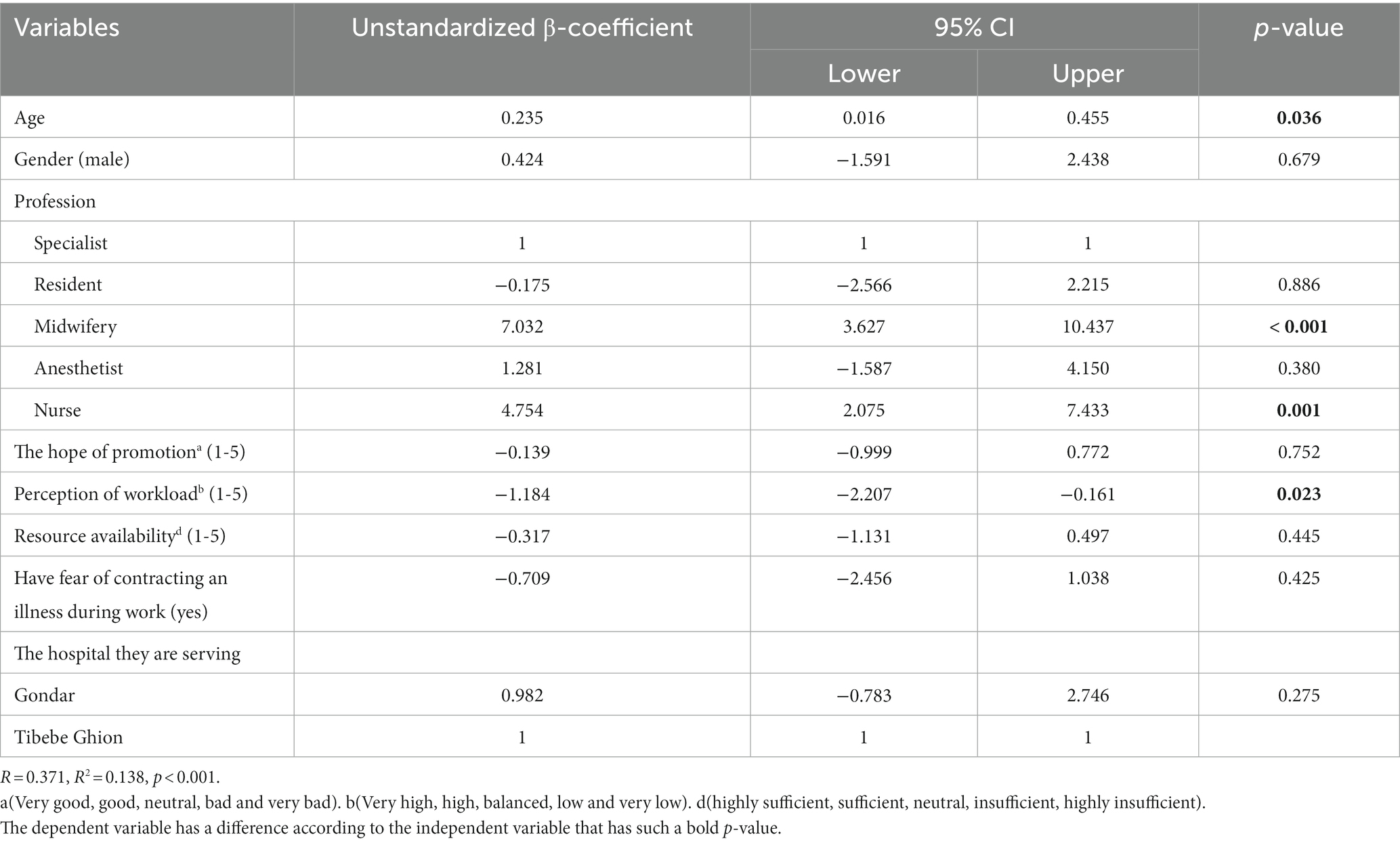
3.7.2. Factors associated with depersonalizationThe multiple linear regression results revealed that depersonalization was positively affected by the participants’ age [β: 0.235, 95% CI:0.016, 0.455] and professional type; midwifery [β:7.032, 95% CI: 3.627, 10.437], and nursing profession [β:4.754, 95% CI: 2.075,7.433]. Conversely, it was negatively affected by the participants’ perception of workload [β: -1.184, 95% CI: −2.207, −0.161] (Table 6). The R-square of this regression model was 0.138; these independent variables collectively explained 13.8% of the dependent variable (depersonalization) mean variation (Figure 3).
Table 6. Factors associated with depersonalization among health personnel working at the surgical care department; tertiary hospitals, North-West Ethiopia; 2021 (n = 388).
Figure 3. Scatter plot showing the amount of mean variation of Depersonalization score explained by the independent variables together.
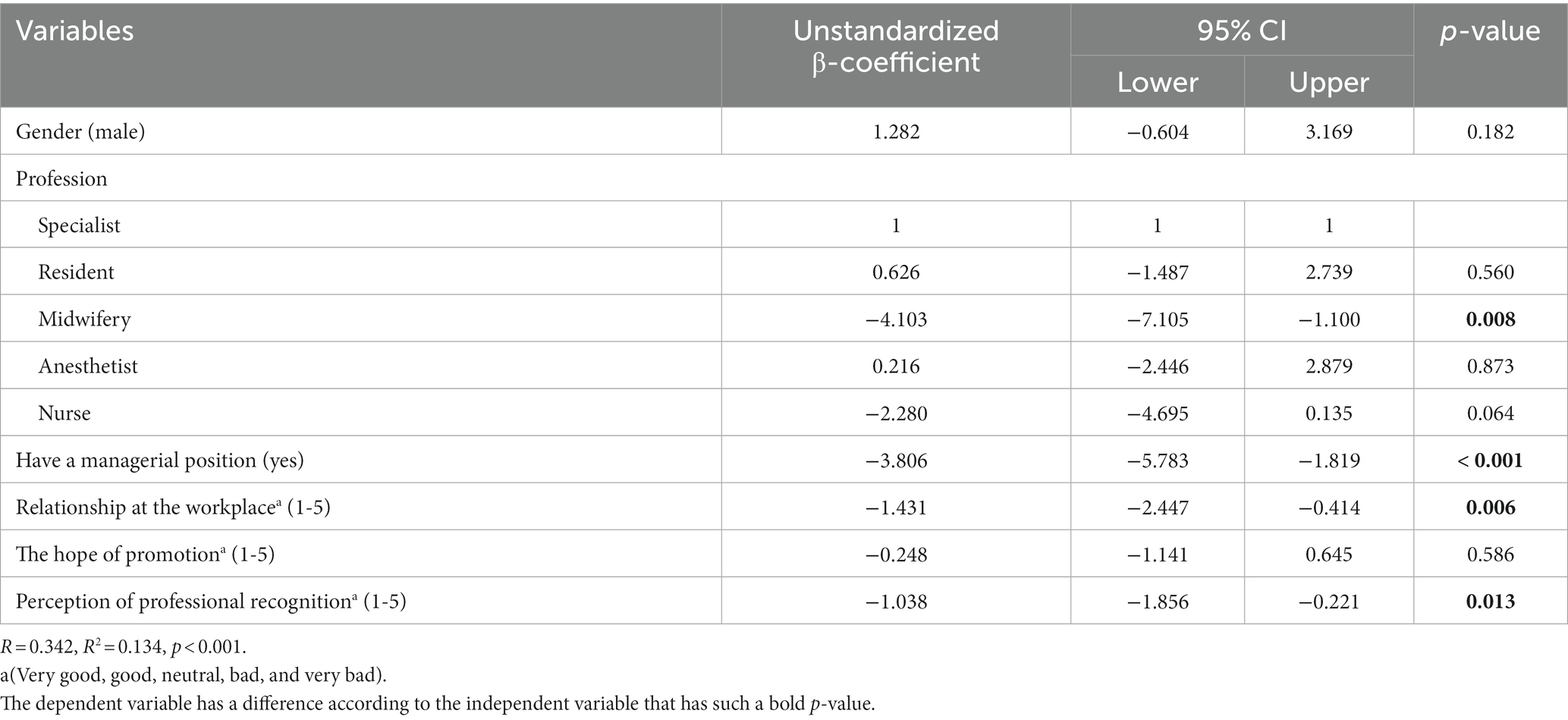
3.7.3. Factors associated with personal accomplishmentThe results of the multiple linear regression indicated that midwifery professionals [: -4.103, 95%CI: −7.105, −1.100], have managerial positions [: -3.806, 95%CI: −5.783, −1.819], relationship at workplace (very good, very bad) [β: -1.431, 95%CI: −2.447, −0.414], and perception of professional recognition (very good, very bad) [β: -1.038, 95%CI: −1.856, −0.221] were negatively associated with the personal accomplishment score (Table 7). The R-square of this regression model was 0.134; these independent variables collectively explained 13.4% of the mean variation of personal accomplishment (Figure 4).
Table 7. Factors associated with personal accomplishment among health personnel working at the surgical care department; tertiary hospitals, North-West Ethiopia; 2021 (n = 388).
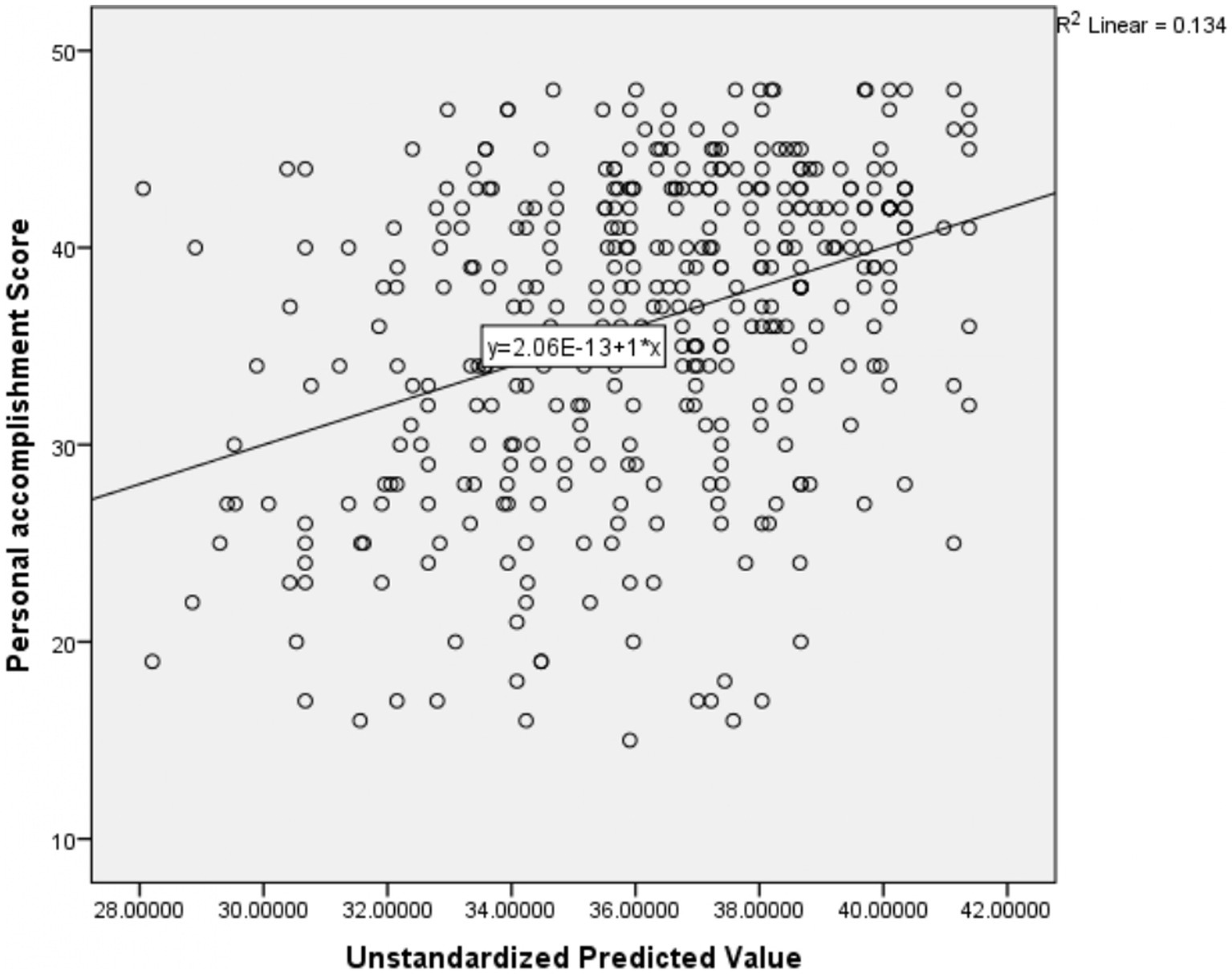
Figure 4. Scatter plot showing the amount of mean variation of personal accomplishment score explained by the independent variables together.
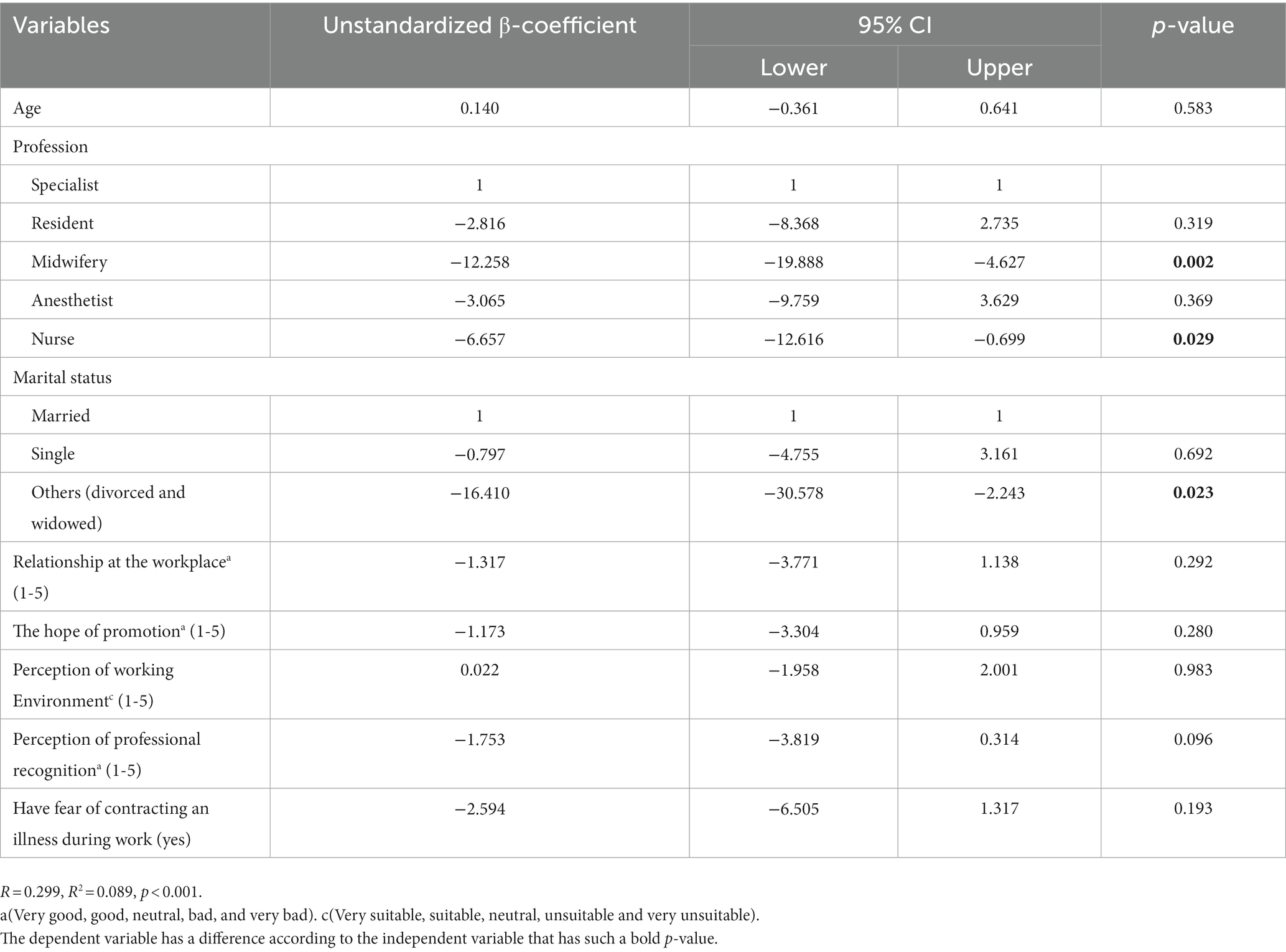
3.7.4. Factors associated with ‘resilience at work’The multiple linear regression results indicated that the level of ‘resilience at work’ was affected by the participants’ profession and marital status. Participants with midwifery [: -12.258, 95%CI: −19.888, −4.627], BSc nurse [β: -6.657, 95%CI: −12.616, −0.699], and others (divorced and widowed) marital status category [β: -16.410, 95%CI: −30.578, −2.243] were negatively associated with the participants ‘resilience at work’ score (Table 8). The R-square of this regression model was 0.089; these independent variables explained 8.9% of resilience at work mean variation score (Figure 5).
Table 8. Factors associated with ‘resilience at work’ among health personnel working at the surgical care department; tertiary hospitals, north-west Ethiopia; 2021 (n = 388).
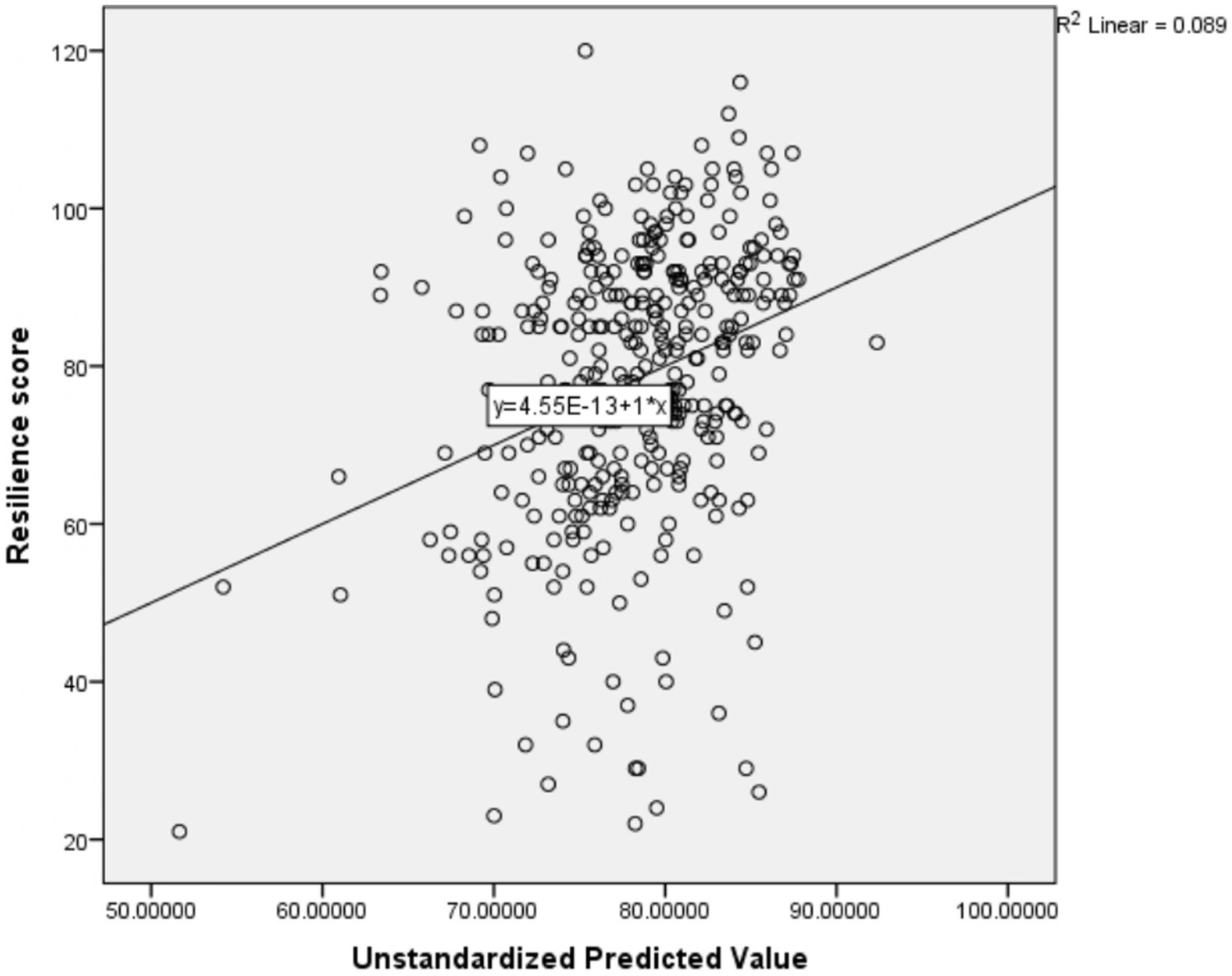
Figure 5. Scatter plot showing the amount of mean variation of resilience at work score explained by the independent variables together.
4. DiscussionIn this study, 23.2, 24.0, and 52.8% of study participants have a low, moderate, and high level of burnout in Emotional exhaustion, respectively. Regarding burnout in depersonalization, 42.5, 18.8, and 38.7% of participants have low, moderate, and high levels of burnout, respectively. Similarly, 32.2, 23.5%, and 42. % of participants have low, moderate, and high levels of burnout in personal accomplishment. Regarding resilience at work, 13.7, 36.3, and 50.0% of respondents have low, moderate, and high levels of resilience at work, respectively. Resilience at work has a positive association with PA and an inverse association with EE and depersonalization burnout sub-domains.
4.1. Level of burnoutThe study revealed that more than half of health professionals have high levels of burnout concerning the emotional exhaustion subscale. This is consistent with studies conducted in other African and/or Asian nations, such as in Mekelle Ethiopia (55.9%) (30), Iran (55.3%) (31), and Saudi Arabia (54%) (32). However, this level of emotional exhaustion is lower than the findings from the Southern part of Ethiopia (65.2%) (33), Brazil (70.6%) (34), and a pooled prevalence systemic review findings from 45 countries (68.1%) (40). The possible reason for the lower prevalence of burnout in high emotional exhaustion in the current study might be the difference in the cutoff point in high emotional exhaustion (≥ 24 for southern Ethiopia, >14 for Brazil vs. ≥27 in the current study) (33, 34). In contrast, it was higher compared to findings from Addis Ababa (42.0%) (41) and South France (15.8%) (42). The difference in perception of workload might be the plausible reason for the high prevalence of burnout in high EE in the current study as compared to Addis Ababa (high workload; 85.7% in the current study vs. 38.9% in Addis Ababa) (41). Contrarily, the distinction in EE from a study done in France may result from variations in the work environment set-up, patient volume, and working culture. In Ethiopia (43) one medical doctor and nurse are expected to serve populations of 28,847 and 2,299 respectively, whereas the equivalent figure in France is below 325 and 110 (44). Evidence showed that clinicians with high patient volume have a high rate of burnout (33, 45, 46).
In the current study, the magnitude of burnout among health professionals concerning high levels of depersonalization was 38.7%. This scope is comparable with the findings of previous studies done in Addis Ababa, Ethiopia (43.0%) (41), and Saudi Arabia (35%) (32). However, it is lower than the findings from Derdeba, Ethiopia (70.6%) (47) and South Africa (50.0%) (48). The possible reason for the lower prevalence of burnout concerning depersonalization may be derived from the relatively smaller proportion of females (26.0%) that participated in the current study compared to 44.5–55.6% of female participants that were reported in the aforementioned studies. Some evidence showed that depersonalization is more prevalent among females compared to men (49, 50). Another reason for the lower prevalence of depersonalization in the current study may be the presence of a higher number of specialists compared to the above previous studies (47). Conversely, burnout concerning depersonalization was found to be higher compared to previous studies done in Nigeria (15.8%) (51), China (7.5%) (52), and South Khorasan (16.8%) (53). Differences in a study setting might contribute to the differences; the aforementioned studies were conducted among primary healthcare professionals while the current study focused on healthcare workers employed in hospitals, characterized by relatively high workloads (54, 55).
The other dimension of burnout that was assessed in this study is personal accomplishment. According to the findings, 32.2% of the participants have high burnout levels, as displayed by low levels of personal accomplishment. This is consistent with other studies done in Romania (38%) (56), Palestine (34.6%) (57), and a systematic review of findings from low and middle-income countries (31.9%) (58). However, the percentage of high burnout in low personal accomplishment was lower than the findings from Debrebirhan (59.7%) (59), Addis Ababa (45%) (41), and among interns at other Ethiopian teaching hospitals (44.4%) (60). A possible reason for the lower prevalence reported in the current study as compared to the aforementioned studies may be the higher number of physicians who participated in the current study. Research on healthcare professionals showed that undergraduate professionals are more prone to burnout compared to post-graduate health professionals including specialists (41).
In contrast, the prevalence of low levels of personal accomplishment is higher compared to studies done in Mekelle Ethiopia (21.8%) (30), Uganda (18.33%) (61), Belgium (10.4%) (62), Germany (21.5%) (63), and Ecuador (18.2%) (64). The reason may be that compared to other studies, the current sample included a relatively higher prevalence of healthcare personnel that also hold managerial positions in addition to their professional duty (17%) compared to a much lower level in the aforementioned studies (62, 64). Literature findings present that managerial strain is positively associated with low personal performance (i.e., a high level of burnout) (65, 66). Another reason might be that the current study was conducted in high patient-load referral hospitals, which is characterized by the increased workload. A high workload was found to have a positive association with low levels of personal accomplishment (46, 67).
4.2. The factors that impact health professionals’ burnoutIn this study, midwifery health professionals were found to have a higher level of emotional exhaustion and depersonalization, and a lower level of personal accomplishment (burnout sub-scales) as compared to specialists. Moreover, anesthetic and nursing health professionals have a higher level of emotional exhaustion and depersonalization burnout, respectively, as compared to specialists. A systematic review report from Sub-Saharan Africa and Ghana is in line with the current findings (55, 68). In contrast, a study from Addis Ababa Ethiopia, which concentrated on varied types of professions, did not identify an association with any of the burnout dimensions (41).
The other demographic variable that predicted the level of burnout in the current study is the age of the participants. However, the association was found only concerning the depersonalization burnout sub-scale. According to this study, the level of depersonalization increases by 0.235 every one-year increment in participants’ age. This is in line with other studies (31, 41). Similarly, in a study done in Iran age groups of 30–39, 40–49, and ≥ 50 years had a significant correlation with the increased likelihood of burnout compared to those below 30 years of age groups (69). In contrast, a study conducted among physicians in southern Ethiopia presented that the age of the participants had an inverse relationship with both emotional exhaustion and depersonalization burnout sub-scale scores (33). However, in several other studies, the age of participants was not found to have any statistical association with the three burnout sub-scales (59, 70, 71).
Lower levels of participants’ perceptions of professional recognition were found to be positively associated with emotional exhaustion and low levels of personal accomplishment. In contrast, reducing the perception of high workloads was negatively associated with emotional exhaustion and depersonalization. Similar previous studies support these findings; studies done in Ethiopia and Malawi showed that participants who got recognition/support from hospital managers had a lower level of emotional exhaustion compared to their counterparts (33, 72, 73). The previous findings in Ethiopia in the context of workload showed that an increased workload increases the health personnel’s stress at work (74). Similarly, a study in the United Kingdom (UK) reported a high prevalence of burnout among participants with high work overload (10).
In line with a previous study conducted in Ethiopia (75), the current study revealed that reducing participants’ hope of promotion was positively associated with emotional exhaustion. In contrast to the current study, a study in Malawi presented that participants’ hope of future promotion was not significantly associated with emotional exhaustion (73).
Relationship at the workplace is another work-related variable that determines personal accomplishment. The participants’ level of burnout concerning a low personal accomplishment was increased when the participant’s perception of a relationship at the workplace decreased from very good to very bad relations. This is in line with findings from previous studies (75–77). As was found in the current study, previous findings also revealed that participants who have a fear of contracting an illness during their work have higher emotional exhaustion compared to their counterparts (75).
Among this study’s participants, seniority in work (work experience) had no statistical association with all dimensions of burnout. This was also found in previous studies (78). In contrast, a study done in Malaysia found that health professionals working under 10 years have higher levels of burnout compared to those working above 10 years (79). In divergence, other studies showed a higher prevalence of emotional exhaustion among participants who work above 10 years as compared to health professionals that work less than that (31, 53). Similarly, in a study done in Greek (80) a positive association was found between professional work experience and depersonalization and an inverse relationship with personal accomplishment.
4.3. Levels of resilience at workThe mean comparison analysis of this study affirms that the level of mean resilience at work score was higher among medical specialists as compared to nurse professionals. The multiple linear regression findings of this study also revealed that midwifery and nurse professionals have 12.26 and 6.66% lower scores of resilience at work respectively, as compared to specialists. This is in line with previous studies that also found that nurses and midwives present lower levels of resilience at work as compared to medical professionals (81, 82). This difference might be derived from the medical specialists’ having more years of education compared to nurses; an increase in education was found to improve the level of resilience at work (83).
Similar to other studies (82), being divorced and widowed is associated with a lower level of resilience at work, as compared to married health professionals. The multiple linear regression analysis also revealed that participants that are divorced or widowed have a lower mean of resilience at work as compared to their married counterparts.
In addition to the demographic variables, the working environment-related variable (perceived professional recognition) is associated with the resilience mean score. Participants in the current study who have a good perception of professional recognition were found to have a higher level of mean resilience score as compared to those who have a neutral or poor perception of professional recognition. Previous evidence showed that professional recognition and support can increase professionals’ resilience levels in their work (33, 84).
In line with findings from previous studies, resilience at work was found in the current study to have a negative association with emotional exhaustion and depersonalization, and a positive association with personal accomplishment (39, 85–88). Increased professional resilience has an impact on reducing emotional exhaustion, and increasing clinicians’ work engagement, as well as enhancing function when facing challenges at the workplace (89). Health personnel with a high level of ‘resilience at work’ have a negative association with psychological distress and burnout (90). In contrast, experiencing a high level of job-related stress and burnout is positively associated with a high-level health professional turnover and dissatisfaction (91).
4.4. The variance explained by the modelThe adjusted R-square of the four models ranged from 8.9 to 15.9% (Figures 2-5). This reflects a very small amount of the mean variation of the four outcome variables (emotional exhaustion, depersonalization, personal accomplishment, and Resilience at work) explained by the predictor variables collectively in the model. This small R-square value might be due to different reasons; The first reason might be important predictor variables like; substance use, family size, role in the family, and house ownership not included in the model that might have a higher capacity to explain the mean variation of those outcome variables. The second reason for the low R-square might also be secondary to the difficulty in explaining human behavior. In most cases, a mall R-square value is considered a sign of a bad model, but it is not always true. It depends on the type of the problem being solved; to explain materials high R-square value is recommended, but in some problems such as human behavior, the model with a small R-square value can be considered a good model (92). As a result, the current model could be a good model to predict the outcome variables with the existing low R-square.
4.5. Limitations of the studyThis study has some limitations; due to the cross-sectional nature; the study does not show the cause-effect relationships between the predictor and the outcome variables. Moreover, due to the small sample size, there is limited generalizability of the current study findings. Since the study targeted specific specialties, the selection bias cannot be excluded. More exploration of working environment-related predictor variables by using a qualitative study design might be useful to identify additional relevant factors.
5. ConclusionThis study revealed that most of the health professionals who are working in Ethiopian hospitals experience one or more forms of burnout. Around one-fourth of health professionals, face an overall burnout syndrome. In the current study, a low mean score of ‘resilience at work’ was reported. This may have a negative influence on organizational performance. This study also revealed that professional burnout and resilience at work are inversely correlated. Therefore, efforts should be invested to increase the level of resilience at work and promote professional recognition, as well as reduce high workloads in the strive of reducing burnout. Moreover, all Ethiopian hospitals should learn from this finding, and invest efforts to reduce burnout and enhance resilience at work by strengthening professional recognition, the hope of promotion, relationships at work, and reducing high workload. Further research concerning burnout and resilience at work is recommended by incorporating additional variables such as the presence of comorbidities, family-related challenges, and behavioral variables like substance use. Moreover, intervention-based studies are recommended for assessing the effect of training on the area of resilience and burnout.
Data availability statementThe raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statementThe studies involving human participants were reviewed and approved by Ethical Review Board of the Rabin Medical Center and Tel-Aviv University. The patients/participants provided their written informed consent to participate in this study.
Author contributionsYG and BA were conceived and designed for the study to conduct the analysis. YG, BA, and KH were equally involved in the interpretation and writing of the results. All authors read and approve the final manuscript.
AcknowledgmentsThe authors would like to acknowledge Rabin Medical Center and Tel-Aviv University for providing us with ethical clearance to conduct the survey. Furthermore, they would like to appreciate Bahir Dar University College of Medicine and Health Science for providing an official letter of cooperation for the study institutions. Our great thanks extend to all study subjects, data collectors, and supervisors.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
AbbreviationsEE, Emotional Exhaustion; Gyn/Obs, Gynecologic and Obstetrics; MBI-HSS, Maslach’s burnout inventory human service survey; PA, Personal Accomplishment; TGSH, Tibebe-Ghion Specialized Hospital; UoGSRH, University of Gondar comprehensive Specialized referral Hospital.
References1. Portela, GZ, Fehn, AC, Ungerer, RLS, and Poz, MRD. Human resources for health: global crisis and international cooperation. Cienc Saude Coletiva. (2017) 22:2237–46. doi: 10.1590/1413-81232017227.02702017
PubMed Abstract | CrossRef Full Text | Google Scholar
2. Witter, S, Bertone, MP, Chirwa, Y, Namakula, J, So, S, and Wurie, HR. Evolution of policies on human resources for health: opportunities and constraints in four post-conflict and post-crisis settings. Confl Heal. (2016) 10:1–18. doi: 10.1186/s13031-016-0099-0
CrossRef Full Text | Google Scholar
3. World Health Organization. Global strategy on human resources for health: workforce 2030. Geneva: World Health Organization (2016).
4. Jackson, J, Vandall-Walker, V, Vanderspank-Wright, B, Wishart, P, and Moore, SL. Burnout and resilience in critical care nurses: a grounded theory of managing exposure. Intens Crit Care Nurs. (2018) 48:28–35. doi: 10.1016/j.iccn.2018.07.002
PubMed Abstract | CrossRef Full Text | Google Scholar
5. Olson, K, Kemper, KJ, and Mahan, JD. What factors promote resilience and protect against burnout in first-year pediatric and medicine-pediatric residents? J Evid Based Complement Altern Med. (2015) 20:192–8. doi: 10.1177/2156587214568894
PubMed Abstract | CrossRef Full Text | Google Scholar
6. Bianchi, R, Schonfeld, IS, and Laurent, E. Is it time to consider the “burnout syndrome” a distinct illness? Front Public Health. (2015) 3:158. doi: 10.3389/fpubh.2015.00158
CrossRef Full Text | Google Scholar
7. Maslach, C, and Leiter, MP. Understanding the burnout experience: recent research and its implications for psychiatry. World Psychiatry. (2016) 15:103–11. doi: 10.1002/wps.20311
CrossRef Full Text | Google Scholar
8. Martínez-López, JÁ, Lázaro-Pérez, C, and Gómez-Galán, J. Predictors of burnout in social workers: the COVID-19 pandemic as a scenario for analysis. Int J Environ Res Public Health. (2021) 18:5416. doi: 10.3390/ijerph18105416
PubMed Abstract | CrossRef Full Text | Google Scholar
9. Habadi, AI, Alfaer, SS, Shilli, RH, Habadi, MI, Suliman, SM, Al-Aslany, SJ, et al. The prevalence of burnout syndrome among nursing staff working at king Abdulaziz university hospital, Jeddah, Saudi Arabia, 2017. Divers Equal Health Care. (2018) 15:122. doi: 10.21767/2049-5471.1000165
CrossRef Full Text | Google Scholar
10. Imo, UO. Burnout and psychiatric morbidity among doctors in the UK: a systematic literature review of prevalence and associated factors. BJPsych Bull. (2017) 41:197–204. doi: 10.1192/pb.bp.116.054247
留言 (0)