
記住我
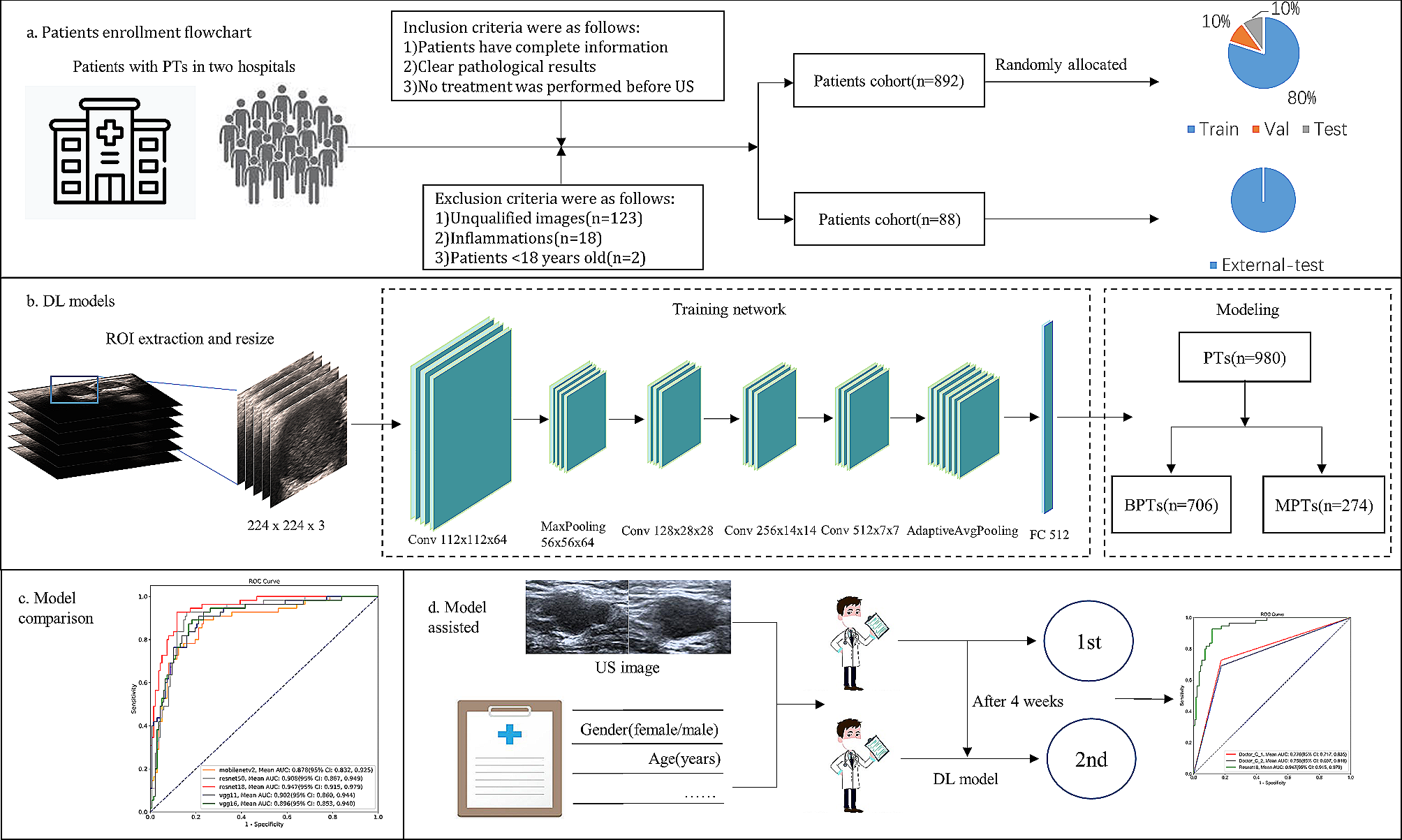

The present study will be an open-label, single-arm, single-center prospective phase-II trial to establish the total neoadjuvant chemotherapy protocol. Preoperative CRT, followed by three cycles of mFOLFOX-6 chemotherapy or two cycles of CAPOX chemotherapy will be performed prior to TME (open, laparoscopic, or robotic). Nine cycles of mFOLFOX-6 chemotherapy or six cycles of CAPOX chemotherapy will then be administered postoperatively to patients with resectable locally advanced rectal adenocarcinoma at a high risk of distant metastasis, including the pretreatment status of a suspected T4b tumor, lateral pelvic lymph node metastasis, or extramural venous invasion. The treatment algorithm is shown in Fig. 1. Pretreatment CT and MRI will be used to diagnose all patients. The study protocol has been approved by the Ethics Committee of the University of Tokyo Hospital and the University of Tokyo Clinical Research Ethical Committee (approval No.: 2021508SP) and is registered in the Japan Registry of Clinical Trials (jRCT, approval No.: jRCTs031210660). This study was opened in March 2022. In modification protocol, including explanatory documents and consent forms, and various procedure manuals are to be changed, the principal investigator must consult with the University of Tokyo clinical research review committee prior to the change. After receiving the board’s review and approval, the change’s details will be reported to the hospital director. Then, submit a notification of changes to the implementation plan to the Minister of Health, Labor and Welfare by registering with jRCT.
Fig. 1
Flow diagram of the trial
Sample sizeThe target sample size was set as 30 patients based on the confidence interval (CI) width. According to a previous clinical trial [9], we estimated the incidence of adverse events (AE) to be 40% in the present study protocol. The two-sided 95% CI ranged between 22.7 and 59.4% with the enrollment of 30 patients. A previous study showed that the incidence of AEs in the historical control was approximately 30% [13]; therefore, 30 patients fulfilled the desired precision because the incidence of AEs in the estimated upper 95% CI is not more than twice that in the control group.
Study objectivesThe primary outcome will be the incidence of AEs during total neoadjuvant therapy at the end of adjuvant FOLFOX or CAPOX therapy. AEs will be evaluated according to the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. Secondary objectives will be the evaluation of long-term outcomes, including distant relapse-free survival at 3 years, relapse-free survival at 3 years, the local recurrence rate at 3 years, and overall survival. Furthermore, pCR rates; postoperative morbidity and mortality rates; the dose intensity for each regimen, including CRT, neoadjuvant chemotherapy (NAC), and adjuvant therapy; and compliance with the study protocol, defined as completing full-dose treatment in each regimen, will be secondary endpoints.
Patient selectionThirty patients with locally advanced rectal adenocarcinoma will be enrolled. Patients will be 20–80 years old and meet inclusion and exclusion criteria (Table 1).
Table 1 Inclusion and exclusion criteria Data collection, monitoring, and auditingTable 2 shows the schedule for the assessment. The principal investigator and sub-study investigator will monitor and assess the clinical course, safety, and efficacy outcomes recorded in medical records and complete the case report form (CRF). All CRF will be submitted to a separate department for data management, which will be appointed by the principal investigator, in the University of Tokyo. The monitor will perform verification based on “Written procedure for the study monitoring” during the study. Among CRFs, severe cases will be reported to the Ethical Committee within 30 days. No auditing is planned as part of this exploratory study.
Table 2 Assessment schedule summary Data analysisPatient baseline characteristics will be used to calculate summary statistics and distributions. The frequency and proportions of the categories for nominal variables are displayed for each group. Summary statistics (the number of cases, mean, standard deviation, minimum, median, and maximum) for continuous variables will be calculated for each group. The primary outcome analysis as an interval estimation of the incidence of AEs (CTCAE ≥ grade 3) is performed using an accurate CI based on the binomial distribution. The incidence of severe adverse events (AEs), the primary endpoint, might be higher in the TNT group than in patients who received preoperative chemoradiation with UFT/UZEL plus CPT-11 at our department (historical control group). If necessary, the ratio of severe AEs will be compared using Fisher’s exact calculus test.
Treatment planPatients who meet the eligibility criteria will be informed of all details about the study procedure. They will receive CRT, mFOLFOX-6, or CAPOX; undergo radical surgery at approximately week 21; and receive another course of mFOLFOX-6 or CAPOX (Fig. 1). Only patients who voluntarily participate in the study and provide informed consent will be enrolled.
Preoperative CRTCRT will be performed as previously described [13]. Briefly, CRT consists of long-course radiation (50.4 Gy/28 fractions, five days per week) on days 1–38, concurrent with oral and intravenous chemotherapy (TEGAFIRI; tegafur/uracil, oral leucovorin, irinotecan). During RT, UFT (300 mg/m2/day for less than 1.17 m [2], 400 mg/m2/day from 1.17 to 1.49 m [2], 500 mg/m2/day from 1.50 to 1.83 m [2], and 600 mg/m2/day for more than 1.83 m [2]) and LV 75 (mg/day) will be orally administered on the days of RT, while irinotecan (80 mg/m2) will be intravenously administered on days 1, 15, 29, and 43.
A physical examination, laboratory test, and AE assessment will be performed at every irinotecan injection. AEs that occur during or after the cycle administration will be collected.
Neoadjuvant systemic chemotherapyFour to eight weeks after the completion of RT, patients will receive NAC, including three cycles of mFOLFOX-6 or two cycles of CAPOX. The mFOLFOX-6 regimen consists of the following: oxaliplatin 85 mg/m2 intravenously administered and 5-FU 400 mg/m2 administered as an intravenous bolus on day 1, followed by 2400 mg/m2 intravenously administered over 24 h on days 1–2, and leucovorin 200 mg/m2 intravenously administered on day 1. One cycle of mFOLFOX-6 is 14 days. The CAPOX regimen consists of the following: oxaliplatin 130 mg/m2 intravenously administered on day 1 and capecitabine 2000 mg/m2 orally administered twice a day on days 1–14 in every cycle. One cycle of CAPOX is 21 days. A physical examination, laboratory test, and AE assessment will be performed at the time of every oxaliplatin injection. AEs that occur during or after the cycle administration will be collected.
Rectal resectionRadical surgery will be performed 4 to 8 weeks after the completion of NAC. Lateral lymph node dissection will be selectively performed on patients with suspected lateral lymph node metastasis before CRT. All resected specimens will be pathologically analyzed according to the American Joint Committee on Cancer classification [14]. The pathological therapeutic response of the primary tumors will be assessed according to the Japanese Classification of Colorectal, Appendiceal, and Anal Carcinoma of the Japanese Society for Cancer of the Colon and Rectum [15]. The frequency and grade of surgical complications within 30 days of surgery will be evaluated using the Clavien-Dindo classification.
Adjuvant systemic chemotherapyPatients will receive adjuvant chemotherapy within 12 weeks of surgery, including nine cycles of mFOLFOX-6 or six cycles of CAPOX. AEs that occur during or after each cycle administration will be collected. A physical examination, laboratory test, and AE assessment will be performed at the time of every oxaliplatin injection. If patients cannot start to receive adjuvant chemotherapy or if adjuvant chemotherapy is discontinued prematurely, the follow-up period will be started in these patients.
Chemotherapy administration criteria and dose reduction criteriaChemotherapy administration criteria are shown in Supplementary Table 1. The criteria consist of number of hematologic toxicities, including white blood cells, neutrophil, platelets, and non-hematologic toxicities, including nausea and hand-foot syndrome. Chemotherapy is interrupted until the criteria are met. The dose reduction criteria and the reduced doses are shown in Supplementary Tables 2 and Supplementary Tables 3, respectively. Each chemotherapeutic drugs should be reduced when hematologic and non-hematologic toxicity ≥ Grade 3 is observed. In addition, doses can be reduced at the physician’s discretion to ensure safety.
Rescue and prohibited concomitant medicationConcomitant use of aprepitant, fosaprepitant meglumine, and granisetron prevent adverse events during systemic chemotherapy. Palonosetron, steroid, and d-chlorpheniramine maleate could be combined with the oxaliplatin regimen (Day 1). Palonosetron and steroids could be used concomitantly during the administration of CPT-11 (Day 1). In addition, supportive care drugs for the several symptoms caused by chemotherapy are allowed to use under the consideration of investigators.
Hormonal therapy other than steroids and concomitant therapy such as immunotherapy is prohibited. Drugs or treatments with anti-tumor effects not listed in the protocol are also prohibited.
Adherence assessmentsMultiple occupations, including investigators and pharmacists, will assess medication adherence at every follow-up visit or admission during pre- and postoperative chemoradiation and chemotherapy to enhance data validity. These data are recorded on the appropriate case report form.
Follow-upPostoperative surveillance is performed according to the Japanese Society for Cancer of the Colon and Rectum guidelines [16]. In this surveillance, patients will receive a physical examination, blood examination, including a complete blood count, routine chemistry, including liver and kidney function tests, and the measurement of carcinoembryonic antigen levels in serum every three months. In addition, an assessment by CT (every six months) and colonoscopy (every year) will be performed.
Safety evaluation and reporting of adverse eventsThe principal and sub-study investigators will monitor and assess the clinical course, safety, and efficacy outcomes recorded in medical records. All adverse events during pre- and postoperative treatment and postoperative complications 30 days after surgery need to be reported in the case report form (CRF). Among CRFs, severe cases will be reported to the Ethical Committee within 30 days. Then investigators will review all events and reactions. The National health system covers indemnity for negligent harm in patients enrolled in the study. After completion or discontinuation of this clinical study, the participants will be performed necessary examinations and observations to ensure their safety.
留言 (0)