
記住我








We considered our case a “paradoxical IRIS” because we observed a worsening of symptoms and the appearance of new lesions. At the first presentation, the worsening of symptoms with the involvement of the contralateral eye was related to the misdiagnosis. The second time the patient was on specific therapy with IV penicillin instead. The condition resolved without the necessity of steroids or other anti-inflammatory drugs.
The definition of IRIS-syphilis is complex as it is not always possible to discern it from a recent infection or a worsening of an undiagnosed one. Syphilis syndromes have rarely been described in the context of immune reconstitution, and only a few cases have been reported in the literature [3]. A computerized search was performed without language restriction using PubMed, SCOPUS and Web of Science™ for all cases of IRIS-syphilis from database inception until April 2022.
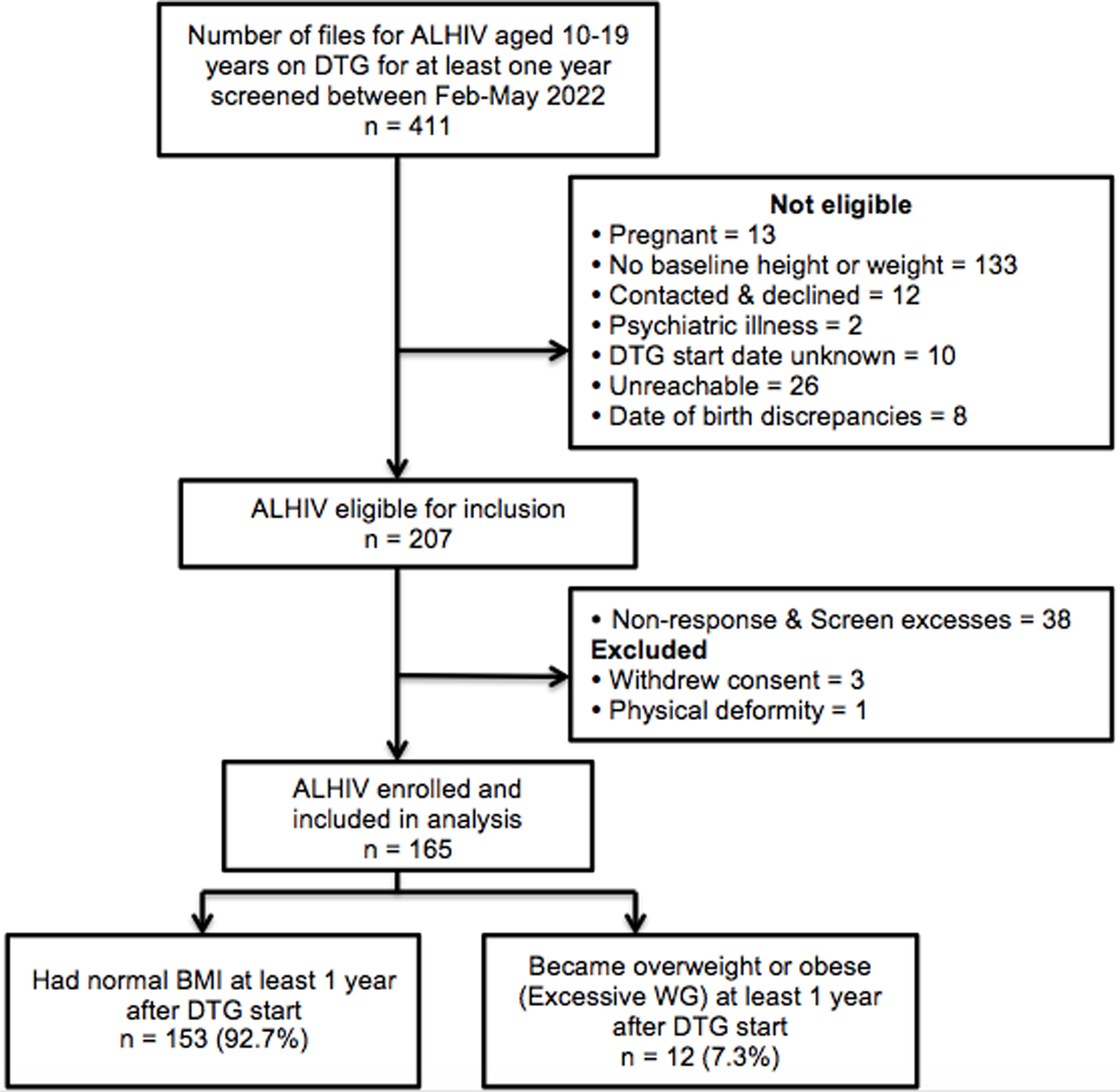
Our review using PubMed, SCOPUS and Web of Science™ (Figure 1) showed only 14 cases of IRIS associated with syphilis described in the literature. The cases were divided into "unmasking syphilis", characterized by a new appearance of syphilis symptoms after ART initiation, and "paradoxical syphilis", characterized by worsening previously present symptoms.
Fig.1
Research of literature: identification of cases, screening, and inclusion
Epidemiological data and HIV status information are analytically shown in Table 1. Clinical characteristics of all the patients retrieved are analytically illustrated in Table 2, and investigations during IRIS, therapy and outcome are shown in Table 3. All patients were male with a 43-year-old median age (IQR 36 to 46). Of these cases, seven were concerned with HIV naïve to therapy patients and 7 with HIV infection known for years with poor compliance to ART. The HIV viral load at baseline was reported in 12 cases with a median value of 177,828 copies/ml (IQR 71,000 to 280,000 copies/ml), and CD4+ T lymphocytes count was reported in 14 cases prevalently lower than 200, with a median value of 91 cells/μl (interquartile range 25.5 to 163.5 cells/μl). The IRIS manifestations were associated with a reduction of HIV viral load by approximately three logarithms and to increase in CD4+ cell count.
Table 1 Epidemiological data and pre-IRIS dataTable 2 Type of IRIS and clinical manifestationTable 3 Investigations during IRIS, therapy, and outcomeWe classified 10 cases as “unmasking syphilis” and four as “paradoxical syphilis”. The median time for the development of IRIS after the beginning of ART was 28 days (IQR 13 to 46.5 days).
Skin and ocular manifestations were the most frequently described; all cases were compatible with secondary syphilis, and there were genital lesions in three.
A diagnosis of neurosyphilis/ocular syphilis was posed in 8 cases: six were characterized by ocular involvement and two by a neurological deficit. Ocular manifestations are diversified, and any component of the eye can be involved. The mostly disorders described were the reduction of visual acuity, scotomas, blurred vision, floaters, conjunctival injection, tearing, and eye pain. Neurological involvement was only in two cases with motor, language, and memory deficits appearance [5, 6]. Skin manifestations were heterogeneous and sometimes atypical. Braue et al describe a case of malignant syphilis characterized by necrotic warty lesions with a tumoral appearance whose histology initially set cutaneous lymphoma in the differential diagnosis [4]. Skin manifestations were associated with ocular involvement in four cases. The frequent ocular manifestation in these patients can be justified by immunocompromising that promotes the rapid spread of the pathogen. Lumbar puncture was performed in most cases, and CSF alterations were in a few, predominantly pleocytosis. Negative syphilis serology and or polymerase chain reaction usually was observed like in our case. Nevertheless, the absence of CSF alterations should never exclude neurosyphilis when clinical manifestations are suggestive. In all cases, the patients were not on ART either because they were naïve or because of inadequate adherence to therapy. We didn’t observe a particular ART regimen associated with IRIS syphilis, but most therapies were INSTI or protease-inhibitor based. ART induces restoration of a cellular immune response against Treponema pallidum antigens and may probably result in the progression toward exuberant clinical features of the disease [2]. In almost all cases, basal serology for syphilis was negative and became positive after IRIS manifestation. It can happen in an HIV-positive patient with less than 200 CD4+T cells because a humoral response does not develop or could be suppressed due to the dysfunction of CD4+T-cells [7]. It is plausible that the restoration of immune responses as a result of effective HIV-1 treatment triggers the unmasking of subclinical Treponema pallidum infection and subsequent seroconversion. On the other hand, a negative syphilis serology could be caused by the prozone phenomenon or the hook effect, in which an overabundance of an antigen led to a false-negative result [3, 8,9,10]. Treatment for IRIS syphilis does not differ from standard syphilis therapy, and steroid therapy would seem unnecessary. Systemic steroid use has been reported for a short period in a few cases.
In conclusion, our case and the others reported in the literature suggest that IRIS associated with syphilis should be considered when an unusual rash or ophthalmologic compromise appears after the ART initiation. A negative syphilis serology before beginning antiretroviral therapy could convey the impression that syphilis has been ruled out; a high index of suspicion should be maintained instead when symptoms suggestive of syphilis are noticed after treatment has begun.
留言 (0)