
記住我
Cholera is an acute, watery diarrheal disease caused by Vibrio cholerae, a curved, rod-shaped, motile, Gram-negative bacterium that lives in aquatic environments. Without prompt treatment, cholera can cause severe dehydration and death. Treatment involves administering saline oral rehydration solutions, intravenous fluids, or antibiotics, depending on the severity (1–3). V. cholerae is spread from person to person via the fecal-oral route or indirectly through contaminated food and water (3). Cholera is endemic in many regions of Africa and Asia, where seasonal or sporadic outbreaks occur (4–7), predominantly in countries with poor sanitary conditions, such as open defecation, unhygienic food handling, and limited access to safe drinking water (8).
Vibrio cholerae is of major public health concern due to its potential to cause pandemics. Since 1817, there have been seven cholera pandemics, with the seventh beginning in 1961 and continuing until today. In 2015, the estimated annual incidence of cholera was 1.3–4 million cases, resulting in 21,000–143,000 deaths (9). However, the notification of cholera cases to the WHO is not mandatory; therefore, it is an underreported disease in many countries (9). For several reasons, the true burden of cholera is underestimated. For instance, it is often difficult to differentiate cholera from other acute diarrheal diseases based on clinical observation. Additionally, diagnostic and epidemiological surveillance laboratories may be deficient or even absent in cholera-endemic areas, thereby limiting accurate etiological diagnosis. It is likely that many cholera-associated cases and deaths do not present to health facilities and are therefore not included in the reports. Added to this, in some countries, there might be disincentives to report cases due to the possible negative impact on tourism and the export industry (10). Recently, the SARS-CoV-2 pandemic has affected cholera surveillance in many regions (11, 12), and there were 65% fewer cases reported to the WHO in 2020 than in 2019 (13). At the same time, preventive measures implemented during the pandemic, such as handwashing, hygiene promotion, social distancing, and banning of large gatherings, likely reduced cholera transmission. The extent to which the SARS-CoV-2 pandemic affected cholera surveillance and epidemiology is currently unknown (14, 15). Thus, cholera remains a leading cause of morbidity and mortality in several developing and resource-poor countries (14).
Cholera is a preventable and treatable disease, and several strategies can be used to control it (Box 1). In 2017, the Global Task Force for Cholera Control proposed an ambitious plan to eliminate endemic cholera in 20 countries and reduce cholera deaths by 90% by 2030 (22). The plan, called “Ending Cholera: A Global Roadmap to 2030,” focuses on strengthening public health systems, improving surveillance for early detection of cholera outbreaks, improving drinking water, sanitation, and hygiene conditions, making oral rehydration treatments more accessible, and increasing vaccination coverage.
BOX 1 Cholera prevention and control strategies.
• Improved sanitation and access to drinking water: This disease is primarily spread through the consumption of contaminated water or food. Therefore, improving access to drinking water and sanitation facilities can contribute to reducing the risk of cholera transmission (16).
• Early detection and prompt treatment: Rapid detection of cholera cases and adequate treatment can reduce the spread of the disease and decrease the number of deaths. Rapid diagnostic tests are useful in this regard (17).
• Vaccination: Oral cholera vaccines (OCVs) have been shown to be effective in preventing cholera and should be used as part of a comprehensive cholera control strategy, especially in endemic areas or during outbreaks (18).
• Health education: Education campaigns can help to raise awareness about cholera and how to prevent it. These campaigns should include information on proper food storage and preparation, hand washing, and recognizing the signs and symptoms of cholera (19).
• Strengthening health systems: A strong health system is crucial for effective prevention, detection, and response to cholera. This requires trained health workers, laboratory capacity, and adequate supplies of vaccines, antibiotics, and oral rehydration solutions (20).
• Antimicrobial resistance (AMR) surveillance: Severe cholera is treated with antibiotics, but the emergence of antibiotic-resistant strains can make treatment more difficult. AMR surveillance is essential to ensure appropriate antibiotic use and prevent the spread of resistant strains (21).
• International cooperation: Cholera is a global health problem and requires a coordinated global effort. The WHO, along with non-governmental organizations (NGOs) and other international organizations, plays a key role in coordinating efforts to control cholera.
While these strategies can help to control the burden of cholera and prevent large outbreaks, it is important to note that V. cholerae will likely never be completely eradicated, as this bacterium is ubiquitous in aquatic environments.
Antibiotic prophylaxis can theoretically prevent both human-to-human and environment-to-human cholera transmissions. Also, some field trials have suggested that chemoprophylaxis has a protective effect among household contacts of people with cholera (23, 24). However, due to the risk of resistance selection, antibiotic prophylaxis for close contacts, as well as for travelers arriving in or departing from cholera-affected areas, is not usually recommended (25).
Efforts and research directed toward the development of cholera vaccines date back more than a century. The first cholera vaccine, a live whole-cell injectable formulation, was developed in 1885 (26). A few years later, killed and attenuated cholera vaccines were reported in 1888 and 1892, respectively (27). Other injectables cholera vaccines were developed throughout the first half of the 20th century. However, all these vaccines had low levels of protective efficacy (PE) and a concerning history of adverse effects (28).
The start of the seventh cholera pandemic in the 1960s and the spread of this disease throughout Asia and Africa led to increased international interest and funding for cholera research, resulting in the development of the first oral cholera vaccine (OCV). It should be noted that current OCVs exhibit variable PE in human populations for several reasons, including the presence of different V. cholerae strains in endemic areas, immunization coverage, malnutrition, co-infections, and variations in the gut microbiome (29, 30). Thus, a cholera vaccine that provides broad and long-lasting protection remains elusive.
In this review, we will discuss recent advances in understanding the V. cholerae pathogenesis and immunity against cholera, as well as the current status of approved cholera vaccines. Lastly, we discuss how all this knowledge gained could lead to the development of next-generation cholera vaccines.
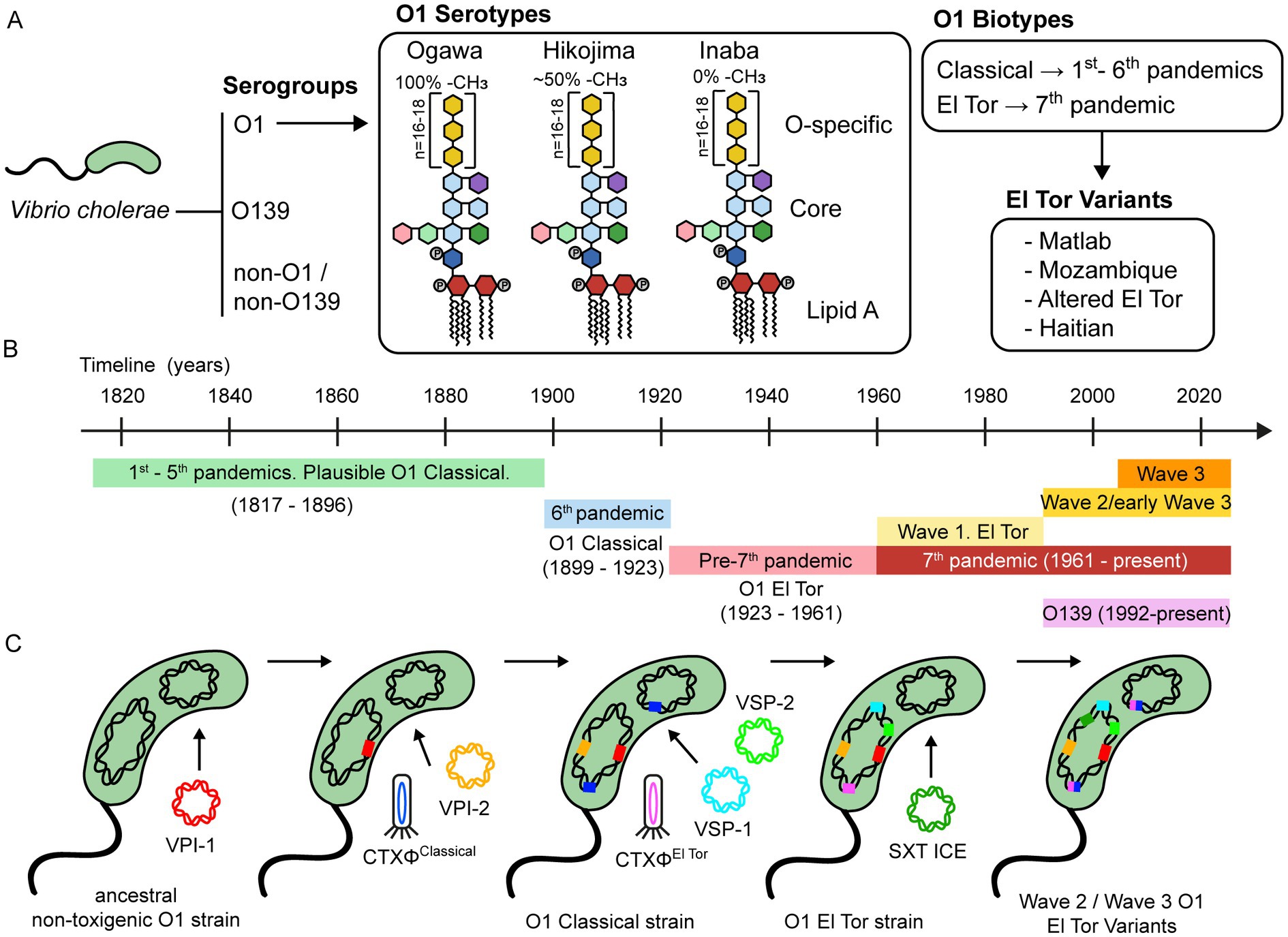
2. Vibrio cholerae classificationVibrio cholerae is divided into more than 200 serogroups determined by the structure of the O-antigen of lipopolysaccharide (LPS) (Figure 1A). Among them, a subset of strains belonging to serogroups O1 and O139 can cause cholera and epidemics due to their ability to produce cholera toxin (CTX). Serogroups that are not O1 and O139, collectively referred to as non-O1/non-O139, typically lack the CTX and cause small gastroenteritis outbreaks, sporadic cases of bacteremia, and wound infections, but they do not cause cholera (31–33). Unlike O1, more than 85% of non-O1 serogroups (including O139) have a capsule that is critical for virulence in extraintestinal infections (34).
Figure 1. Classification and evolution of V. cholerae. (A) V. cholerae is classified into serogroups based on the composition of the O antigen of LPS. Strains belonging to the O1 serogroup are further divided into three serotypes, namely Ogawa, Hikojima, and Inaba. The LPS of these three serotypes is schematically represented, showing the approximate percentage of methylation of the terminal perosamine. Serogroup O1 is also classified into the Classical and El Tor biotypes, based on phenotypic and genetic markers. Over the past two decades, there has been a growing number of reports on V. cholerae strains that possess genetic features from both the Classical and El Tor biotypes, leading to the emergence of hybrid or variant strains. These strains have been linked to several cholera outbreaks worldwide and have contributed significantly to the global burden of this disease. (B) Timeline of the history of cholera pandemics. (C) A schematic representation of the evolutionary process underlying the development of virulence in serogroup O1. This process is mainly driven by the acquisition of mobile genetic elements, including bacteriophages, genomic islands, integrative and conjugative elements, among others.
Furthermore, O1 strains are divided into three serotypes, designated Ogawa, Inaba, and Hikojima, which are grouped according to the methylation status of the terminal perosamine of the LPS. Ogawa strains are methylated, Inaba strains are unmethylated, and Hikojima strains express both methylated and unmethylated O-antigens. While the Ogawa and Inaba serotypes can co-circulate during epidemics and are capable of interconverting (35), the Hikojima serotype is rare, and evidence indicates that it is an unstable transitional form that results when a strain undergoes serotype switching from Ogawa to Inaba (36).
Biotype is another key classifier of V. cholerae O1 strains. Classical and El Tor biotypes can be distinguished according to a set of phenotypic and genetic markers (37, 38). Interestingly, there are some differences in the infection patterns between both biotypes. El Tor strains are more efficient at host-to-host transmission, survive better in the environment and the human gut, and have a higher occurrence of asymptomatic than symptomatic carriers, compared to the Classical strains (39).
3. Cholera epidemics and pandemicsIt seems that the first five cholera pandemics were caused by Classical biotype strains (1817–1896) (Figure 1B) (40). After this, the sixth cholera pandemic (1899–1923) was caused by the Classical biotype. The Classical biotype was prevalent until the 1960s, but during the pre-seventh-pandemic period (1923–1961), some sporadic outbreaks associated with the El Tor biotype were reported. The ongoing seventh pandemic (1961 to date) is caused by the El Tor biotype (41). Notably, after the emergence of the El Tor biotype, the Classical biotype declined and disappeared by the 1980s, and it is now considered extinct (42).
Eight distinct phylogenetic lineages have been identified based on whole-genome sequencing and genomic analyses of different pandemic strains. The L1 and L3-L6 lineages include Classical strains from the first six pandemics. The L2 lineage includes the El Tor strains of the seventh pandemic (7PET) and is subdivided into three clades (waves 1–3) that represent independent waves of transmission (43). Subsequent analysis reported subclades within individual waves and several transmission events, namely, T1-T12 from African countries, LAT-1 to LAT-3 from Latin America, and T13 from East Africa and Yemen (43–45).
Wave 1 strains were prevalent between 1961 and the early 1990s. During the 1990s, serogroup O139 emerged and caused cholera epidemics in Southeast Asia, but its incidence declined a few years later, and it is now rarely isolated. At the same time, Wave 2 and early Wave 3 strains emerged and replaced Wave 1 strains. Interestingly, many Wave 2 and Wave 3 strains display a mix of phenotypic and genotypic traits of Classical and El Tor biotypes, suggesting that they are genetic hybrids (37). These hybrid strains include the Matlab variants from Bangladesh, the Mozambique variants, the Haitian variants, and the altered El Tor biotype from various parts of the world (46). While Wave 2 strains have waned since the 2000s, Wave 3 strains are now the dominant cause of cholera globally (47).
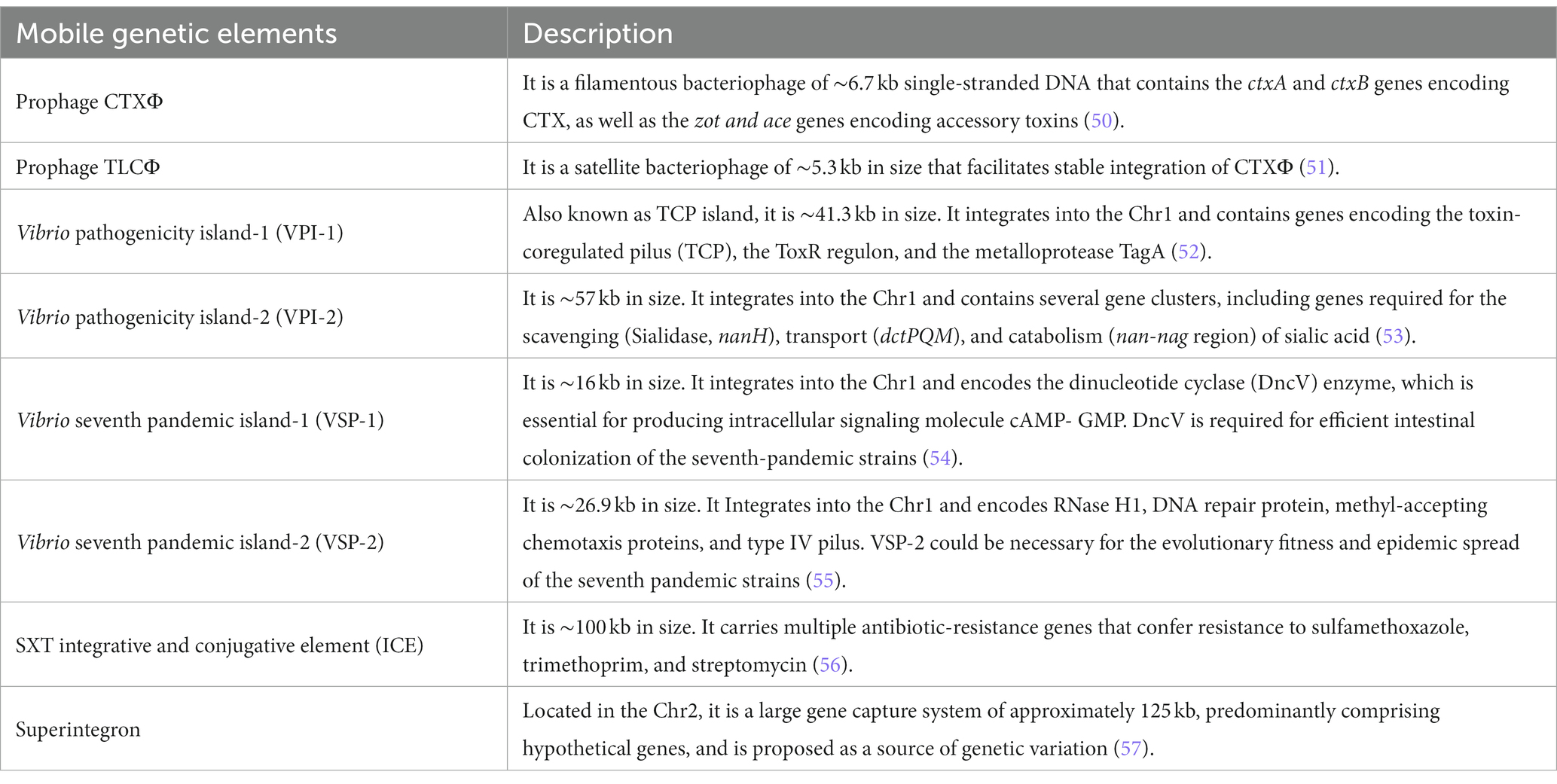
4. Genome and evolution of virulence of Vibrio choleraeThe genus Vibrio commonly harbors two nonhomologous circular chromosomes, Chr1 and Chr2 (48). The first complete genome sequence of a V. cholerae strain was announced for the clinical isolate O1 El Tor Inaba N16961 (49). Genomic analysis of this strain revealed that Chr1 has 2.96 Mb with a 47.7% G + C content, while Chr2 has 1.07 Mb with a 46.9% G + C content. Chr1 contains a large number of genes for essential cellular functions, such as DNA replication, transcription, translation, and cell-wall biosynthesis, as well as virulence genes encoding toxins, adhesins, and surface antigens. By contrast, the Chr2 has fewer such genes and contains a very large integron comprising genes with diverse functions. Comprehensive analysis of both chromosomes revealed the presence of a suite of mobile genetic elements (MGEs), including prophages, genomic islands (GIs), and integrative and conjugative elements (ICEs) (49). Table 1 describes a select list of MGEs that are important in pandemic V. cholerae strains.
Table 1. Main mobile genetic elements harbored by pandemic V. cholerae strains.
The genomic plasticity of V. cholerae and its ability to exchange genes through natural transformation, conjugation, and transduction are hallmarks of this bacterium. Its evolution is continuous due to the acquisition or loss of genomic segments (58, 59). The acquisition of MGEs is known to be the major driver for the evolution of V. cholerae virulence and a determinant of genetic divergence between environmental and pandemic strains (60, 61). In this respect, understanding the evolutionary events that lead to the emergence of pandemic clones of V. cholerae might provide new approaches for controlling this pathogen.
Chun et al. (62) proposed a hypothetical evolutionary pathway for the emergence of the seventh pandemic V. cholerae strains (Figure 1C). According to this model, the diversification of a common ancestral strain occurred through the sequential acquisition of MGEs, likely driven by environmental factors. After acquiring the O1 antigen, an O1 progenitor strain probably acquired the Vibrio pathogenicity island-1 (VPI-1) and Vibrio pathogenicity island-2 (VPI-2), which are ubiquitous among strains from the sixth (Classical biotype) and seventh (El Tor biotype) pandemics (63). VPI-1 encodes the toxin-coregulated pilus (TCP), which is the receptor for bacteriophage CTXΦ. Thus, transduction by the CTXΦ must have been preceded by the acquisition of VPI-1. The divergence between the Classical and El Tor biotypes was due to the acquisition of distinct bacteriophages CTXΦ and the Vibrio seventh pandemic islands (VSP-1 and VSP-2). Several lines of evidence support this. For example, comparative nucleotide sequence analyses have revealed that the CTXΦ from Classical and El Tor biotypes comprise two distinct lineages, indicating that they were acquired in independent events (64–66). In addition, VSP-1 and VSP-2 are consistently found in the O1 El Tor and O139 strains but are predominantly absent in the O1 Classical strains isolated between 1817 and 1923 (40, 59).
Horizontal gene transfer events have also occurred among strains from the seventh pandemic. Unlike Wave 1 strains, Wave 2 and Wave 3 strains contain a self-transmissible integrative conjugative element that carries multiple antibiotic-resistance genes (SXT ICE). The acquisition of SXT ICE likely influenced the population shift from the Wave 1 to Wave 2/3 strains (43). Interestingly, O139 strains that emerged in the 1990s also harbor the SXT ICE (56). In addition, Wave 2 and Wave 3 strains have undergone multiple CTXΦ substitutions and replacements, leading to the emergence of El Tor variant strains (47, 67).
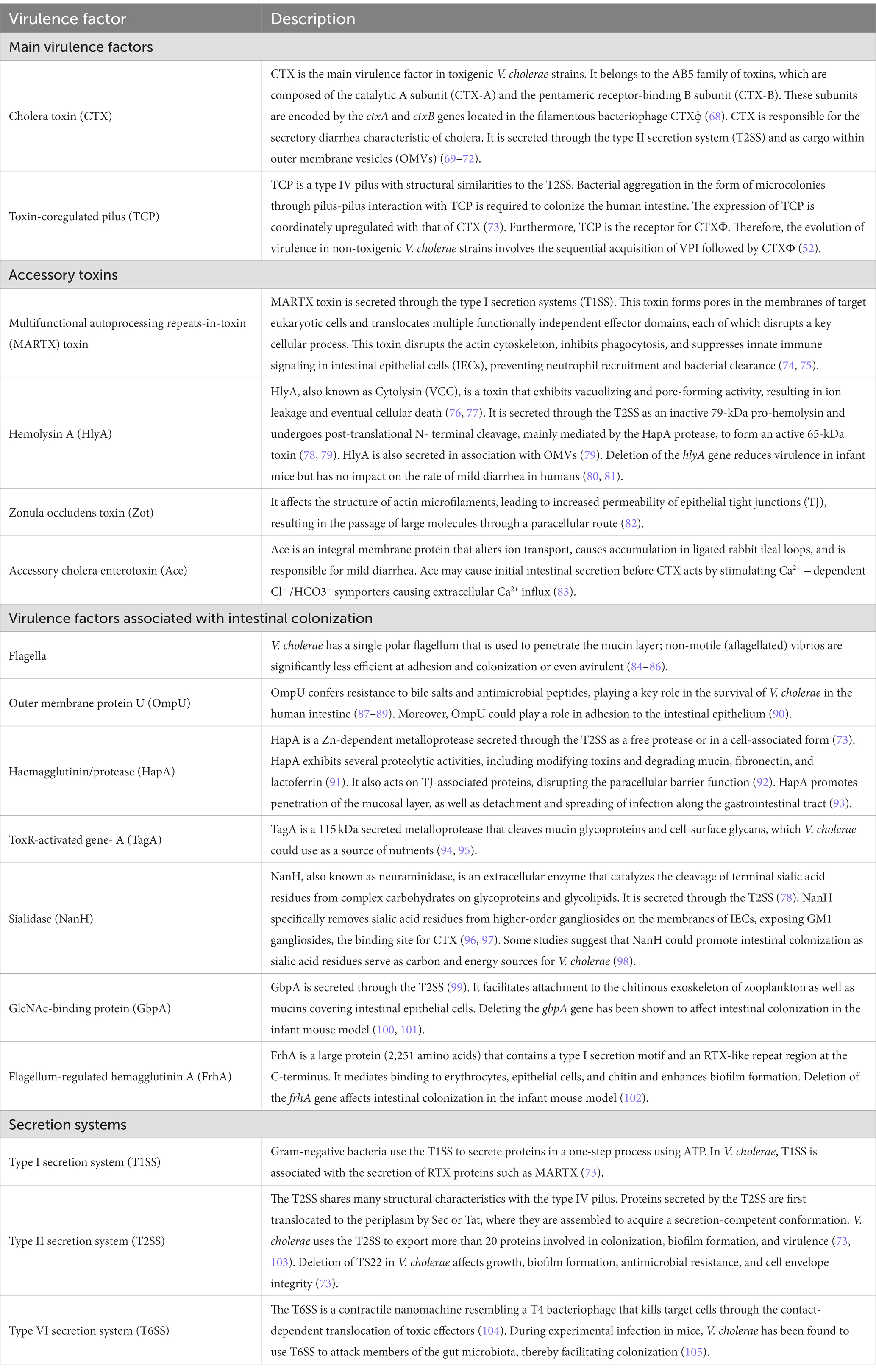
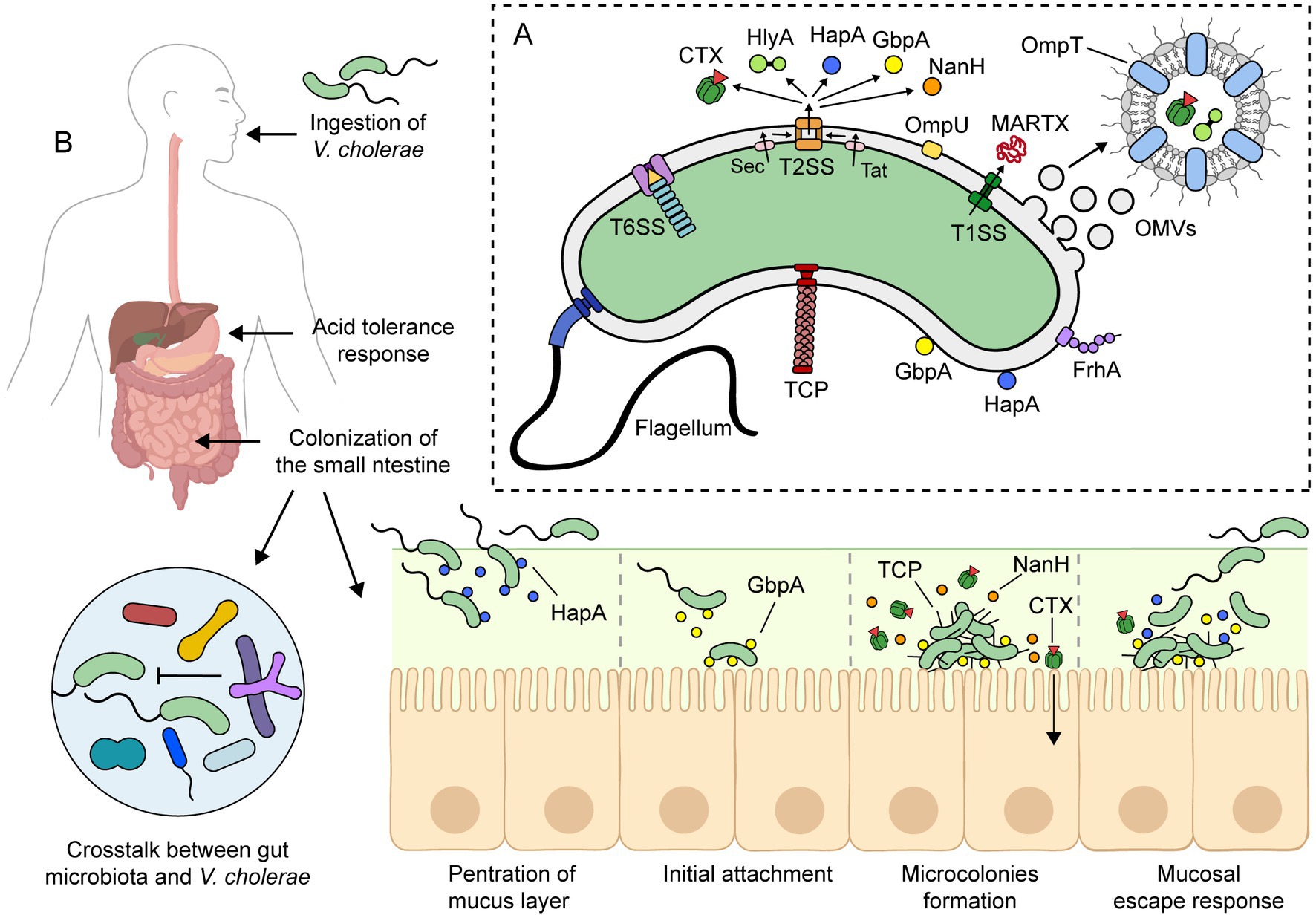
5. Pathogenesis of Vibrio choleraeIn this section, we will review the current understanding of the pathogenesis of toxigenic V. cholerae strains, particularly the O1 serogroup. Much of this information has been obtained from in vitro assays and challenge experiments in animal models, although some findings have been subsequently confirmed in human infections. Table 2 provides a summary of the main virulence factors of V. cholerae that are expressed during infection, and Figure 2A depicts some of these virulence factors.
Table 2. Selected virulence factors of V. cholerae expressed during human infection.
Figure 2. Pathogenesis of toxigenic V. cholerae. (A) Toxigenic V. cholerae produces several virulence factors that contribute to its pathogenesis. The precise pathogenic mechanism is not yet fully understood, but it is widely accepted that it involves the combination of these virulence factors and the ability to colonize and persist in the small intestine. (B) Upon ingestion, V. cholerae survives the low pH of the stomach via an acid tolerance response. In the small intestine, V. cholerae uses its flagellum to propel through the mucus layer and reach the epithelial surface. Meanwhile, V. cholerae must overcome host immunity and the colonization resistance mechanisms of the gut microbiota. To colonize the small intestine, it expresses virulence factors such as toxin-coregulated pilus (TCP) and cholera toxin (CTX). During infection, other factors such as HapA, GbpA, and NanH are also expressed. For more details on the roles of these virulence factors, please refer to the text. This figure was created using BioRender.com.
The incubation period of cholera can range from 12 h to 5 days (106, 107). Once ingested, V. cholerae must rapidly adapt to the human digestive system (Figure 2B). To accomplish this, the bacterium uses a complex signal transduction network that regulates gene expression in response to different environments and stimuli throughout the gastrointestinal tract.
Vibrio cholerae is highly sensitive to low pH, and during passage through the stomach, the vibrios undergo an acid tolerance response (ATR) to both inorganic and organic acid. ATR involves several proteins, including the porin OmpU and the transcriptional regulators CadC and HepA, among others (108–110). Despite the ATR, the number of vibrios reaching the small intestine is reduced. In fact, a high infectious dose (108 bacteria) is required to cause severe cholera in healthy volunteers, while a lower dose (105 bacteria) is sufficient when given with antacids to neutralize stomach acid (28, 111).
Upon reaching the small intestine, the main site of colonization, adaptation to antimicrobial agents, such as bile salts and antimicrobial peptides, is crucial. To achieve this, the bacterium modulates its outer membrane protein (OMP) profile through the activation of a tightly regulated signaling pathway known as the ToxR Regulon (112). In the presence of bile salts, ToxR upregulates the expression of OmpU and downregulates the expression of OmpT, two of the most abundant OMPs of V. cholerae (113). The change of the OMP composition also involves removal of OmpT by outer membrane vesicle (OMV) production (114). OmpU and OmpT have distinct channel properties: OmpU is more cation-selective than OmpT, and the bile salt deoxycholic acid blocks OmpT porin activity but not that of OmpU (115, 116). Therefore, OmpU confers resistance to bile salts and antimicrobial peptides, playing a crucial role in the colonization and survival of V. cholerae in the small intestine (87, 88). Other intestinal environmental signals, such as bicarbonate, mucin, and osmolarity, also modulate the expression of virulence factors in V. cholerae (117–120).
To successfully colonize the small intestine, V. cholerae must penetrate a highly viscous mucus layer that is approximately 100–400 μm thick (121), or roughly 30–130 times the size of the bacterium. For this, the vibrios use their flagellum to propel through the mucus layer and reach the epithelial surface (122). It is worth noting that nonmotile vibrios are significantly less efficient at colonization or even avirulent (84). Additionally, the penetration of the mucus layer is facilitated by the hydrolysis of mucins by a group of enzymes, such as HapA, TagA, among others (91, 93–95, 123). Vibrios that fail to penetrate the mucus layer do not colonize the intestinal mucosa and are shed in the feces due to the continuous production and replenishment of mucus (124).
Meanwhile, V. cholerae needs to overcome host immunity (see next section) and the colonization resistance mechanisms of the gut microbiota (125). In this respect, mucin activates the V. cholerae type VI secretion system (T6SS), which operates as a molecular syringe that kills bacterial competitors through the contact-dependent translocation of toxic effectors (104, 126). In mice, V. cholerae T6SS has been shown to attack members of the host commensal microbiota, facilitating intestinal colonization (105). Moreover, T6SS has been suggested as a key mechanism conferring enhanced fitness to pandemic V. cholerae strains (127). However, secondary bile acids generated by gut microbiota can inhibit the assembly of the T6SS apparatus (126). Recently, differences in the gut microbiota among individuals have been suggested as a possible explanation for the susceptibility or resistance to cholera (125, 128).
The initial attachment of V. cholerae to intestinal epithelial cells (IECs) is likely mediated by the GbpA protein. GbpA is regulated by quorum sensing and is expressed at low cell density (129). Additionally, GbpA stimulates mucin secretion by IECs, which in turn enhances GbpA expression (130). GbpA has been shown to bind mucin, and deletion of its encoding gene decreases intestinal colonization in the infant mouse model (100, 101, 130). Other adhesive factors that could play a role in attachment to the intestinal epithelium are the OmpU and FrhA proteins (90, 102, 131).
After attachment to the intestinal epithelium, V. cholerae decreases its motility, proliferates, and forms microcolonies, mostly originating from single vibrio cells (95). Colonizing vibrios express CTX and toxin-coregulated pilus (TCP), which are their main virulence factors. CTX is responsible for the secretory diarrhea characteristic of cholera, while TCP mediates adherence and microcolony formation. Both acidic bile and bicarbonate have been shown to induce CTX and TCP expression via the ToxR regulon (112, 119, 132). Importantly, TCP-deficient mutant strains are unable to colonize animal models and the human intestine (133–135).
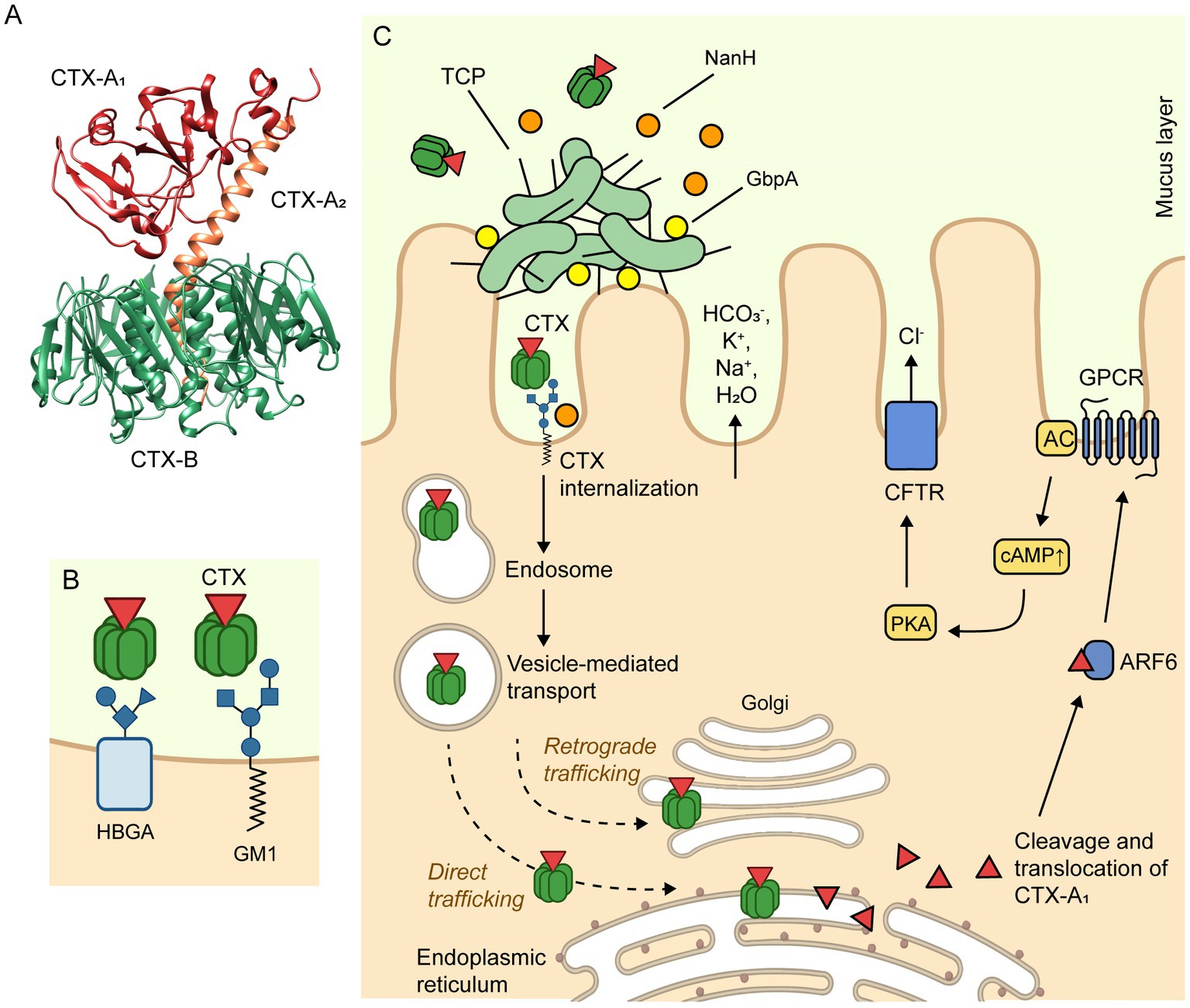
CTX is secreted into the extracellular milieu through the type II secretion system (T2SS) (69). Then, the cellular uptake of CTX occurs via endocytosis, mediated by the binding of CTX-B pentamer to GM1 ganglioside receptors located on the surface of IECs (Figure 3). Of note, NanH cleaves sialic acid from high order gangliosides to release sialic acid and expose the GM1 ganglioside (96, 97). Therefore, NanH promotes the internalization of CTX and its toxigenic effects (139). Although GM1 is considered the primary receptor of CTX, recent studies suggest that CTX-B also binds histo-blood group antigens (HBGAs) at a secondary binding site (140). Additionally, CTX can be released as cargo inside OMVs, which protects the toxin from degradation by intestinal proteases, potentially preserving its toxic effects for longer periods of time (70–72). In particular, CTX-containing OMVs have been shown to be internalized by caveolin-mediated endocytosis in a GM1-independent mechanism that appears to require the presence of OmpU on the vesicle surface (71). After CTX is internalized, cAMP signaling in the IECs is impaired, resulting in a massive release of electrolytes and water into the intestinal lumen, leading to diarrhea (137). The mechanism of action of CTX is described in detail in Figure 3C. Furthermore, other accessory toxins produced by this pathogen can contribute to impaired epithelial barrier function and the development of diarrhea (141). Although 90–95% of infected individuals remain asymptomatic or experience mild symptoms, the remaining 10% develop severe cholera, characterized by profuse watery diarrhea (25). This diarrhea is often described as “rice-water stool” due to its pale, milky appearance (28).
Figure 3. Mechanism of action of cholera toxin. (A) The crystal structure of CTX (PDB accession number 1XTC) was determined by Zhang et al. (136). CTX is composed of a heterodimeric CTX-A subunit, which consists of two polypeptide chains, CTX-A1 (22 kDa) and CTX-A2 (5 kDa), linked by a single disulfide bond. The CTX-A2 helical peptide links the CTX-A1 chain to the pentameric CTX-B subunit, which is composed of five identical polypeptide chains (11.6 kDa). (B) The CTX-B pentamer specifically binds to GM1 gangliosides (primary receptor) or histo-blood group antigens (HBGAs; secondary binding site) present on the apical side of intestinal epithelial cells, promoting the endocytosis of the toxin. (C) The internalization of CTX may occur through clathrin-dependent as well as caveolae- and clathrin-independent endocytosis. Regardless of the mechanism of endocytosis, the CTX is internalized to the early endosomal compartment, trafficked to the Golgi, and then onto the endoplasmic reticulum (ER), where it dissociates into a CTX-A1 and a CTX-A2/CTX-B complex. Next, the CTX-A1 is exported out of the ER to the cytosol, where it is activated by ADP ribosylation factor 6 (ARF6). The ARF6-bound, activated CT-A1 subunit, in turn, activates adenylyl cyclase (AC) by catalyzing ADP ribosylation of a G protein-coupled receptor (GPCR). The AC then catalyzes the conversion of ATP to cyclic adenosine monophosphate (cAMP), increasing the intracellular cAMP concentration. This leads to the activation of protein kinase A (PKA), which phosphorylates the cystic fibrosis transmembrane conductance regulator (CFTR) chloride channel proteins, ultimately resulting in the release of electrolytes (Cl−, HCO3−, Na+, K+) and water into the intestinal lumen, causing the secretory diarrhea characteristic of cholera (137, 138). The figure was created with BioRender.com.
In the late phase of infection, microcolonies of vibrios reach a high cell density, and the nutrients in the intestine decrease. Consequently, vibrios switch from rapid replication to bacteriostasis and downregulate the expression of major virulence factors. Some of them become motile and detach from the epithelial surface moving into the luminal fluid. This process, known as the “mucosal escape response,” is dependent on the general stress response regulator RpoS and the quorum sensing regulator HapR (142–145). Moreover, detachment of vibrios from the intestinal cells is facilitated by the HapA protease, which degrades the GbpA adhesin (129).
Lastly, individuals without effective antibiotic treatment may shed vibrios in their feces for up to 10 days after infection, releasing the bacteria into the environment and increasing the risk of further infections (25). Interestingly, vibrios shed in rice water stool are in a hyperinfectious state (146). These hyperinfectious vibrios are flagellated and highly motile, but most known virulence genes, including those for CTX and TCP, as well as those associated with chemotaxis, are downregulated (147). The exact mechanism for the regulation of the hyperinfectious state remains unknown. In any case, hyperinfectivity is a transient state and is maintained only for a few hours after shedding from the patients (148). Thus, the hyperinfectious state could play a role in the spread of cholera when transmission to another person occurs in a relatively short period of time (149). It is also worth noting that asymptomatic individuals (healthy carriers) are mostly short-term carriers and short-term shedders of vibrios but play an important role in the persistence and transmission of the disease (150).
6. Immune response to choleraNumerous experimental and epidemiological studies have documented that V. cholerae infection induces protection against reinfection for at least 3 years in most patients who recover. In this respect, cholera confers greater protection than a subclinical infection (151). However, several factors can affect the immune response against V. cholerae and the consequent establishment of immunological memory, including age, nutritional status, blood group, endemicity, co-infections, microbiota, and others (152).
Although the exact mechanism behind protective immunity against cholera remains largely unknown, our current understanding of V. cholerae pathogenesis offers some insight into how this bacterium interacts with the intestinal mucosa and triggers multiple arms of the immune system (Figure 4).
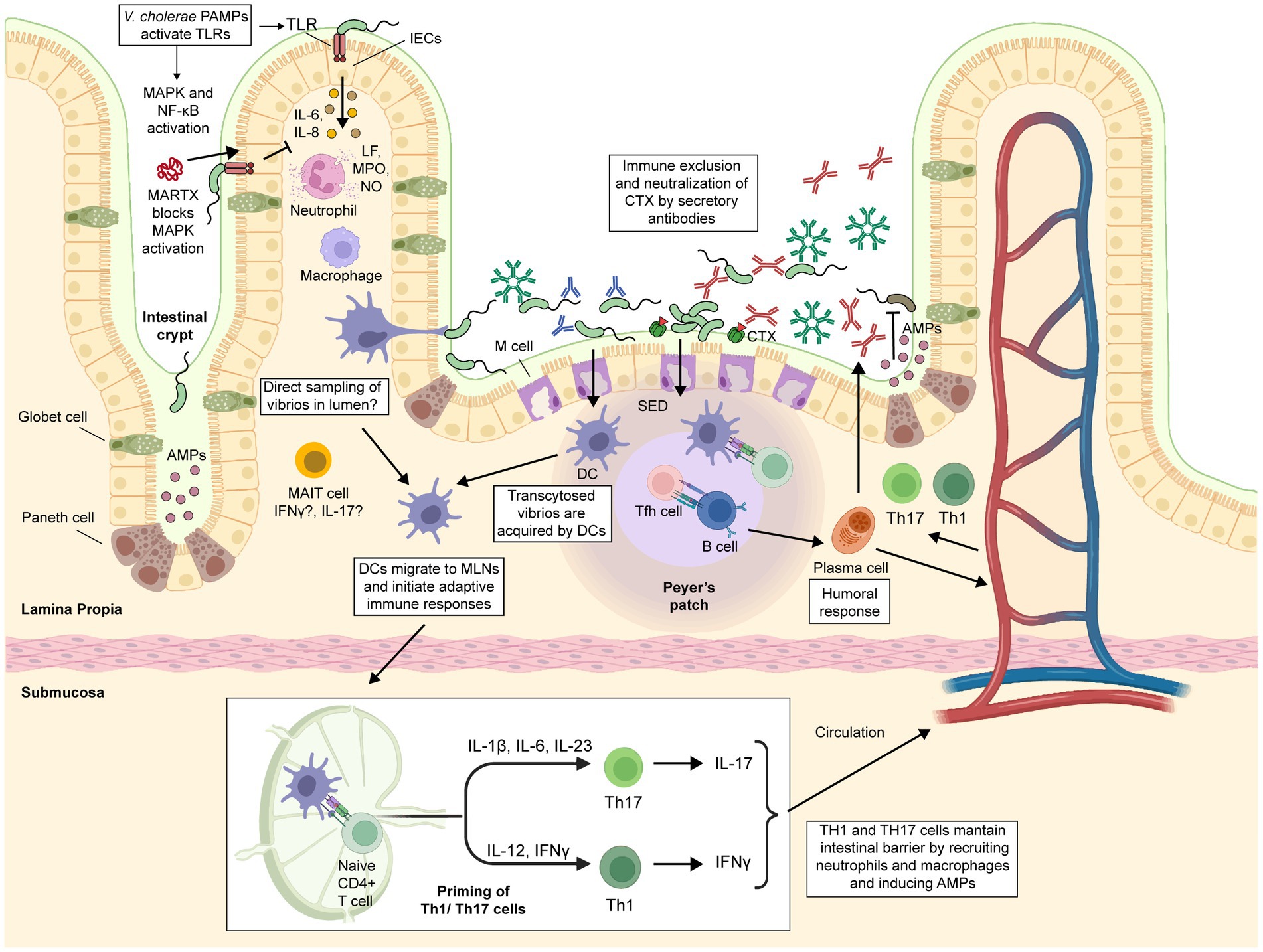
Figure 4. Immune response against cholerae infection. Intestinal epithelial cells (IECs) serve as a physical barrier that limits bacteria to the intestinal lumen. They detect PAMPs such as LPS, flagellin, CTX and OmpU, triggering the secretion of proinflammatory cytokines that recruit innate immune cells such as macrophages, dendritic cells (DCs), and neutrophils. Activated neutrophils increase the inflammation of the intestinal lumen through metabolites such as lactoferrin (LF), myeloperoxidase (MPO), and nitric oxide (NO). M cells take up and transport vibrios from the intestinal lumen to the subepithelial dome (SED) region in Peyer’s patches, where DCs engulf them. Activated DCs migrate to mesenteric lymph nodes, where they produce Th17 or Th1-driving cytokines. Macrophages can also contribute to Th17 or Th1 differentiation through the secretion of IL-23 and IL-6 or IFNγ, respectively. Th1, Th17, and Tfh cells induce B-cell differentiation and expansion. Mucosal-associated invariant T (MAIT) cells are present and highly activated in the lamina propria of the duodenum of cholera patients, but their exact role in the protection against cholera remains to be determined. Secretory antibodies (sIgA and sIgM) prevent vibrios from attaching to the epithelium, blocking their access to the epithelial surface and facilitating their removal through peristaltic activities. Some IgG antibodies could enter the intestinal lumen via passive leakage through a damaged and leaky epithelium. The figure was created with BioRender.com.
6.1. Innate immune responseCholera has traditionally been considered a noninflammatory diarrheal disease; however, this concept has been re-evaluated, and now it is known that some inflammation occurs during the acute phase of the infection, which is followed by a non-inflammatory convalescent phase (153, 154). In fact, patients with cholera in the acute phase exhibit ultrastructural changes in the duodenal mucosa, such as the widening of the intracellular spaces and alterations of the apical junctional complexes. Moreover, these changes correlate with clinical severity and are characterized by the infiltration of innate immune cells, strongly suggesting an inflammatory response at the site of infection (155).
In the small intestine, IECs play a fundamental role in the defense against enteric pathogens. First, IECs constitute a physical barrier that restricts bacteria to the intestinal lumen. Second, they act as sensors to detect pathogen-associated molecular patterns (PAMPs) and release cytokines that recruit immune cells to the site of infection (156). Mechanistically, during the onset of V. cholerae infection, several immunogenic components of this pathogen, such as LPS, flagellins, CTX, and OmpU, can act as PAMPs and be recognized by extracellular and intracellular pattern recognition receptors (PRRs). This triggers the activation of central innate immune pathways, including the myeloid differentiation primary response gene 88 (MyD88), mitogen-activated protein kinase (MAPK), and nuclear factor kappa light-chain enhancer of activated B cells (NF-κB), which in turn activate the secretion of several proinflammatory cytokines (154, 157–162).
For example, V. cholerae flagellins induce the expression of IL-1β and IL-8 in IECs by interacting with Toll-like receptor 5 (TLR5) and activating NF-kB and MAPK pathways (159, 161). Likewise, OmpU induces the expression of IL-6, IL-8, and MCP-1 (CCL2) in IECs (163, 164). Moreover, CTX increases intracellular cAMP, leading to IL-6 secretion in IECs (165, 166). These studies were further supported by a transcriptomic analysis of IECs from patients with cholera in the acute phase, where an upregulation of several genes associated with innate immunity was observed (160). Remarkably, activation of the MAPK and NF-κB pathways persisted even 30 days after infection. Furthermore, multiple TLRs, including cell surface TLRs 1, 2, 4, 5, and 6, as well as the endosomal TLRs, including TLR3, TLR7, and TLR8 were upregulated (160).
Among the cytokines mentioned, IL-8 is a potent chemoattractant that recruits polymorphonuclear leukocytes and T cells to the infection site, and stimulates neutrophil degranulation and phagocytosis (167, 168). In addition, the CCL2 chemokine induces the migration of monocytes, dendritic cells, and memory T-cells (169, 170), while IL-6 secretion by IECs activates neutrophil degranulation in the intestinal lumen (166). As a result, innate immune cells, particularly neutrophils, are recruited to the site of infection during the acute phase of cholera (153, 155, 171). Furthermore, a recent study showed that mucosal-associated invariant T (MAIT) cells, an innate-like lymphocyte known to provide immediate effector functions in response to infections, are present and highly activated in the lamina propria of the duodenum of cholera patients (172). Recent evidence suggests that MAIT cells can also provide B cell help and support antibody production at the mucosa level (173); however, further investigation is needed to determine the exact role of MAIT cells in the protection against cholera.
Once neutrophils arrive at the infection site, they express metabolites such as lactoferrin (LF), myeloperoxidase (MPO), and nitric oxide (NO) (153, 174, 175). This may explain the detection of elevated levels of LF and MPO in stools and NO metabolites (NO2−/NO3−) in serum of patients with cholera during the acute phase (174, 175). Of note, V. cholerae is highly susceptible to the bactericidal action of LF (176, 177). By contrast, in the convalescence phase (~ up to 30 days post infection), an increase of mast cells and eosinophils and their respective effector molecules chymase and IL-3 have been reported (153). Consequently, the activation of proinflammatory signaling pathways, the recruitment of innate immune cells, and their effector functions are fundamental in the initial defense against V. cholerae.
Despite the above, V. cholerae has some strategies to evade the innate immune response of the host (178). A recent study demonstrated that the accessory MARTX (multifunctional-autoprocessing repeats-in-toxin) toxins secreted by some V. cholerae strains can block the MAPK signaling pathway in T84 cells grown in vitro. Suppression of MAPK signaling in IECs prevented the recruitment of innate immune cells, and thus this mechanism could protect colonizing vibrios from neutrophil-mediated clearance (74). Importantly, the immunomodulatory effect of these toxins may contribute to the differences in inflammation observed between various V. cholerae strains (158). In fact, the current predominant circulating altered El Tor strains lack the MARTX toxins due to a stop codon (179), which could explain in part why these hybrid strains cause a more severe diarrhea and increased intestinal inflammation (158). This raises the question: are innate immune responses in cholera beneficial or detrimental to the host? It is likely that adequate tuning of the innate immune system and a subsequent moderate inflammatory response can be protective against severe cholera.
The gut-associated lymphoid tissues (GALT) play a vital role in developing immunity following natural exposure to enteric pathogens (180). GALT is divided into inductive sites, such as the Peyer’s patches (PP) and mesenteric lymph nodes (MLNs), and effector sites, such as the lamina propria and the intraepithelial lymphocyte compartment (181). Consequently, upon exposure to V. cholerae, protective immunity against this pathogen is expected to largely depend on cellular processes that occur in GALT. In fact, in the rabbit ileal loop model, M cells take up and transport vibrios from the intestinal lumen to the subepithelial dome (SED) region in the PP (182). Thus, it is likely that resident DCs and macrophages in the SED become activated and then phagocytose these vibrios during infection in humans.
CTX induces an increase in intracellular cAMP in innate immune cells, leading to the production of IL-1β, TNF-α, and IL-6 (183). In particular, it has been shown that CTX has an immunomodulatory effect on DCs by stimulating their maturation, as well as the expression of MHC class II and costimulatory molecules (184, 185). CTX activates DCs to produce Th17-driving cytokines, including IL-6, which promotes the differentiation of Th17 cells (186, 187). Significantly, CTX also induces the migration of DCs from the SED region to B and T cell zones, where antigen presentation occurs (188). Therefore, the DCs activated by CTX can induce strong humoral and cellular immunity.
Some insights into the role of macrophages against cholera infection have been obtained using the THP-1 human monocyte-like cell line. THP-1 cells exposed to live toxigenic V. cholerae upregulate IL-23 expression (189). In another study, THP-1 cells stimulated with V. cholerae LPS exhibited increased expression of TNF-α, IL-1β, and MIP-3α through interaction with TLR4 and subsequent activation of the MyD88 pathway (190). It is important to note that both IL-23 and IL-1β are essential for the differentiation of Th17 cells (191, 192).
6.2. Adaptive immune responseThe subsequent adaptive immune response is complex and involves both humoral and cellular mechanisms. In the acute stage of cholera, studies have shown that lamina propria lymphocytes (LPLs) in the duodenum express significant amounts of IL-6, IL-8, IL-12β, and IL-17 cytokines (162, 193). Later, at day 7 post-infection, cholera induces cellular immune responses in blood compatible with Th1 (IFN-γ) and Th17 (IL-17) profiles (193). Additionally, patients who recover from cholera display an increased percentage of gut-homing CD4+ T cells and gut-homing B cells that peak in the circulation 7 days after the infection. Th17 lineage and other IL-17-producing cells play a key role in host defense against bacteria at mucosal surfaces (191), making the Th17 response to V. cholerae highly significant. By contrast, the level of gut-homing CD8+ T cells reaches its peak in circulation on day 21 (194, 195).
Cholera also triggers follicular helper T (Tfh) cells, which are essential for germinal center formation, affinity maturation, and the development of most high-affinity antibodies and memory B cells (196). A recent study demonstrated that cholera infection in the acute phase induces a significant increase in circulating Tfh cells, which impacts the development of antigen-specific B cells and consequent immunoglobulin production (197).
Considering the pathogenesis of V. cholerae, a humoral response capable of neutralizing the CTX, blocking bacterial adherence to the mucosa, and opsonizing the bacteria to mediate their clearance is expected. Consistently, patients who recover from cholera develop systemic IgM, IgG, and IgA antibodies, as well as secretory IgA (sIgA) antibodies, which target several antigens, including CTX-A and CTX-B subunits, LPS, O-specific polysaccharide (OSP), LPS, NanH, flagellins (FlaB, FlaC, and FlaD), TcpA, and HlyA (139, 198–204). Nevertheless, while CTX-specific antibodies confer short-term immunity, the antibacterial (vibriocidal) antibodies are associated with protection against colonization and long-term protective immunity (205).
The best-characterized correlate of protection against cholera is the vibriocidal antibody titer (VAT), which measures the minimum concentration of serum required for antibody-dependent complement-mediated bacterial killing (206). However, VAT is not a comprehensive predictor of long-term immunity. For instance, a specific VAT threshold for absolute protection has not been identified; infection still occurs in a few individuals with very high titers (207). Moreover, there is a lack of mechanistic connection between levels of circulating VAT and prevention of V. cholerae colonization at the intestinal mucosal surface level. At the same time, anti-body-dependent complement-mediated bacterial killing is relevant for immunity against systemic infections, it appears to be less important at the intestinal mucosa due to low complement levels at this site (206, 208).
The mechanism by which IgG enters the intestinal lumen is unclear, but it may occur via passive leakage through a damaged and leaky epithelium or through FcRn-mediated epithelial transport (209, 210). Notably, recent studies have demonstrated that IgG anti-OSP contributes to protection against cholera by inhibiting the motility of V. cholerae, potentially limiting its access to the apical surface of the intestine (211). It is also possible that anti-OSP sIgA may contribute to protection by inhibiting motility and trapping the bacteria at the mucosal surface (1, 212). Even in the absence of circulating anti-OSP antibodies, OSP-specific memory B cells may maintain protective immunity by rapidly expanding and differentiating into plasmablasts upon antigen exposure (213). Furthermore, a recent study showed that patients with cholera develop IgG, IgA, and IgM antibodies against NanH, and that plasma responses targeting this antigen correlate with protection (214). The protective role of other antibacterial antibodies against cholera is currently unknown.
Thus, this body of studies demonstrates that cholera infection stimulates innate cells at the site of infection, primarily neutrophils and their corresponding effector molecules. The subsequent adaptive response is characterized by Th1, Th17, and Tfh CD4+ cells, which shape the antibody production targeting the CTX and various surface-exposed antigens. However, there are currently many knowledge gaps in understanding how these immunological processes occur. In this regard, to develop a highly effective cholera vaccine, it may be necessary to mimic these immune responses. As such, progress should be made in understanding the differences between the immune response triggered by V. cholerae infection and that induced by vaccination. This could pave the way for the development of the next generation of cholera vaccines.
7. Current vaccines licensed worldwide or with restricted licenseThe knowledge gained on immunity against V. cholerae has not only facilitated the development of current cholera vaccines, but also highlighted the possibility of developing novel vaccines that provide broader and longer-lasting protection. In this section, we will briefly review licensed cholera vaccines, while subsequent sections will focus on candidate vaccines currently undergoing clinical and preclinical evaluation.
In the 1960s, several large field studies conducted in Asian countries showed that injectable killed whole-cell cholera vaccines had modest efficacy and a high rate of adverse reactions, such as fever, local pain and swelling (215). Subsequently, interest shifted to exploring the potential of oral vaccination, which led to the development of the OCVs. Oral vaccines mainly interact with the immune system through the Waldeyer’s tonsillar ring in the oral cavity or via the PP in the small intestine. Compared to vaccines administered by parenteral routes, oral vaccines have been found to induce stronger immune responses at the intestinal mucosa level, partly via antigen-specific sIgA (216). However, oral vaccines face some challenges, including the potential degradation of acid-labile antigens in the stomach, the lack of licensed oral adjuvants for human use, and the difficulty of their release at mucosal immune inductive sites (217).
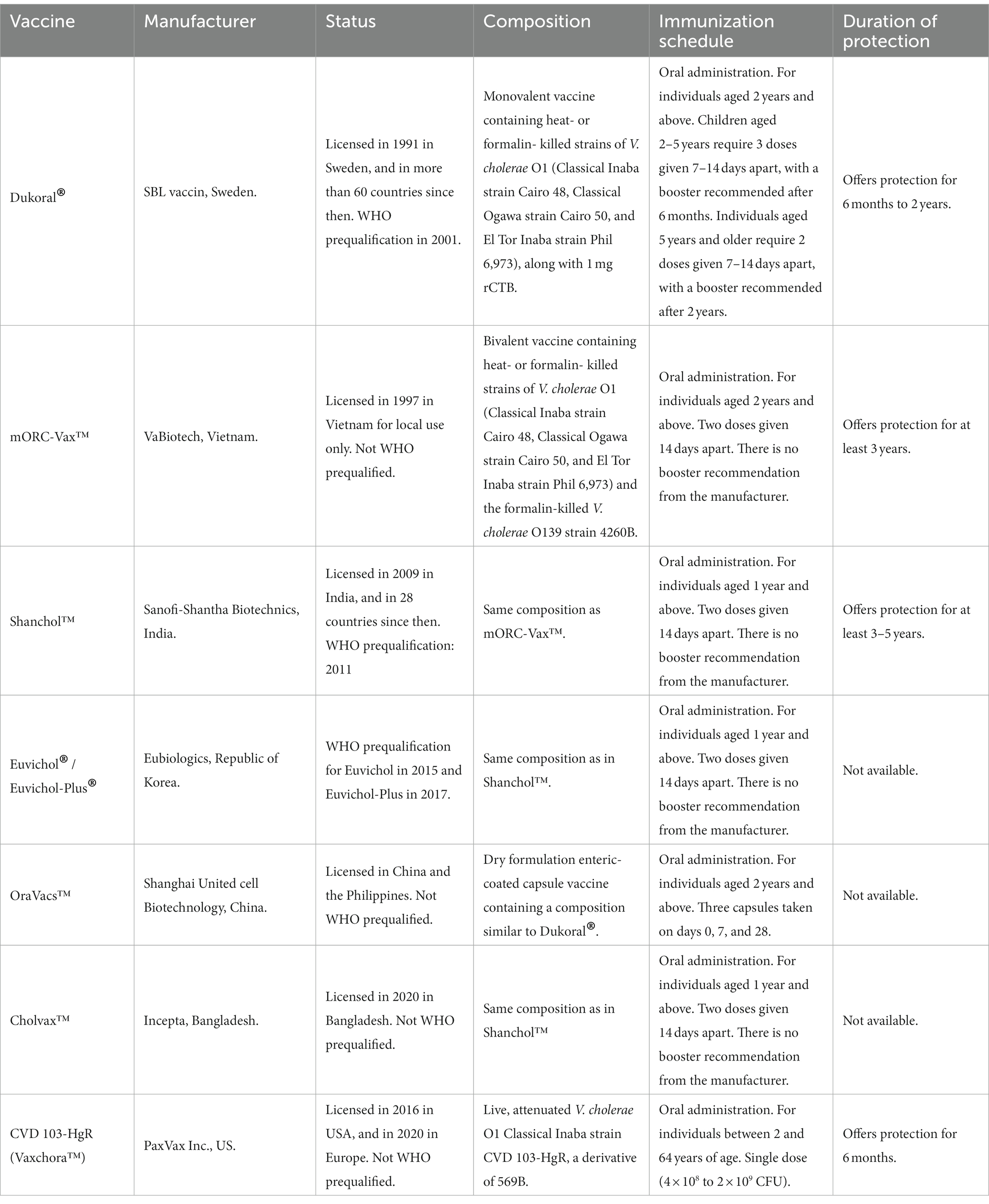
At present, four OCVs based on killed whole cell vibrios are prequalified by the WHO (meaning that they can be purchased by United Nations agencies): Dukoral®, Shanchol™, Euvichol, and Euvichol-Plus (Table 3 and Box 2) (217).
Table 3. Licensed cholera vaccines.
BOX 2 Advantages and limitations of killed OCVs.Killed OCVs possess several characteristics that make them effective in combating cholera:
• Safety: These vaccines have been proven safe, with only minor side effects reported.
• Easy administration: They can be easily administered in mass vaccination campaigns and in settings where injection-based vaccines may be logistically difficult to implement.
• Cost-effectiveness: Killed OCVs are relatively inexpensive, making them accessible to populations in resource-limited areas where cholera is prevalent.
• Herd immunity: OCVs not only protect the individuals who receive them but also create herd immunity, which can help to decrease transmission of the disease in the community (218, 219).
While killed OCVs offer several benefits as a tool for controlling cholera, they also have some limitations:
• Limited effectiveness: Their effectiveness can vary depending on the vaccinated population and the level of cholera transmission in the area. The protection provided by OCVs is short-term and decreases over time.
• Limited immune response: These vaccines do not contain live bacteria; thus, the immune response elicited may differ from that triggered by a natural cholera infection. This difference may result in a different pattern of immune response and antibody production, which can affect the duration and quality of the immunity provided.
• Cold chain requirements: They must be stored at a specific temperature range (typically between 2 and 8°C) to preserve their immunogenic properties, which can be challenging in areas with limited infrastructure.
• Requirement for multiple doses: They require at least two doses to provide adequate protection, which can be a barrier to achieving high coverage in some settings.
• Limited role in outbreaks: They do not provide immediate protection against cholera and are not intended to replace other control measures.
Dukoral® was licensed in 1991 and since then has been distributed in over 60 countries. It is a monovalent vaccine composed of a mixture of three heat- or formalin-inactivated V. cholerae O1 strains (Classical Inaba strain Cairo 48, Classical Ogawa strain Cairo 50, and El Tor Inaba strain Phil 6973) along with the recombinant CTX-B (rCTX-B) subunit. The vaccine is free of the CTX-A subunit due to its toxicity. A sodium bicarbonate buffer is also added to the formulation to prevent the degradation of rCTX-B by gastric acid. This vaccine can be administered to individuals over 2 years of age and requires at least two doses for optimal efficacy. The protective efficacy (PE) of this vaccine has been demonstrated in several field trials in different countries, achieving over 80% protection in the first 6 months and gradually decreasing thereafter, ultimately providing negligible protection after 2 years. No significant severe adverse effects were attributed to this vaccine (220–222). Further analyses of volunteers vaccinated with Dukoral® revealed that this formulation induces high levels of specific sIgA antibodies and IFN-γ production in the duodenal mucosa (223). Notably, Dukoral® also provides significant protection for 3–9 months (PE: 67%) against diarrhea caused by enterotoxigenic E. coli (ETEC) producing heat-labile toxin (LT). This cross-protection is due to the cross-reactivity between the CTX-B subunit and LT (224).
In the late 1980s, the technology for manufacturing Dukoral® was transferred from Sweden to Vietnam for local production. This vaccine contained the same Dukoral strain composition, but the rCTX-B subunit was removed to simplify manufacturing, reduce costs, and improve stability. In 1992, the O139 epidemic in India and Bangladesh led to the addition of a killed O139 strain. This formulation was initially licensed in Vietnam as ORC-Vax™ and later after its modification as mORC-Vax™. It should be noted that the incorporation of the O139 component did not affect the responses to the original Dukoral components; instead, anti-O1 and anti-O139 antibodies were induced in serum and the intestinal mucosa (225, 226). However, the National Regulatory Agency (NRA) of Vietnam at that time did not have WHO approval, which limited the international use and WHO prequalification of this Vietnamese OCV. To make the vaccine available for international use, the manufacturing technology was transferred from Vietnam to Shantha Biotechnics in India, which had a WHO-approved NRA (195, 227). The PE of this vaccine was evaluated in a trial conducted in Kolkata, demonstrating that a two-dose immunization schedule provides an overall 65% protection over a five-year observation period. In 2009, this vaccine was licensed in India as Shanchol™, and WHO prequalified it in 2011 (228, 229).
The manufacturing technology of Shanchol™ was later transferred to Eubiologics in Seoul, Republic of Korea, resulting in the production of Euvichol®, which has an identical composition to Shanchol™. Studies in different countries have shown that Euvichol® and Shanchol™ elicit similar vibriocidal antibody responses and have comparable safety profiles. Euvichol® received licensure and WHO prequalification in 2015. Euvichol-Plus® is an improved vaccine that utilizes plastic tubes instead of conventional glass vials, providing better conditions for storage, transportation, and administration. This change has facilitated the delivery of this vaccine in emergency situations or humanitarian campaigns. Euvichol-Plus® received WHO prequalification in 2017 (230).
Two killed OCVs are licensed in some countries but are not WHO-prequalified. OraVacs™ is a dry formulation enteric-coated capsule vaccine containing a composition similar to Dukoral®. It is licensed in China and the Philippines (231). Cholvax™ is licensed in Bangladesh for use in the national cholera control program and has demonstrated safety and immunogenicity comparable to Shanchol™ (232).
The OCVs have achieved an important milestone in public health by providing herd immunity in vaccinated communities, thereby reducing person-to-person transmission (218, 219). In addition, the accumulation of evidence regarding the safety and efficacy of these vaccines has led the WHO to recommend their mass use as a preventive strategy in cholera-endemic areas, as well as a response measure during cholera outbreaks. Consequently, the WHO established the global OCV stockpile in 2011, which received support from the Global Alliance for Vaccines and Immunizations (Gavi Alliance) in 2014 (233). The main objectives of the OCV stockpile are to store and provide cholera vaccines during outbreaks and humanitarian campaigns, among other measures to control this disease. Presently, the OCV stockpile primarily uses Euvichol-Plus as its main formulation.
Despite their importance and usefulness, killed OCVs have several limitations. First, the PE of these vaccines is low (~42%) in children under the age of five, who are most vulnerable to the long-term effects and higher mortality associated with cholera (228). Second, they require multiple doses to achieve a high level of protection, which increases economic costs and the time required to elicit immunity. In fact, with a single dose, PE is only 8% for those under the age of five and 57.5% for those over the age of five (234, 235). Third, PE is short-term since it begins to decrease after 6 months and practically disappears after 3 or 5 years. In some sense, these limitations may be intrinsically related to the nature of killed vaccines. For instance, the in vitro cultures used to grow the vibrios included in these formulations do not reproduce host conditions and some important antigens may not be expressed. This is the case of the TcpA antigen, which is absent in the killed OCVs (236). Moreover, the formalin and heat treatment used to kill the bacteria may destroy or alter epitopes (237). Ultimately, killed vaccines are unable to mimic natural infection, so immune stimulation may be different from what is needed to achieve long-lasting protection.
Live attenuated OCVs have the potential to overcome many of the intrinsic limitations of killed OCVs. For instance, live attenuated vibrios closely mimic natural infection, and thus, they may trigger immune responses in the GALT, with the potential to target antigens which are only expressed in vivo during infection (199). Moreover, live attenuated OCVs may require a single dose, reducing the time required to achieve significant PE; this is particularly advantageous for individuals requiring travel at short notice to areas where an outbreak is occurring or where cholera is endemic (238).
Currently, only one live attenuated OCV is available, named Vaxchora™, which is approved in the United States and Europe for travelers visiting regions where cholera is endemic (238). The approval of Vaxchora™ in other markets is pending. This vaccine is based on the V. cholerae strain CVD 103-HgR, serogroup O1, serotype Inaba, classical biotype, which is derived from the strain 569B. The CVD 103-HgR strain is genetically modified and contains a deletion of the ctxA gene and an insertion of the Hg++ resistance gene to enable differentiation of the vaccine strain from the wild type (239). Although the CVD 103-HgR strain cannot produce active CTX, it can synthesize the CTX-B subunit and the TcpA antigen, and colonize the small intestine transiently (199). The initial CVD 103-HgR formulation was introduced in 1993, and since then, it has been manufactured by various companies and known by other trade names such as Orochol®, Mutacol®, and Orochol-E®.
The effectiveness of the CVD 103-HgR vaccine was initially evaluated
留言 (0)