
記住我
Gallstone disease (GS) is a common gastrointestinal disease worldwide. Epidemiological surveys have revealed that the prevalence of GS among adults in the United States (US) and Europe is approximately 5–25% (1, 2), whereas among Asians, it is relatively low (3). The annual healthcare cost associated with GS in the US is approximately $6 billion (4), placing a significant burden on public health. Most patients with GS are asymptomatic and are diagnosed through physical examination. A small number of patients may experience abdominal pain, loss of appetite, nausea, and vomiting. In a very small number of patients, GS involving the common bile duct can lead to cholangitis and pancreatitis, which can be life-threatening in severe cases (5, 6). Previous studies have reported the potential mechanisms and risk factors for developing GS; however, validated indicators for predicting or evaluating the risk of developing GS are lacking.
The arm circumference (AC) is a simple, direct, cost-effective, and noninvasive indicator of nutritional status and risk of developing diseases. AC reflects an individual’s muscle mass and fat reserves, particularly the muscle-to-fat ratio in the upper arm area. In developing countries, AC has been utilized to evaluate the nutritional status of children and adolescents, with a small AC value indicating that a child or adolescent may be malnourished or have stunted growth (7–10). Moreover, a low AC value is linked to a higher risk of mortality in patients with cirrhosis and cardiac failure, those undergoing hemodialysis, and the elderly (11–15). Recent studies have shown that AC can be used as a novel bioindicator to assess obesity, insulin resistance (IR), metabolic syndrome (MetS), and non-alcoholic fatty liver disease (NAFLD) in adults (16–19).
Although waist circumference (WC) is an established indicator of central obesity and metabolic health, AC provides complementary information about body composition, particularly in terms of the muscle-to-fat ratio and upper extremity nutritional status. Unlike WC, which primarily reflects abdominal fat distribution, AC captures a broader physiological profile, including peripheral muscle and fat reserves. This distinction is important when exploring conditions like GS, where factors beyond central obesity may contribute to disease risk. Furthermore, there are specific clinical scenarios where accurate WC measurement may not be feasible, such as in individuals with abdominal deformities, surgical scars, or extreme obesity. In such cases, AC offers a practical and reliable alternative for assessing body composition.
However, the relationship between AC and GS remains unclear. Given that GS is, to some extent, a metabolic disorder, we hypothesized a link between AC and GS. This study aimed to evaluate the relationship between AC and the prevalence of GS in US adults, utilizing data from the National Health and Nutrition Examination Survey (NHANES) to provide evidence of AC’s potential role in adult health assessments. By focusing on AC as a less explored but complementary bioindicator, we sought to uncover novel insights into the relationship between body composition and GS, thereby contributing to a more comprehensive understanding of metabolic health.
2 Materials and methods 2.1 Study design and participantsParticipant information was extracted from NHANES, an open-source database officially maintained by the Centers for Disease Control and Prevention. The NHANES provides valuable data support for disease prevention, public health policy development, clinical practice, and individualized medicine and plays a very important role in nutritional assessment, research, and education. NHANES is updated biennially with a population of approximately 10,000 at a time. NHANES employs a stratified multistage probability sampling design to ensure the representativeness of its sample at the national level. This approach involves several key steps: first, the population is stratified into distinct groups based on relevant characteristics; then, primary sampling units (PSUs) are selected, followed by the identification and selection of secondary sampling units (SSUs) within each PSU. In the next phase, households are randomly sampled from the SSUs. Additionally, NHANES incorporates an oversampling strategy to ensure that specific subgroups, such as minority populations or those with specific health conditions, are adequately represented in the final sample. This comprehensive sampling methodology ensures that the data collected are reflective of the diverse U.S. population, providing a robust basis for national health assessments. Due to the coronavirus disease 2019, NHANES was suspended in March 2020. Data from the 2017–2020 cycle were utilized for the analysis as the GS questionnaire was exclusively available during these years. The questionnaire was conducted exclusively among adults who were 20 years of age or older.
2.2 Definition of dataAC was an exposure variable in this study. For AC measurement, the participant stood upright with the arm hanging loosely, and the examiner stood facing the participant’s right side, comfortably rolling up the tape measure at the midpoint of the upper arm without pressing on the skin. The tape was placed perpendicular to the long axis of the upper arm with the ends overlapping, and the resultant tape was located on the side of the arm. The AC was recorded to the nearest millimeter (20).
2.3 Data collectionA questionnaire was used to assess patients with GS. GS in the NHANES dataset (2017–2020) was defined based on self-reported medical history, where participants were asked if they had ever been told by a doctor that they had gallstones. The main covariates included in this study were demographic variables, comorbidities, dietary intake, laboratory findings, and other parameters. Detailed results are presented in Table 1. All study participants were asked to complete two 24-h dietary recalls, which were conducted on separate, non-consecutive days within the same survey cycle. To provide a more accurate estimate of dietary intake, the average of the two recall days was calculated and used in the subsequent analysis. This method helps account for day-to-day variability in dietary consumption, offering a more reliable representation of participants’ typical food intake. Detailed procedures for measuring all covariates are available on the official NHANES website. The official link is: www.cdc.gov/nchs/nhanes. All NHANES protocols adhered to the U.S. Department of Health and Human Services Policy for the Protection of Human Research Subjects and underwent annual review and standardization by the NCHS Research Ethics Review Board. All NHANES participants signed an informed consent form. Therefore, no additional permission or ethical review was required for this study.
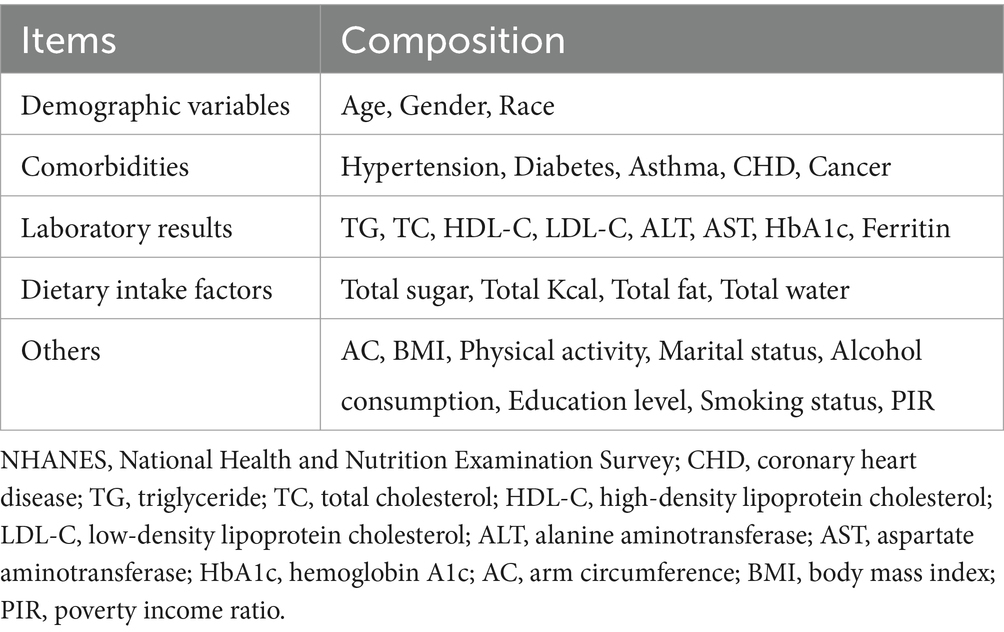
Table 1. Covariates extracted from NHANES (2017–2020).
2.4 Outcome indicatorsThe outcome variable was the prevalence of GS.
2.5 Statistical analysisCategorical variables were expressed as numbers and percentages (%), and comparisons between groups were made using Pearson’s χ2 test or Fisher’s exact test. Continuous variables are expressed as medians and interquartile ranges, and comparisons of continuous variables between groups were performed using a t-test or one-way ANOVA. Following these guidelines, multivariate logistic regression models were performed to examine the association between AC and the prevalence of GS across various model specifications: Model 1, which did not include adjustments for covariates; Model 2, which accounted for age, sex, and race, and Model 3, which was additionally adjusted for physical activity, smoking status, diabetes, hypertension, coronary heart disease (CHD), triglyceride, alanine aminotransferase, total kcal intake. The relationship between AC and the prevalence of GS was further assessed using a generalized additive model regression combined with smoothed curve fitting (penalized spline method). When a nonlinear relationship was observed, a logarithmic likelihood ratio test was employed to determine the inflection point values. Subgroup analyses were performed according to age, sex, race, hypertension, diabetes, and body mass index (BMI). A p-value of less than 0.05 was considered statistically significant. All analyses were conducted using R version 4.0.2 (R Foundation) and Empower software (X&Y Solutions, Inc., Boston, MA, USA).
3 Results 3.1 Participants’ baseline characteristicsThe study included a total of 8,081 participants, of whom 849 had a history of GS. Figure 1 illustrates the participant selection process. Table 2 presents the baseline characteristics of the study participants. The GS group exhibited higher AC values compared to the non-GS group [33.55 (5.20) vs. 35.27 (6.00), p < 0.001]. The patients in the GS group were older; had a higher BMI; and a higher prevalence of hypertension, diabetes, asthma, CHD, and cancer. Moreover, significant differences were observed between the two groups in terms of sex, race, physical activity, marital status, alcohol consumption, smoking status, total calory intake, total fat intake, and total triglycerides, hemoglobin A1c, and Ferritin levels (All p < 0.05).
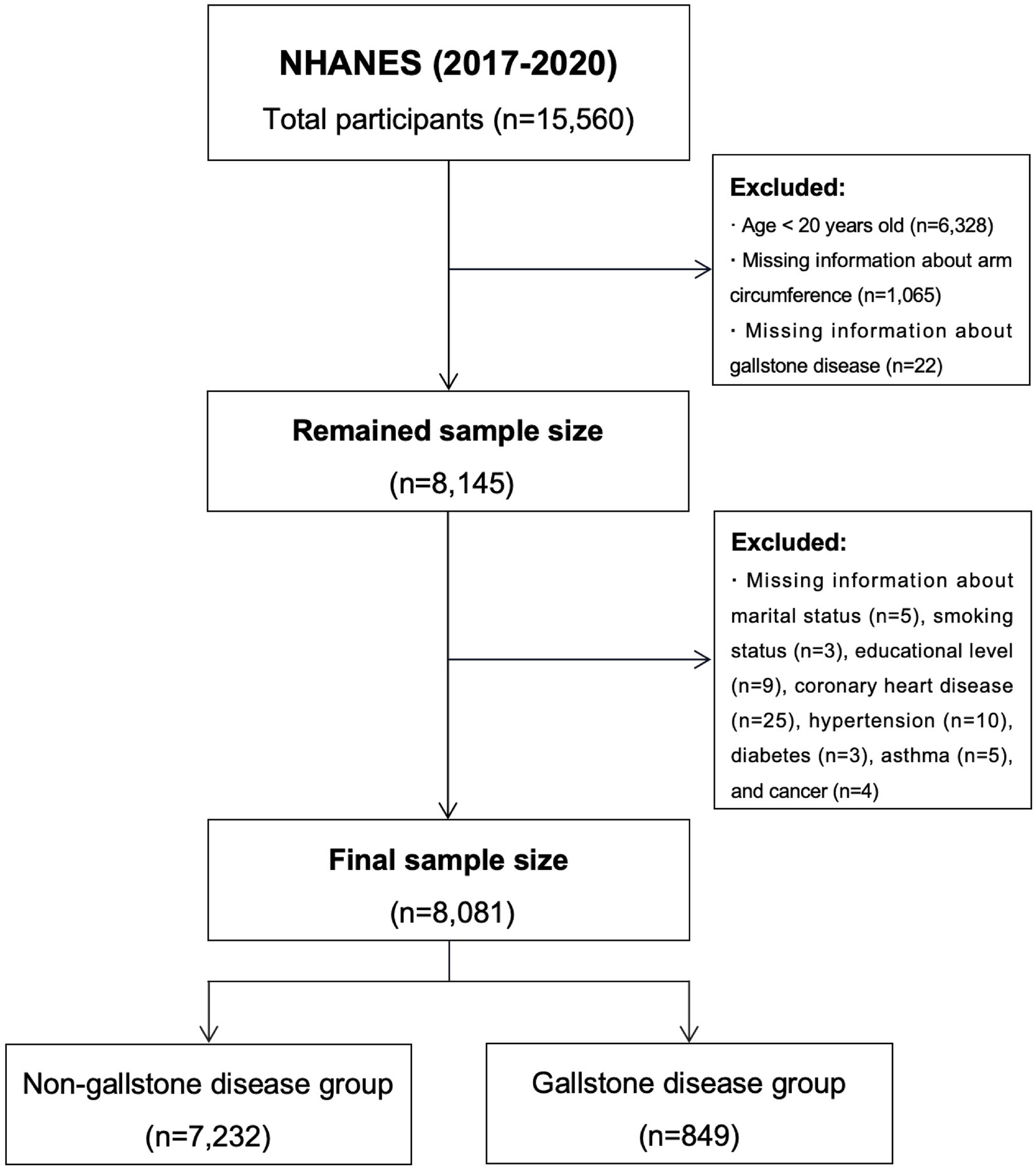
Figure 1. Flowchart for participants from NHANES (2017–2020).
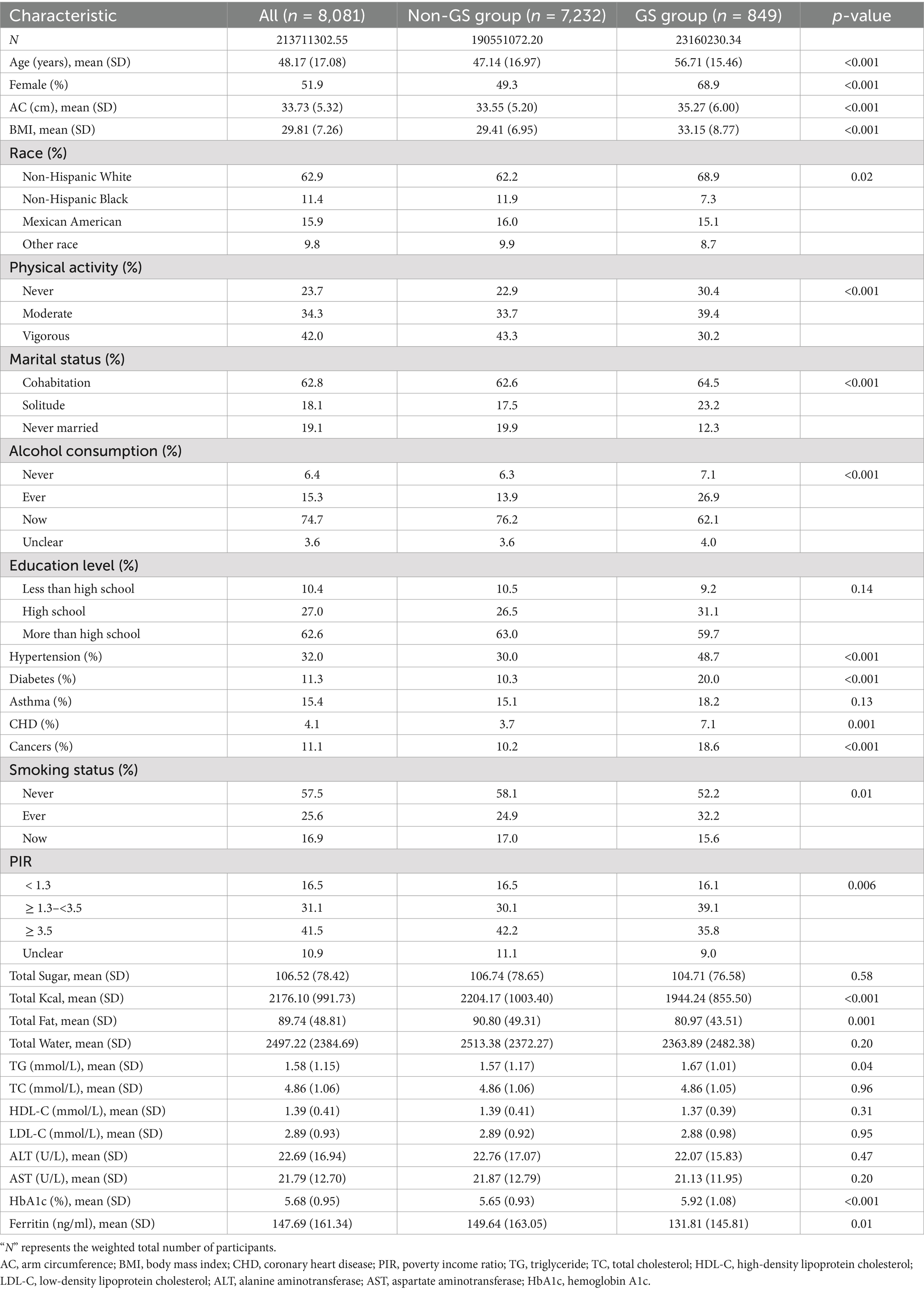
Table 2. Baseline characteristics of participants (weighted).
3.2 Logistic regression analysis between AC with gallstone disease prevalenceThe multivariable logistic regression analysis results revealed a positive correlation between high AC values and a high prevalence of GS. This relationship persisted even in the fully adjusted model (Model 3) (OR = 1.08, 95% CI: 1.07–1.10), meaning that for every 1 centimeter increase in AC, the prevalence of GS increases by 8%. When AC was converted from a continuous variable to a categorical variable (tertiles) for further analyses, we found a 2.43-fold increase in the prevalence of GS in the third tertile (OR = 2.43, 95% CI: 1.91, 3.10) compared with that in the lowest AC tertile (tertile 1). The comprehensive results are displayed in Table 3.
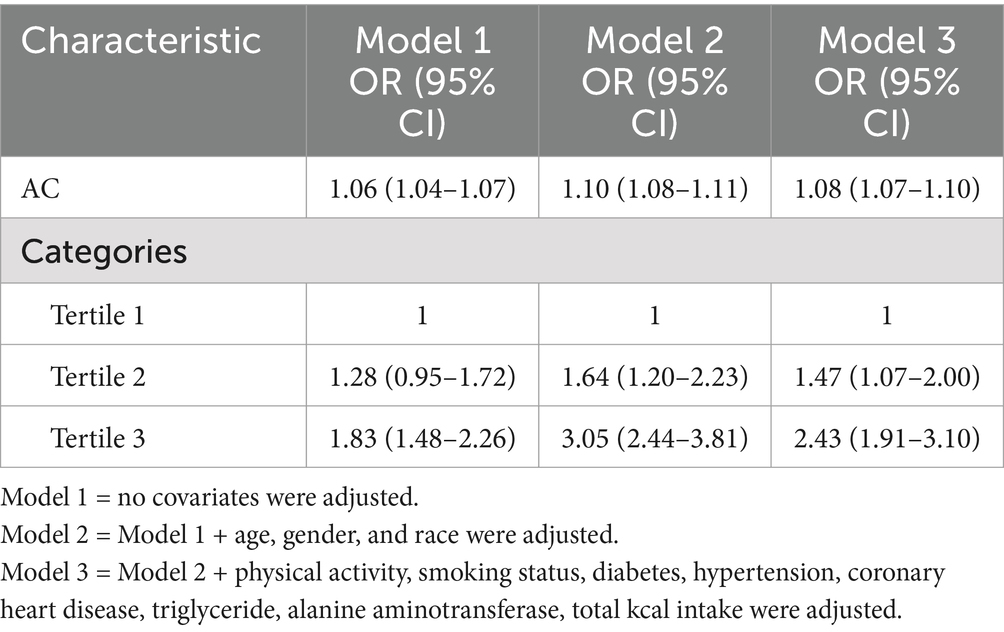
Table 3. Logistic regression analysis between AC with gallstone disease prevalence (weighted).
3.3 Dose–response and threshold effects of AC on GS prevalenceThe relationship between AC and the prevalence GS was further explored using generalized additive models and smooth curve fitting. The results demonstrated a significant positive linear correlation between AC and GS prevalence (Figure 2 and Table 4). In Figure 2, the confidence intervals (CIs) around the dose–response curve narrow as AC increases from approximately 25 cm to 50 cm, reflecting greater precision and reliability in this range. For higher AC values (>50 cm), the CIs widen slightly due to fewer participants with very large AC, introducing greater variability. Nonetheless, the overall positive linear relationship between AC and gallstone disease prevalence remains robust, as supported by the logistic regression results in Table 3.
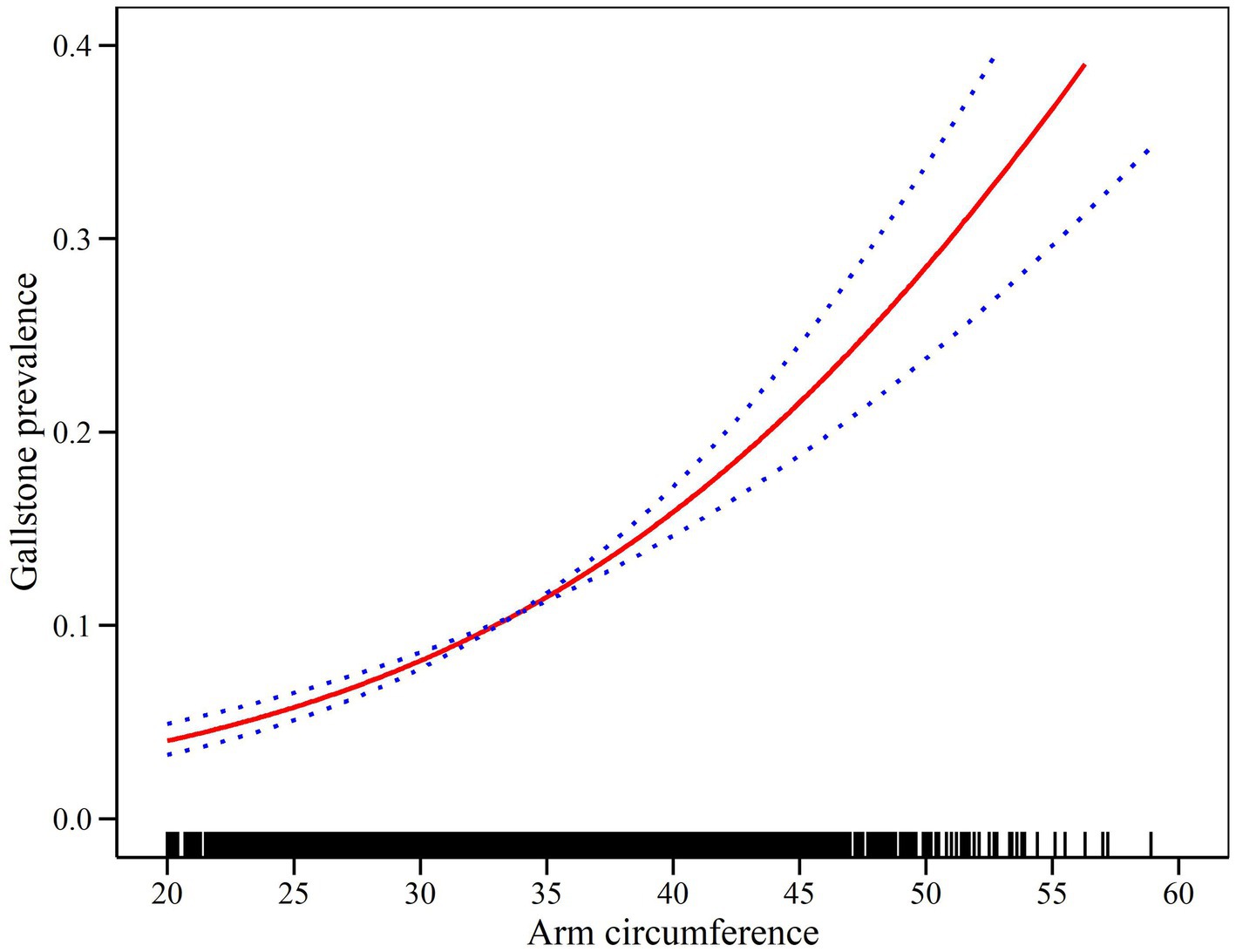
Figure 2. Density dose–response relationship between AC and gallstone disease prevalence. The area between the upper and lower dashed lines representes the 95% CI.
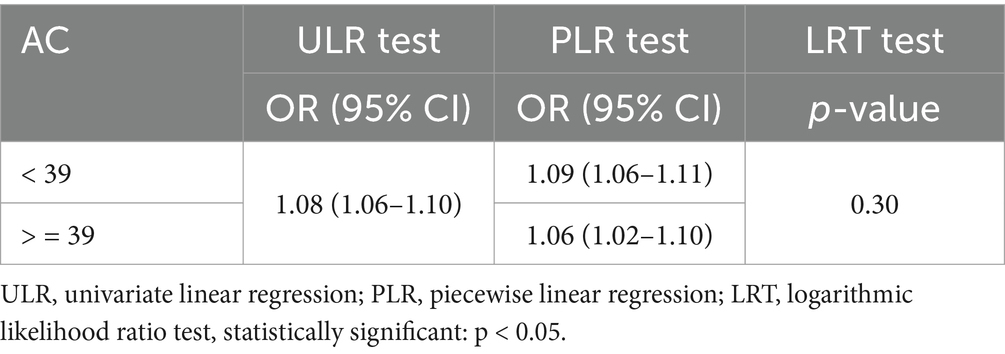
Table 4. Two-piecewise linear regression and logarithmic likelihood ratio test explained the threshold effect analysis of AC with gallstone disease prevalence.
3.4 Subgroup analysisSubgroup analyses revealed a consistent positive association between arm circumference (AC) and the prevalence of gallstone disease (GS) across various demographic and clinical subgroups (Table 5). Stratified by age, the strongest association was observed in participants aged 20–39 years (OR: 1.11, 95% CI: 1.08–1.14), with the association attenuating in older age groups, particularly among those aged 60–80 years (OR: 1.05, 95% CI: 1.03–1.08; P for interaction = 0.006). When stratified by gender, the association was more pronounced in females (OR: 1.10, 95% CI: 1.08–1.11) compared to males (OR: 1.06, 95% CI: 1.02–1.09; P for interaction = 0.001).
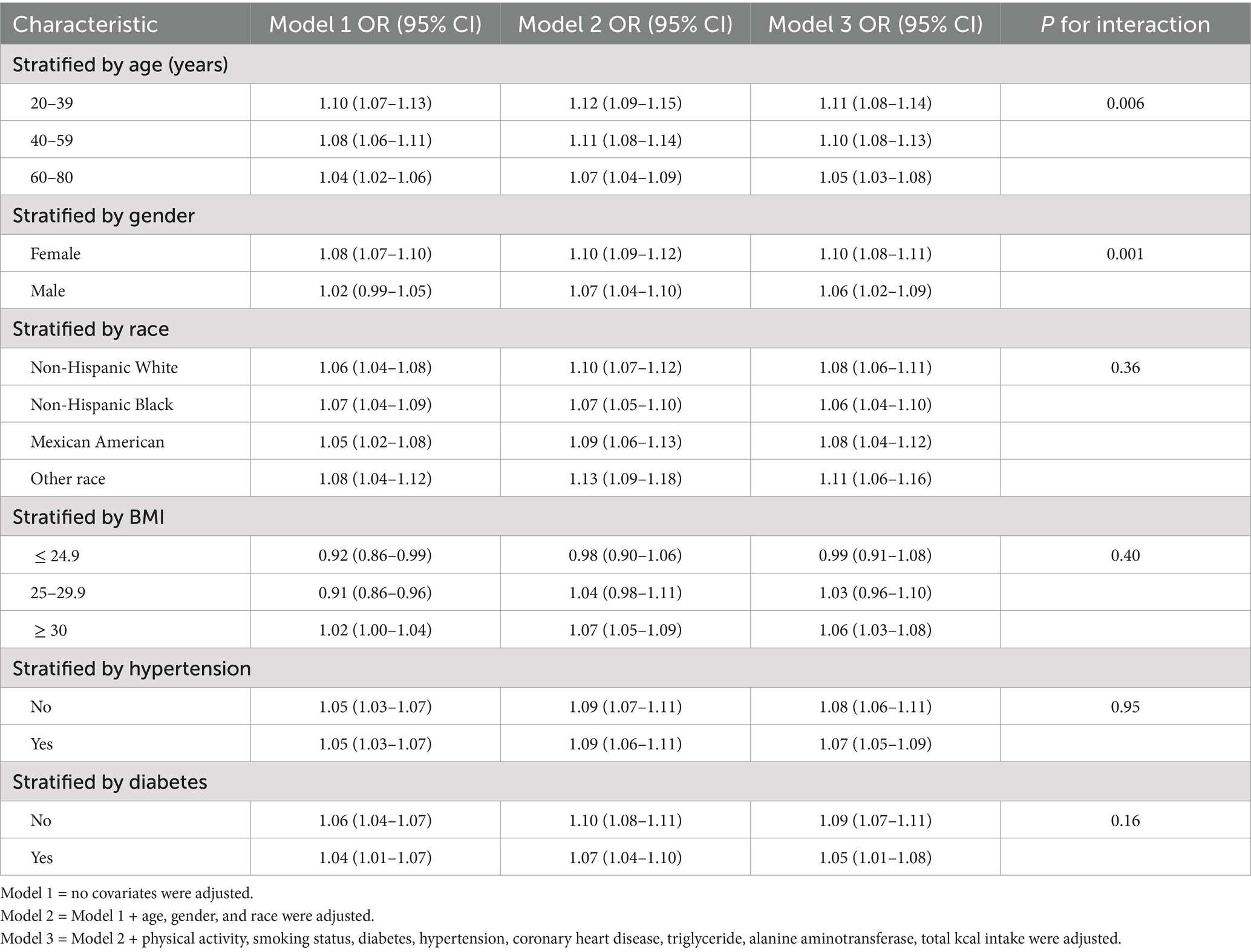
Table 5. Subgroup analysis between AC with gallstone disease prevalence.
The association remained statistically significant across all racial groups, with the highest odds observed in the “Other Race” category (OR: 1.11, 95% CI: 1.06–1.16), followed by Non-Hispanic Whites (OR: 1.08, 95% CI: 1.06–1.11; P for interaction = 0.36). When stratified by BMI, the relationship was strongest in participants with a BMI ≥30 (OR: 1.06, 95% CI: 1.03–1.08), while it was not statistically significant in those with a BMI ≤24.9 (OR: 0.99, 95% CI: 0.91–1.08; P for interaction = 0.40). Furthermore, the association persisted regardless of hypertension status, with comparable odds ratios in hypertensive (OR: 1.07, 95% CI: 1.05–1.09) and non-hypertensive participants (OR: 1.08, 95% CI: 1.06–1.11; P for interaction = 0.95). Stratification by diabetes status revealed a stronger association in participants without diabetes (OR: 1.09, 95% CI: 1.07–1.11) compared to those with diabetes (OR: 1.05, 95% CI: 1.01–1.08; P for interaction = 0.16).
In summary, the positive association between AC and GS prevalence was consistent across most subgroups, with stronger associations observed in younger participants, females, and those with higher BMI.
4 DiscussionThis study is the first to comprehensively examine the relationship between AC and GS prevalence. We found a linear positive correlation between AC and GS prevalence, with an 8% increase in the prevalence of GS for every 1 cm increase in AC. After categorizing AC into tertiles, we observed a 2.43-fold increase in GS prevalence among individuals in the highest AC tertile than in those in the lowest AC tertile. The results of the subgroup analyses further indicated that AC showed a positive association with GS prevalence across nearly all populations, with only slight variations. Our results confirm the importance of AC as a predictor of the risk of developing GS.
While our findings are novel, it is essential to position AC within the broader context of established indicators of obesity, such as BMI and WC, which are well-recognized predictors of MetS and GS. BMI is the most commonly used measure of overall adiposity, while WC serves as a strong indicator of visceral fat accumulation, which is closely linked to metabolic abnormalities. In contrast, AC is a simple, practical, and noninvasive measure that simultaneously reflects body composition (including muscle and fat mass) and nutritional status. Importantly, our study demonstrated that the association between AC and GS prevalence remained significant even after adjusting for BMI, WC, and other metabolic confounders. This finding suggests that AC provides complementary information beyond BMI and WC, particularly in populations where assessing WC or BMI is not feasible or practical.
GS is prevalent globally, especially in developed countries, with 1.5 million people seeking medical care for GS in the US in 2015 alone (21). The pathogenesis of GS is complex and involves several factors. Earlier studies have indicated a higher prevalence of GS in females compared to males (22, 23), which may be because of estrogen-induced increase in the synthesis and secretion of hepatic cholesterol by increasing the expression of estrogen receptor 1 and G protein-coupled receptor 30 as well as decreased bile salt synthesis, and ultimately promoting GS development (24). Moreover, estrogen weakens the contractility of the gallbladder and prolongs the retention time of bile, thereby increasing the deposition of cholesterol crystals (24). Similarly, we found a higher prevalence of GS in females than in males. Advanced age is considered an important factor in the increased prevalence of GS (25, 26). Similarly, our study found that the mean age of individuals without GS was 50 years (ranging from 35 to 63), while for those with GS, it was 60 years (ranging from 46 to 71). With increasing age, the composition of bile changes, and the amount of cholesterol in bile may increase, whereas the amount of bile acid salts may decrease, leading to an increased risk of cholesterol crystal formation and, consequently, an increased incidence of GS (27).
Moreover, the motor function of the gallbladder may weaken, leading to a longer bile retention time, which increases the risk of developing GS (28, 29). However, recent studies have highlighted that metabolic factors, such as obesity and diabetes, significantly influence the prevalence of GS, particularly among younger populations (30, 31). Genetic factors are also important risk factors for GS, with its prevalence varying according to race. In developed countries, the prevalence of GS is significantly higher in white populations than in black populations (28). For example, an epidemiological survey found that, in the US, the prevalence of GS was 16.6% among white women compared with 13.9% among black women and 8.6% among white men, compared with 5.3% among black men (32). This may be related to the differences in dietary habits, lifestyles, and healthcare among the different races. For example, white populations have greater access to high-calorie food, which may have contributed to a higher prevalence of GS. Similarly, our study found that the prevalence of GS is highest among non-Hispanic white people compared with other populations.
Recently, a growing body of research has identified a strong correlation between the rising incidence of GS and the high prevalence of MetS (26, 33, 34). Among them, IR is a key mechanism underlying the increased incidence of GS. In hepatocytes, IR promotes cholesterol secretion by causing abnormal expression of the transcription factor forkhead box protein O1 through the action of ABCG5 and ABCG8 (35), which may explain the higher prevalence of GS among individuals with diabetes. The prevalence of GS was also higher among individuals with obesity than among those without obesity (26). The main reason for this is obesity-induced metabolic changes, such as increased bile secretion from the liver, hyperlipidemia, reduced intestinal motility, and dysfunctions in various metabolic organs, including the liver and gallbladder (36). Further, our study revealed that the mean BMI of participants in the GS group was higher than that of those in the non-GS group [31.8 (27.7–37.7) vs. 28.5 (24.6–33.3), p < 0.001]. Notably, the prevalence of GS is increasing among the younger population due to the increased intake of high-calorie foods as society develops, and economic standards increase, as well as increased physical inactivity (37).
AC is a simple and noninvasive measure of great value for evaluating the nutritional status of the body and the risk of disease development. The connection between AC, MetS, and related diseases has been thoroughly investigated (23, 26, 33, 38–40). In a cross-sectional study including 2,397 patients, Wang et al. discovered a positive association between AC and both hepatic steatosis and fibrosis and that this positive association was consistent across sex and race (Mexican Americans, other Hispanics, non-Hispanic white people, Black population, Asians, and other races) (41). Xiao et al. investigated the relationship between AC and both all-cause and cardiovascular-related mortality in patients with diabetes (20). They identified a significant negative correlation between AC and both all-cause and cardiovascular-related mortality in this population (20). In a study by Chao et al. that included 11,527 participants, AC showed a significant positive association with HOMA-IR, an indicator of IR (42).
As mentioned previously, the pathogenesis of GS is closely related to metabolic abnormalities. However, the relationship between the AC and GS has not yet been effectively explored. In this study, we examined the association between AC and GS prevalence. We discovered that AC showed a linear positive correlation with the prevalence of GS and that this relationship was maintained across different subgroups, although there were subtle differences. Our findings offer new insights into the potential utility of AC in evaluating adult health.
Our study has several strengths. First, this study is the first to clarify the relationship between AC and GS prevalence. Second, NHANES provided a representative sample of US participants who followed a meticulously designed study protocol and underwent stringent quality control and assurance, thereby ensuring the reliability of our conclusions. Third, the comprehensive demographic and metabolic data, along with detailed follow-up information, enabled us to account for potential confounders. Finally, we also performed subgroup analyses to ensure the generalizability of our results to a wider population.
Nevertheless, our study has certain limitations. First, as this was a cross-sectional study, we were unable to establish a causal relationship between AC and GS. While causal inference methods, such as propensity score matching or instrumental variable analysis, could strengthen causal interpretations, the nature of our study and data limitations restricted their application. Nonetheless, sensitivity analyses demonstrated consistent results, underscoring the robustness of our findings. Future longitudinal or Mendelian randomization studies are warranted to explore causal relationships further. Second, GS was diagnosed based on a questionnaire survey, which might have been influenced by recall bias. Third, owing to the design of the NHANES, we could only measure AC at a single time point at baseline; however, AC may change over time. Finally, although we adjusted for many possible confounders, we could not eliminate the potential impact of unmeasured confounders.
Despite these limitations, our study provides new insights into the relationship between AC and GS prevalence. Compared with BMI and WC, AC represents a practical and complementary indicator that may help assess GS risk, particularly in resource-limited or large-scale screening settings. In the future, we plan to conduct prospective cohort studies to evaluate the longitudinal relationship between AC and GS incidence, as well as comparative analyses to explore the relative predictive value of AC, WC, and BMI in identifying individuals at high risk of GS. These efforts will further clarify the utility of AC in metabolic and gallstone disease management.
5 ConclusionOur study is the first to uncover the link between AC and GS prevalence. Specifically, there was a linear positive correlation between AC and GS prevalence, with GS prevalence increasing by 8% for each 1 cm rise in AC. While we could not establish a causal relationship between AC and GS prevalence, the result remains noteworthy.
Data availability statementThe original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
Author contributionsJW: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing. XC: Conceptualization, Data curation, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing. WH: Conceptualization, Formal analysis, Methodology, Project administration, Resources, Writing – original draft, Writing – review & editing. XZ: Data curation, Formal analysis, Investigation, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing. PY: Formal analysis, Investigation, Methodology, Project administration, Resources, Validation, Writing – original draft, Writing – review & editing. JG: Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. DW: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Writing – original draft, Writing – review & editing.
FundingThe author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by National Natural Science Foundation of China (NSFC) (Grant no. 82400758), NHC Key Laboratory of Nuclear Technology Medical Transformation (Mianyang Central Hospital) (Grant no. 2023HYX032), Health Commission of Sichuan Province Medical Science and Technology Program (Grant no. 24QNMP028), and Medical Research Youth Innovation Project of Sichuan Province, China (Grant no. Q23046).
AcknowledgmentsWe are appreciative of the NHANES participants and staff. We thank all reviewers who participated in the review.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statementThe authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
AbbreviationsGS, gallstone disease; AC, arm circumference; US, United States; MetS, metabolic syndrome; IR, insulin resistance; NAFLD, non-alcoholic fatty liver disease; NHANES, National Health and Nutrition Examination Survey; BMI, body mass index; CHD, coronary heart disease; AST, aspartate aminotransferase; HbA1c, hemoglobin A1c.
Footnotes References1. Wang, X, Yu, W, Jiang, G, Li, H, Li, S, Xie, L, et al. Global epidemiology of gallstones in the 21st century: a systematic review and Meta-analysis. Clin Gastroenterol Hepatol. (2024) 22:1586–95. doi: 10.1016/j.cgh.2024.01.051
PubMed Abstract | Crossref Full Text | Google Scholar
2. Rodriguez Gatta, D, Huidobro, L, Petermann-Rocha, F, Van de Wyngard, V, Godoy, F, Cid, V, et al. Sex disparities in gallstone disease: insights from the MAUCO prospective population-based cohort study. BMJ Open Gastroenterol. (2024) 11:e001457. doi: 10.1136/bmjgast-2024-001457
PubMed Abstract | Crossref Full Text | Google Scholar
3. Wu, W, Pei, Y, Wang, J, Liang, Q, and Chen, W. Association between visceral lipid accumulation indicators and gallstones: a cross-sectional study based on NHANES 2017-2020. Lipids Health Dis. (2024) 23:345. doi: 10.1186/s12944-024-02319-2
PubMed Abstract | Crossref Full Text | Google Scholar
4. Sandler, RS, Everhart, JE, Donowitz, M, Adams, E, Cronin, K, Goodman, C, et al. The burden of selected digestive diseases in the United States. Gastroenterology. (2002) 122:1500–11. doi: 10.1053/gast.2002.32978
PubMed Abstract | Crossref Full Text | Google Scholar
5. Stevens, N, Saroya, GA, Elian, A, and Shebrain, S. Gender variations in 30-day outcomes following cholecystectomy in patients with biliary acute pancreatitis. Am J Surg. (2024) 241:116034. doi: 10.1016/j.amjsurg.2024.116034
PubMed Abstract | Crossref Full Text | Google Scholar
6. Fugazzola, P, Podda, M, Tian, BW, Cobianchi, L, Ansaloni, L, and Catena, F. Clinical update on acute cholecystitis and biliary pancreatitis: between certainties and grey areas. EClinicalMedicine. (2024) 77:102880. doi: 10.1016/j.eclinm.2024.102880
PubMed Abstract | Crossref Full Text | Google Scholar
7. Shinsugi, C, Gunasekara, D, and Takimoto, H. Use of mid-upper arm circumference (MUAC) to predict malnutrition among Sri Lankan schoolchildren. Nutrients. (2020) 12:168. doi: 10.3390/nu12010168
PubMed Abstract | Crossref Full Text | Google Scholar
8. Chand, S, and Shah, D. Mid upper arm circumference for detection of severe acute malnutrition in infants aged between one and six months. Indian Pediatr. (2015) 52:528–32. doi: 10.1007/s13312-015-0671-5
PubMed Abstract | Crossref Full Text | Google Scholar
9. Rieckmann, A, Fisker, AB, Øland, CB, Nielsen, S, Wibaek, R, Sørensen, TB, et al. Understanding the child mortality decline in Guinea-Bissau: the role of population-level nutritional status measured by mid-upper arm circumference. Int J Epidemiol. (2022) 51:1522–32. doi: 10.1093/ije/dyac113
PubMed Abstract | Crossref Full Text | Google Scholar
10. Mramba, L, Ngari, M, Mwangome, M, Muchai, L, Bauni, E, Walker, AS, et al. A growth reference for mid upper arm circumference for age among school age children and adolescents, and validation for mortality: growth curve construction and longitudinal cohort study. BMJ. (2017) 358:j3423. doi: 10.1136/bmj.j3423
PubMed Abstract | Crossref Full Text | Google Scholar
11. Saueressig, C, Luft, VC, and Dall'Alba, V. Measurement of mid-arm circumference as a starting point for nutritional assessment of patients with decompensated cirrhosis: a prospective cohort study. J Hum Nutr Diet. (2023) 36:116–25. doi: 10.1111/jhn.13067
PubMed Abstract | Crossref Full Text | Google Scholar
12. Kamiya, K, Masuda, T, Matsue, Y, Inomata, T, Hamazaki, N, Matsuzawa, R, et al. Complementary role of arm circumference to body mass index in risk stratification in heart failure. JACC Heart Fail. (2016) 4:265–73. doi: 10.1016/j.jchf.2015.11.010
PubMed Abstract | Crossref Full Text | Google Scholar
13. Duong, TV, Wu, PY, Wong, TC, Chen, HH, Chen, TH, Hsu, YH, et al. Mid-arm circumference, body fat, nutritional and inflammatory biomarkers, blood glucose, dialysis adequacy influence all-cause mortality in hemodialysis patients: a prospective cohort study. Medicine. (2019) 98:e14930. doi: 10.1097/MD.0000000000014930
PubMed Abstract | Crossref Full Text | Google Scholar
14. Schaap, LA, Quirke, T, Wijnhoven, HAH, and Visser, M. Changes in body mass index and mid-upper arm circumference in relation to all-cause mortality in older adults. Clin Nutr. (2018) 37:2252–9. doi: 10.1016/j.clnu.2017.11.004
PubMed Abstract | Crossref Full Text | Google Scholar
15. Wijnhoven, HA, van Bokhorst-de van der Schueren, MA, Heymans, MW, de Vet, HC, Kruizenga, HM, Twisk, JW, et al. Low mid-upper arm circumference, calf circumference, and body mass index and mortality in older persons. J Gerontol A Biol Sci Med Sci. (2010) 65:1107–14. doi: 10.1093/gerona/glq100
PubMed Abstract | Crossref Full Text | Google Scholar
16. Shi, J, Yang, Z, Niu, Y, Zhang, W, Li, X, Zhang, H, et al. Large mid-upper arm circumference is associated with metabolic syndrome in middle-aged and elderly individuals: a community-based study. BMC Endocr Disord. (2020) 20:78. doi: 10.1186/s12902-020-00559-8
PubMed Abstract | Crossref Full Text | Google Scholar
17. Zhu, Y, Lin, Q, Zhang, Y, Deng, H, Hu, X, Yang, X, et al. Mid-upper arm circumference as a simple tool for identifying central obesity and insulin resistance in type 2 diabetes. PLoS One. (2020) 15:e0231308. doi: 10.1371/journal.pone.0231308
PubMed Abstract | Crossref Full Text | Google Scholar
19. Gómez-García, A, Nieto-Alcantar, E, Gómez-Alonso, C, Figueroa-Nuñez, B, and Alvarez-Aguilar, C. Parámetros antropométricos como predictores de resistencia a la insulina en adultos con sobrepeso y obesidad [Anthropometric parameters as predictors of insulin resistance in overweight and obese adults]. Aten Primaria. (2010) 42:364–71. doi: 10.1016/j.aprim.2009.10.015
PubMed Abstract | Crossref Full Text | Google Scholar
20. Xiao, X, Yu, X, Zhu, H, Zhai, X, Li, S, Ma, W, et al. Arm circumference, arm-to-waist ratio in relation to cardiovascular and all-cause mortality among patients with diabetes mellitus. Nutrients. (2023) 15:961. doi: 10.3390/nu15040961
PubMed Abstract | Crossref Full Text | Google Scholar
21. Peery, AF, Crockett, SD, Murphy, CC, Jensen, ET, Kim, HP, Egberg, MD, et al. Burden and cost of gastrointestinal, liver, and pancreatic diseases in the United States: update 2021. Gastroenterology. (2022) 162:621–44. doi: 10.1053/j.gastro.2021.10.017
PubMed Abstract | Crossref Full Text | Google Scholar
22. Fujita, N, Yasuda, I, Endo, I, Isayama, H, Iwashita, T, Ueki, T, et al. Evidence-based clinical practice guidelines for cholelithiasis 2021. J Gastroenterol. (2023) 58:801–33. doi: 10.1007/s00535-023-02014-6
PubMed Abstract | Crossref Full Text | Google Scholar
23. Zhu, Q, Xing, Y, Fu, Y, Chen, X, Guan, L, Liao, F, et al. Causal association between metabolic syndrome and cholelithiasis: a Mendelian randomization study. Front Endocrinol. (2023) 14:1180903. doi: 10.3389/fendo.2023.1180903
PubMed Abstract | Crossref Full Text | Google Scholar
24. de Bari, O, Wang, TY, Liu, M, Portincasa, P, and Wang, DQ. Estrogen induces two distinct cholesterol crystallization pathways by activating ERα and GPR30 in female mice. J Lipid Res. (2015) 56:1691–700. doi: 10.1194/jlr.M059121
PubMed Abstract | Crossref Full Text | Google Scholar
25. Sogabe, M, Okahisa, T, Kagawa, M, Sei, M, Kagemoto, K, Tanaka, H, et al. Association of metabolic dysfunction-associated fatty liver disease with gallstone development: a longitudinal study. J Gastroenterol Hepatol. (2024) 39:754–61. doi: 10.1111/jgh.16483
PubMed Abstract | Crossref Full Text | Google Scholar
26. Ke, B, Sun, Y, Dai, X, Gui, Y, and Chen, S. Relationship between weight-adjusted waist circumference index and prevalence of gallstones in U.S. adults: a study based on the NHANES 2017-2020. Front Endocrinol. (2023) 14:1276465. doi: 10.3389/fendo.2023.1276465
Crossref Full Text | Google Scholar
27. Misciagna, G, Leoci, C, Guerra, V, Chiloiro, M, Elba, S, Petruzzi, J, et al. Epidemiology of cholelithiasis in southern Italy. Part II: risk factors. Eur J Gastroenterol Hepatol. (1996) 8:585–94. doi: 10.1097/00042737-199606000-00017
PubMed Abstract | Crossref Full Text | Google Scholar
28. Li, YT, Shao, WQ, Chen, ZM, Ma, XC, Yi, CH, Tao, BR, et al. GOLM1 promotes cholesterol gallstone formation via ABCG5-mediated cholesterol efflux in MASH livers. Clin Mol Hepatol. (2024) 10:657. doi: 10.3350/cmh.2024.0657
留言 (0)