
記住我
Uterine torsion, which is defined as a rotation of >45° around the long axis, is a rare obstetric complication in humans that can lead to severe complications if ignored. Twin pregnancy, with simultaneous pregnancy in each uterus and a complete bicorporeal uterus, is another rare and complex clinical situation. To date, most studies in the literature have been case reports of single pregnancies, and we present a case of gravid uterus torsion in a complete bicorporeal uterus with a twin pregnancy during the third trimester.
2. Patient and case presentationA 33-year-old para-2 mother was hospitalised at 33 weeks of gestation because of a threatened premature delivery. The patient had a complete bicorporeal uterus. She had a healthy full-term baby through an uncomplicated lower right uterine segment caesarean section prior to this pregnancy. The patient conceived spontaneously. Two foetuses from a twin pregnancy (cephalic position and transverse lie) were discovered in the bilateral uterine cavities. She had no significant disease history and denied a history of smoking.
The patient's vital signs were stable at admission. She denied vaginal bleeding and described normal foetal movement before presentation, except for irregular uterine contractions. Laboratory examination showed normal results, and the patient suddenly experienced dizziness and fatigue after rolling over. Physical examination revealed hypotension (blood pressure, 81/55 mmHg) and tenderness in the right lower abdomen. The foetal heart rate (left/right) was 130/60 beats per minute. An emergency caesarean section was rapidly performed under spinal anaesthesia due to maternal shock and foetal bradycardia. We considered placental abruption or uterine rupture as a preoperative diagnosis, and no imaging examination was performed due to the urgency of the event. The abdomen was opened using a Pfannenstiel incision. After opening the peritoneum, we examined one uterus and did a caesarean section on its lower part. The first neonate was delivered without difficulty, with an Apgar score of 10 points (1/5/10 min). The other uterus was congested, and the peritoneum of the uterus and bladder were invisible. No obvious rupture of the uterus or difficult exposure of the ipsilateral fallopian tube and ovary were observed during exploration. An engorged venous plexus crossing the anterior operating field was observed. Another neonate was delivered with an Apgar score of 10 (1/5/10 min). Due to the urgency of the situation, it took only 21 min from the discovery of the abnormality to the delivery of the foetus by caesarean section.
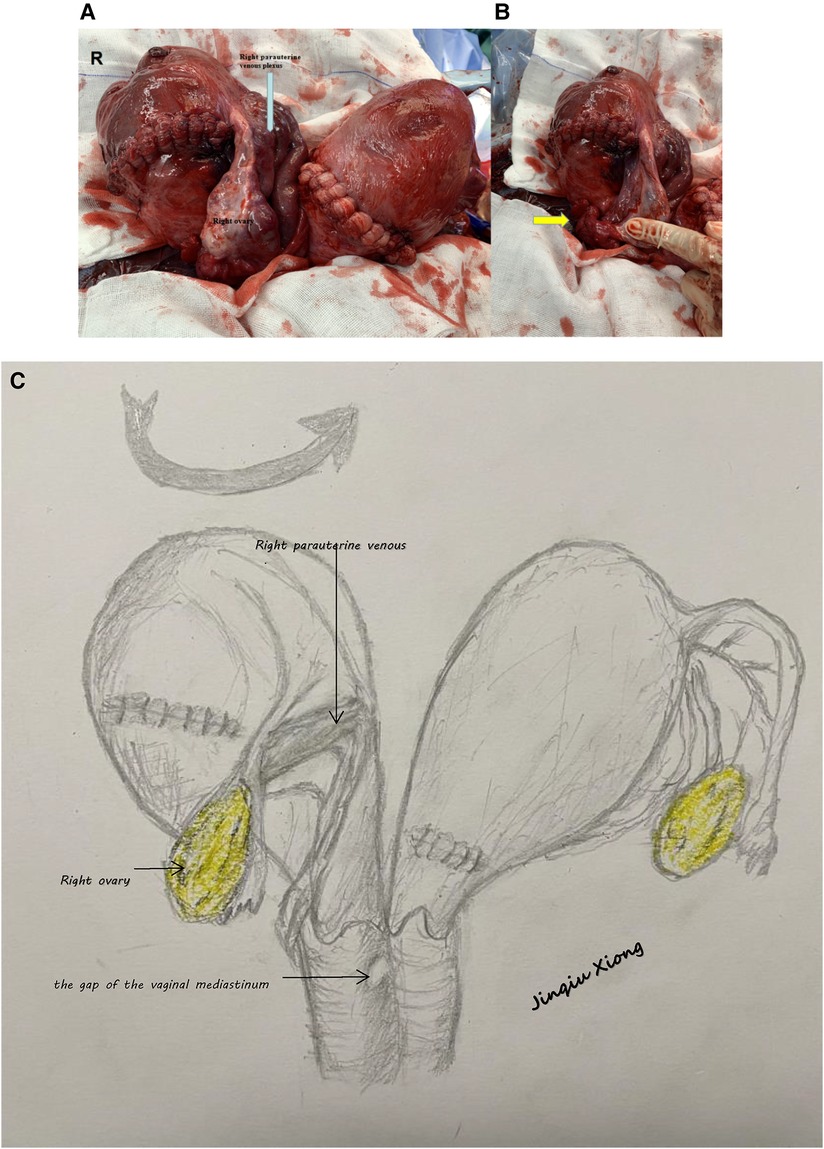
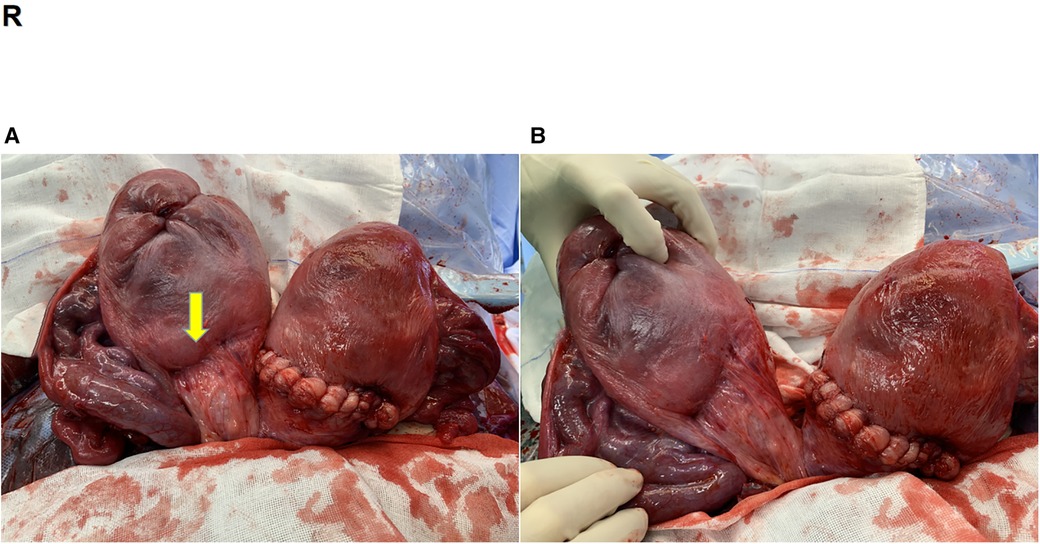
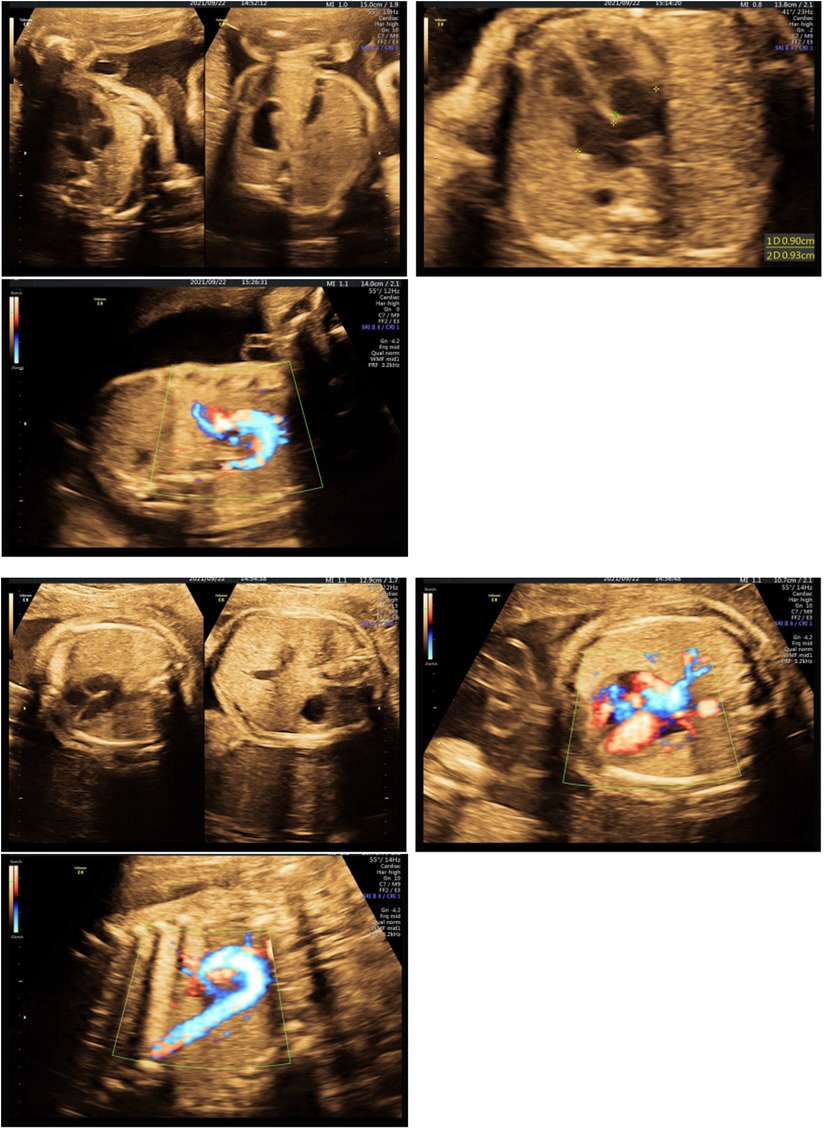
After the newborns and placentas were delivered, the right uterus was rotated 180° anticlockwise at the junction of the cervix and uterine corpus along the long axis of the uterus. This caused hyperaemia and distension of the parauterine venous plexus (Figure 1). The rotation was corrected manually without difficulty, and we performed a posterior transverse caesarean delivery (Figure 2). The colour of the uterine muscle layer rapidly returned to normal after restoration, and no signs of placental abruption were observed. During the postoperative physical examination, we discovered the vaginal mediastinum and double cervix, and the gap of the mediastinum, which was 2 cm away from the cervix, connected the two vaginas, which were classified as a complete bicorporeal uterus, a double “normal” cervix, and a longitudinal non-obstructing vaginal septum (U3b/C2/V1) according to the European Society of Human Reproduction and Embryology and the European Society for Gynaecological Endoscopy Classification (1), and was classified as uterus didelphys with a complete longitudinal vaginal septum according to the American Society for Reproductive Medicine 2021 classification (2). The estimated blood loss volume was 600 ml. Oxytocin and prophylactic antibiotic were administered. Low-molecular-weight heparin was administered postoperatively to prevent thrombosis due to preoperative uterine ischaemia and reperfusion. The patient recovered well and was discharged on the fifth postoperative day. Doppler echocardiography of the two foetuses was normal (Figure 3). Two neonates underwent Doppler echocardiography after birth, and one had patent ductus arteriosus and patent foramen ovale. Two neonates were followed up, and so far, they have been in good condition.
Figure 1. (A) Uterus after foetal delivery (Uterus exteriorized intraoperatively). (B) Torsion of the cervix and uterine body (arrow; the peritoneum of the uterus and bladder was invisible). (C) Schematic figure of uterine torsion.
Figure 2. (A) Uterus after restoration (arrow; previous surgical scar in the lower right uterine segment). (B) Biuterine malformation.
Figure 3. Doppler echocardiography of two fetuses.
3. DiscussionThe enlarged uterine body is usually dextral (<45°) during pregnancy due to the presence of the rectum sigmoid colon, which is a physiological change. Females with congenital uterine anomalies may be at increased risk of spontaneous abortion, premature birth, foetal growth restriction, foetal malpresentation, and abnormal placental insertion (3, 4). The aetiology of uterine torsion is unknown, but the uterus can twist because of hysteromyoma (5, 6), uterine malformation (7), external cephalic version (8, 9), pelvic malformation, loosely suspended uterus, malpresentation (10), pelvic adhesions, which may cause placental abruption, placental perfusion insufficiency (11), foetal distress (8), foetal death (12), intrauterine growth restriction (13), maternal shock, and other fatal complications. However, few cases have occurred without discernible causes (14). Symptoms of uterine torsion vary depending on the degree and duration of torsion. Due to its rarity and atypical clinical symptoms, uterine torsion is usually an acute abdominal condition that is difficult to diagnose preoperatively. Only rare asymptomatic cases during pregnancy have been diagnosed intraoperatively (15). Lower abdominal pain was the most common symptom. By comparing placental location, ultrasonography can aid in diagnosis. Differential diagnoses include placental abruption, uterine rupture, premature labour, appendicitis, acute pyelonephritis, urinary obstruction, hematoma of the broad ligament of the uterus, etc.
Congenital malformations of the female genital tract are common benign conditions that are associated with reproductive problems depending on the type and degree of anatomical distortion, and in our case, when there is an abnormal foetal presentation and uterine malformation exists, sudden postural change may be the precipitating factor.We have used the CARE criteria (https://www.care-statement.org/checklist) to describe the case report. We have submitted as many details about the patient as possible in the hopes of providing some instructive information. Unfortunately, no image of a patient's gynaecological examination or cadiotocography registration of the foetal heart is available.
Obstetricians should be aware of this complication to avoid a delayed diagnosis of uterine torsion. Prompt surgical treatment should be performed to avoid a hysterectomy for uterine necrosis. During the surgery, there could be serious damage to the blood vessels and tissues around the uterus because of an unclear surgical field, and the difficulties in exposing the uterine body should be considered.
Data availability statementThe original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statementWritten informed consent was obtained from the patient for the publication of images or data included in this article.
Author contributionsJX: conceived the idea and critically revised the manuscript. QG: interpreted the data and wrote the manuscript. YZ: provided patient data and contributed to the manuscript. All authors contributed to the article and approved the submitted version.
AcknowledgmentsWe are grateful to Xuwen Yang and Lingfeng Lu for supporting this work.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References1. Grimbizis GF, Gordts S, Di Spiezio Sardo A, Brucker S, De Angelis C, Gergolet M, et al. The ESHRE/ESGE consensus on the classification of female genital tract congenital anomalies. Hum Reprod. (2013) 28:2032–44. doi: 10.1093/humrep/det098
PubMed Abstract | CrossRef Full Text | Google Scholar
2. Pfeifer SM, Attaran M, Goldstein J, Lindheim SR, Petrozza JC, Rackow BW, et al. ASRM Müllerian anomalies classification 2021. Fertil Steril. (2021) 116:1238–52. doi: 10.1016/j.fertnstert.2021.09.025
PubMed Abstract | CrossRef Full Text | Google Scholar
3. Rich DA, Stokes IM. Uterine torsion due to a fibroid, emergency myomectomy and transverse upper segment caesarean section. BJOG. (2002) 109:105–6. doi: 10.1111/j.1471-0528.2002.t01-1-01067.x
PubMed Abstract | CrossRef Full Text | Google Scholar
4. Vaz SA, Dotters-Katz SK, Kuller JA. Diagnosis and management of congenital uterine anomalies in pregnancy. Obstet Gynecol Surv. (2017) 72:194–201. doi: 10.1097/OGX.0000000000000408
PubMed Abstract | CrossRef Full Text | Google Scholar
5. Akhtar MA, Saravelos SH, Li TC, Jayaprakasan K, on behalf of the Royal College of Obstetricians and Gynaecologists. Reproductive implications and management of congenital uterine anomalies: scientific impact paper no. 62 November 2019. BJOG. (2020) 127:e1–e13. doi: 10.1111/1471-0528.15968
PubMed Abstract | CrossRef Full Text | Google Scholar
6. Jeong YY, Kang HK, Park JG, Choi HS. CT features of uterine torsion. Eur Radiol. (2003) 13(Suppl 6):L249–50. doi: 10.1007/s00330-003-1838-3
CrossRef Full Text | Google Scholar
7. Demaria F, Goffinet F, Jouannic JM, Cabrol D. Preterm torsion of a gravid uterus didelphys horn of a twin pregnancy. Obstet Gynecol. (2005) 106:1186–7. doi: 10.1097/01.AOG.0000160477.02248.55
PubMed Abstract | CrossRef Full Text | Google Scholar
8. Salani R, Theiler RN, Lindsay M. Uterine torsion and fetal bradycardia associated with external cephalic version. Obstet Gynecol. (2006) 108:820–2. doi: 10.1097/01.AOG.0000215997.13103.f2
PubMed Abstract | CrossRef Full Text | Google Scholar
9. Karavani G, Picard R, Elami-Suzin M, Mankuta D. Complete uterine torsion diagnosed during an elective caesarean section following failed external cephalic version: a case report. J Obstet Gynaecol. (2017) 37:673–4. doi: 10.1080/01443615.2017.1285874
PubMed Abstract | CrossRef Full Text | Google Scholar
12. Cook KE, Jenkins SM. Pathologic uterine torsion associated with placental abruption, maternal shock, and intrauterine fetal demise. Am J Obstet Gynecol. (2005) 192:2082–3. doi: 10.1016/j.ajog.2004.09.003
PubMed Abstract | CrossRef Full Text | Google Scholar
13. Rood K, Markham KB. Torsion of a term gravid uterus: a possible cause of intrauterine growth restriction and abnormal umbilical artery Doppler findings. J Ultrasound Med. (2014) 33:1873–5. doi: 10.7863/ultra.33.10.1873
PubMed Abstract | CrossRef Full Text | Google Scholar
14. Farhadifar F, Nikkhoo B, Shahgheibi S, Soofizadeh N, Rezaie M. Asymptomatic uterine torsion in a pregnant woman. Indian J Surg. (2014) 76:321–2. doi: 10.1007/s12262-013-0981-6
PubMed Abstract | CrossRef Full Text | Google Scholar
15. Carrier M, Korb D, Morin C, Sibony O. Asymptomatic uterine torsion diagnosed after two uneventful pregnancies. J Gynecol Obstet Hum Reprod. (2018) 47:583–5. doi: 10.1016/j.jogoh.2018.09.004
留言 (0)