
記住我

National and international clinical guidelines agree that total mesorectal excisions (TMEs) should be the oncological standard in rectal cancer surgery. TMEs are associated with pelvic autonomic nerve preservation, which prevents urogenital and ano-(neo-)rectal dysfunction.1–3 However, approximately one third of TMEs are associated with surgically induced postoperative neurogenic urinary dysfunction, and sexual and ano-(neo-)rectal dysfunction occurs even more frequently. Thus, nerve damage during surgery is a well-recognized risk factor.4 Thanks to advances in minimally invasive surgery and the prioritization of functionality and quality of life (QoL) in oncology, colorectal surgeons are increasingly motivated to recognize the complexity and vulnerability of pelvic autonomic neuroanatomy and neurophysiology. Although monitoring TMEs for oncological quality has been standardized, a corresponding standard for preventing nerve damage is lacking.
From the surgeon’s perspective, nerve identification can be difficult, and nerve fibers and plexuses that appear morphologically intact are not always functional. In 2009, a European consensus group (European Society of Medical Oncology, European Society of Surgical Oncology, and European Society of Therapeutic Radiation Oncology) proposed a potential solution to these difficulties: use of a nerve-stimulating device to facilitate nerve sparing during TME.5
Primary prevention of postoperative dysfunction is a main aim of neuromonitoring. A loss of neurosignaling could trigger a timely change in surgical strategy, potentially yielding a better functional outcome. For example, detecting the loss of neurosignaling could prompt correction of the dissection plane, judicious use of energy devices (and possibly an intermittent change to cold scissors), shifting of the surgical objective to selective (palliative) nerve sparing, or insertion of a suprapubic urinary catheter. Before the consensus group proposal, the results of initial, nonrandomized studies had suggested the utility of a neuromonitoring system during open TMEs in offering objective confirmation.6–8
Subsequent advances and exploration led to the development of an accurate, 2-dimensional, pelvic intraoperative neuromonitoring (pIONM) system. Prospective comparative long-term studies,9–11 studies with other designs,12–14 and a recent systematic review and meta-analysis15 showed that pIONM was functionally advantageous in patients with rectal cancer who required electrophysiologically controlled nerve-sparing operations. However, despite promising data, these pIONM studies suffered the limitation of nonrandomized, single-institution designs. A randomized trial was needed to overcome this limitation and a selection bias effect that could not be ruled out.4,15–17 Moreover, because few professionals may be familiar with the pIONM method, a higher level of evidence is certainly important to promote adoption of pIONM technology.
We conducted the multicenter, randomized NEUROmonitoring System (NEUROS) trial to evaluate the safety and efficacy of 2-dimensional pIONM for improving the functional outcome of TME in patients with rectal cancer. Here, we present the 12-month follow-up patient-reported outcomes of urogenital and ano-(neo-)rectal function.
METHODS DesignNEUROS was a 2-arm, randomized, controlled, national multicenter clinical trial with a parallel group and superiority design. It was conducted in 8 centers, all certified as colorectal cancer centers by the German Cancer Society. Before trial initiation, all centers received pIONM training, with technical and clinical support, including pIONM workshops, proctored initiations of pIONM experience, on-site user training, and case visits/observations. The previously published study protocol,18 all amendments, and all other relevant documents were approved by the Ethics Committee of the Rhineland-Palatinate and the individual ethics committees of other participating centers. The trial was conducted according to the ethical principles of the Declaration of Helsinki and the principles of Good Clinical Practice. The trial was supervised by an independent data monitoring committee and is registered at ClinicalTrials.gov (NCT01585727).
PatientsEligible patients (ages 18–90 years) with histologically confirmed rectal cancer were scheduled to undergo a TME. All patients provided written informed consent before inclusion. Trial exclusion criteria were as follows: an emergency operation, presence of a pacemaker, a multivisceral resection, a partial mesorectal excision, missing preoperative data on urogenital or anorectal function, or a severe, untreated physical or mental impairment.
Randomization and MaskingWe used a central web-based randomization method to assign patients in a 1:1 ratio to the pIONM and control groups. The groups were stratified by neoadjuvant therapy and patient sex, with blocks of variable length. All patients and statisticians were blinded to group assignments.
ProceduresIn patients who underwent neoadjuvant therapy, prescreening was scheduled 1 to 21 days before therapy. Preoperative screening (baseline) was scheduled for all patients at 1 to 14 days before the TME. The TMEs were performed by members of a group of 20 skilled surgeons. The frequency and scope of the follow-up visits are shown in Figure 1.
 FIGURE 1:
FIGURE 1: Postoperative follow-up visits and intervention scheme for patients who underwent TME for rectal cancer. FSFI indicates Female Sexual Function Index; IIEF, International Index of Erectile Function; IPSS, International Prostate Symptom Score; NT, neoadjuvant therapy; QoL, quality of life due to urinary symptoms; SC, stoma closure; WS, Wexner Score. †In patients who did not undergo stoma closure, study follow-up visits were planned for 6 and 12 months after the TME. These patients were not assessed for IIEF/FSFI or WS.
Pelvic autonomic nerves were monitored with a Conformité Européenne–certified device (Inomed Medizintechnik GmbH, Emmendingen, Germany; Fig. 2). The colorectal surgeon performed pIONM with a hand-held bipolar microfork probe to identify and verify functional nerve integrity. With this approach, neurostimulation occurs under the continuous electromyographic observation of the internal anal sphincter with simultaneous manometry of the urinary bladder. The monitoring takes place bilaterally within the scope of 4 defined surgical steps (Fig. 3).
 FIGURE 2:
FIGURE 2: pIONM system. The system is semiautomated with system-wide online signal processing and artefact suppression. Changes in acoustic and visual signals were based on reference and threshold values. Nerve stimulation was performed (1–25 mA, 30 Hz, monophasic rectangular pulses, with a 200 μs pulse duration, a 3–10 seconds stimulation period, and 3–10 seconds resting intervals between stimulations), while simultaneously observing (left) electromyography (EMG) of the internal anal sphincter and (right) manometry of the urinary bladder.
 FIGURE 3:
FIGURE 3: pIONM: defined surgical steps during TME (shown for unilateral left only).
The initial stimulations were performed during posterior/posterolateral mesorectal dissection, to detect the pelvic splanchnic nerves. These neurostimulations were limited to 5 stimulations per side. During lateral dissection, neuromapping along the pelvic sidewall was performed to identify other potential nervous tissue exposure (eg, the pelvic splanchnic nerves, S2–S4, or the inferior hypogastric plexus). When anterolateral mesorectal dissection was performed, the extrinsic autonomic nerve supply of the internal anal sphincter was also neuromapped. After the specimen was resected, autonomic innervation was verified with bilateral neuromapping again. This last mapping step was limited to 5 stimulations per side. Spot checks on the quality of the signal analysis were advocated and conducted regularly.
OutcomesThe primary endpoint of urinary function deterioration was defined as at least a 5-point increase at 12 postoperative months in the total International Prostate Symptom Score over the preoperative score. The cutoff was based on long-term results that correlated with deteriorations in QoL because of urinary symptoms.18 In patients who received postoperative urologic treatment for newly developed urinary dysfunction, the primary endpoint was at least a 5-point increase in the pretreatment score compared with the preoperative score. Higher scores indicated deteriorations in urinary function and QoL.
Secondary endpoints were as follows: reduced Female Sexual Function Index by ≥8 points or International Index of Erectile Function by ≥15 points, and a change in fecal incontinence as evaluated by the Wexner score at 12 postoperative months compared with preoperative scores. To assess safety, particularly oncologic safety and adverse events, we evaluated the tumor distance from the circumferential resection margin (CRM) (CRM involvement was defined as a CRM ≤1 mm) and TME quality (grade I: complete; grade II: nearly complete; grade III: incomplete).
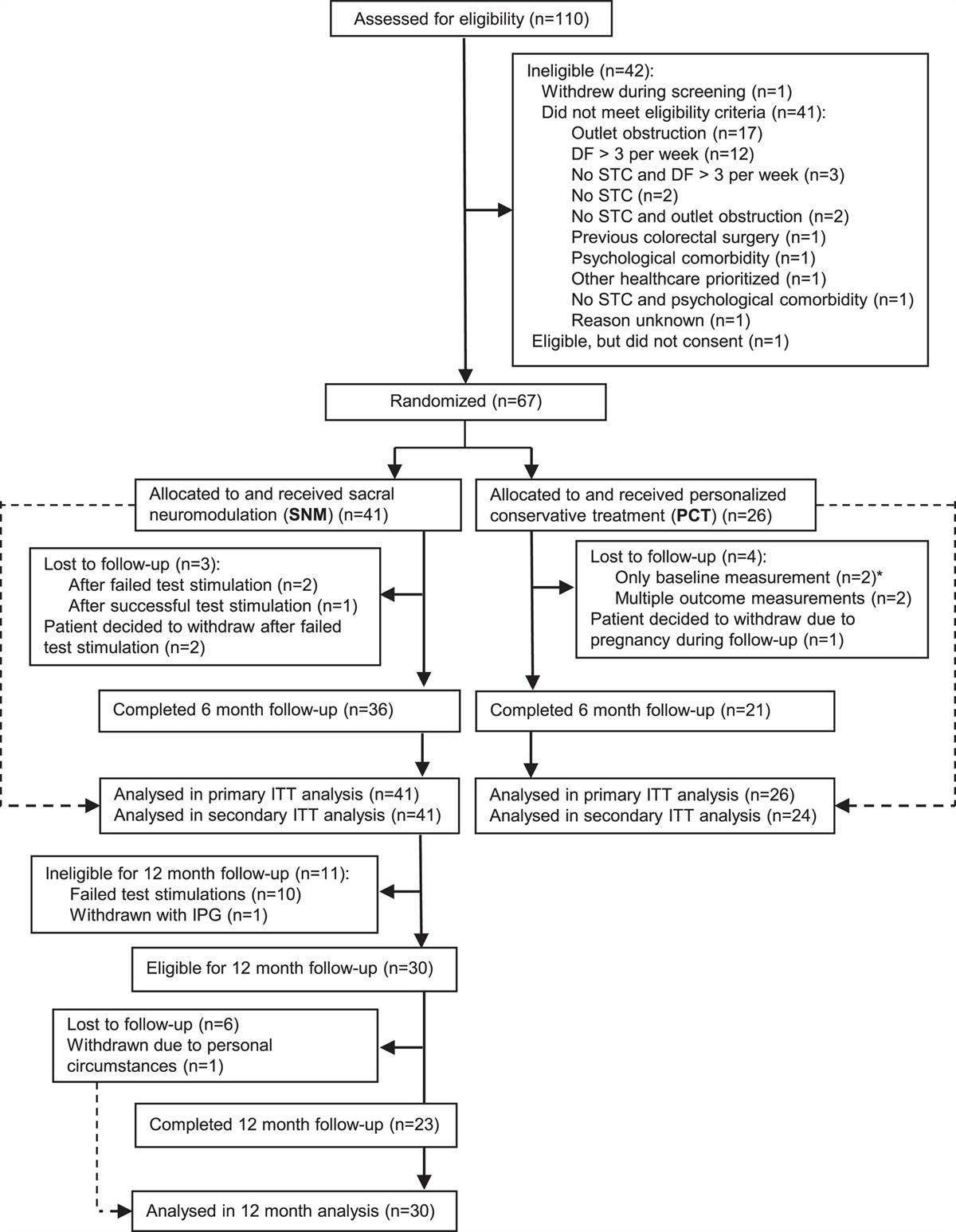
Statistical analysisA power analysis was performed to estimate the sample size. We assumed that deteriorated urinary function would occur in 10% of patients undergoing TME with pIONM and 30% undergoing it without pIONM. In total, 164 study patients would be needed to demonstrate a significant difference between study arms with a power of 90%, based on the Fisher exact test (α=0.05, 2-sided) and an overall dropout rate of 12% (perioperatively: 2%; follow-up period, in both study arms: 10%). Therefore, we enrolled 189 patients in the trial, and data for 171 were analyzed (Fig. 4) according to a modified intention-to-treat protocol.
 FIGURE 4:
FIGURE 4: Patient allocation and analysis. IPSS indicates International Prostate Symptom Score; mITT, modified intention-to-treat.
We constructed a logistic regression model with the following fixed factors: intervention group, patient sex, and existing neoadjuvant therapy. Missing values were replaced with the last observation carried forward. When data were missing on International Prostate Symptom Score status before initiating bladder therapy, these values were replaced with the last postoperative score value recorded before bladder therapy. Treatment effects were expressed as odds ratios and 95% confidence intervals. To test sensitivity, the analysis was repeated with the observed values. Analysis of secondary parameters was considered exploratory, and groups were compared with descriptive methods and exploratory P values (Wilcoxon or Mann-Whitney U test for continuous variables, and χ2 test for dichotomous variables). All analyses were performed with SAS, version 9.4.
RESULTSOf 171 patients included in the modified intention-to-treat analysis, 82 were in the pIONM group and 89 in the control group. The treatment groups were well balanced in baseline demographic and clinical characteristics (Supplemental Digital Content Table 1, https://links.lww.com/SLA/E199). Among 171 patients, 162 (94.7%) had a normal general physical examination and physical condition findings. Fifteen patients in each group had stage IV disease. The procedures included minimally invasive surgery (n=145; 84.8%), low anterior resection (n=163; 95.3%), and abdominoperineal excision (n=8; 4 patients per group). Complete pelvic autonomic nerve preservation was achieved in 74 (43%) patients, with similar rates between groups (P=0.117).
Functional Outcome at BaselineThe average International Prostate Symptom Score was 4.0 (SD: 4.5) in both groups (Table 1). The mean±SD International Index of Erectile Function and its abridged 5-item version, and Female Sexual Function Index, were evenly distributed between groups. Preoperatively, 57% of women had sexual dysfunction and 69% of men had erectile dysfunction, with no differences between groups. The control group had a significantly worse baseline Wexner score than the pIONM group.
TABLE 1 - Baseline Functional Performance of Patients With Rectal Cancer Variables Total (n=171) TME With pIONM (n=82) TME Without pIONM (n=89) P IPSS [mean (SD)] 4.0 (4.5) 4.0 (4.6) 4.0 (4.5) 0.933 Missing data (n) 0 0 0 IIEF [mean (SD)] 39.8 (24.9) 44.5 (25.3) 35.6 (23.9) 0.064 Missing data (n) 16 7 9 IIEF-5 [mean (SD)] 12.2 (9.6) 13.9 (9.7) 10.8 (9.2) 0.065 Missing data (n) 9 3 6 Erectile dysfunction* [n/N (%)] 67/97 (69.1) 28/46 (61) 39/51 (76) 0.223 FSFI [mean (SD)] 21.7 (9.7) 22.2 (9.7) 21.2 (10.4) 0.842 Missing data (n) 11 6 5 Sexual dysfunction† [n/N (%)] 31/54 (57.4) 16/27 (59) 15/27 (56) 0.900 Wexner score [mean (SD)] 2.7 (4.0) 2.1 (3.1) 3.3 (4.7) 0.049 Missing data (n) 7 3 4*Erectile dysfunction=IIEF-5 score <21 points.
†Sexual dysfunction=FSFI score <26.6 points.
FSFI indicates Female Sexual Function Index; IIEF, International Index of Erectile Function; IIEF-5, International Index of Erectile Function, 5-item version; IPSS, International Prostate Symptom Score.
The groups had similar micturition-related QoL, residual urinary volumes, medications for urinary incontinence, and anal sphincter resting tone and squeeze tone. The same number of patients in the pIONM and control groups took constipating medication or required incontinence pads. No differences were observed with regard to urge symptoms, stool frequency, fragmentation, or nocturnal incontinence (Supplemental Digital Content Tables 2, https://links.lww.com/SLA/E200, 3, https://links.lww.com/SLA/E201).
Key Primary OutcomeA logistic regression analysis showed that urinary function deteriorated more frequently in the control group than in the pIONM group (odds ratio: 0.342; 95% confidence interval, 0.124–0.944; P=0.038; Fig. 5). However, no significant effects were detected for patient sex (odds ratio: 0.417; 0.147–1.184; P=0.100), neoadjuvant therapy (odds ratio: 1.464; 0.573–3.741; P=0.426), or baseline International Prostate Symptom Score (odds ratio: 0.852; 0.717–1.012; P=0.067).
 FIGURE 5:
FIGURE 5: Proportions of patients with urinary function deterioration at 12 months after TME surgery. Urinary function deterioration was defined as at least a 5-point increase in the IPSS. pIONM group (black), control group (gray). IPSS indicates International Prostate Symptom Score.
Key Secondary OutcomesCompared with the preoperative International Index of Erectile Function, the 12-month postsurgery score decreased by at least 15 points in 20/65 (31%) male patients. This result was independent of the intervention (10/33 in the pIONM group vs 10/32 of control patients; odds ratio: 0.515; 0.151–1.763; P=0.291) and neoadjuvant therapy (odds ratio: 1.204; 0.380–3.823; P=0.752). Logistic regression analysis showed a significant influence of baseline sexual function on this effect (odds ratio: 1.044; 1.014–1.076; P=0.005).
Compared with the preoperative Female Sexual Function Index, the 12-month postsurgery score was reduced by at least 8 points in 11/37 (30%) patients. This result was independent of the intervention (3/18 of pIONM patients vs 8/19 of control patients; odds ratio: 0.166; 0.025–1.096; P=0.062) and neoadjuvant therapy (odds ratio: 0.486; 0.076–3.106; P=0.446). Logistic regression analysis showed that the baseline Female Sexual Function Index score significantly influenced this effect (odds ratio: 1.235; 1.026–1.486; P=0.026).
During the 12-month observation period, postoperative fecal incontinence was significantly worse in the control group than in the pIONM group (Table 2). This difference manifested in the smaller absolute change in Wexner score versus baseline in the pIONM group (3.6±5.2) compared with the control group (5.5±5.3, P=0.044).
TABLE 2 - Patient Functional Performance at 12 Months After TME Surgery for Rectal Cancer Variables Total (n=171) TME With pIONM (n=82) TME Without pIONM (n=89) P IPSS [mean (SD)]* 4.2 (4.2) 3.8 (4.3) 4.5 (4.2) 0.230 Missing data (n) 21 8 13 IIEF [mean (SD)]† 32.5 (23.3) 40.3 (25.0) 25.0 (19.1) 0.012 Missing data (n) 34 14 20 IIEF-5 [mean (SD)]† 9.9 (9.2) 12.1 (10.0) 7.7 (7.8) 0.074 Missing data (n) 29 11 18 Erectile dysfunction‡ [n/N (%)] 61/86 (70.9) 26/42 (62) 35/44 (80) 0.072 FSFI [mean (SD)] 18.0 (11.1) 20.3 (11.1) 15.6 (10.8) 0.199 Missing data (n) 25 13 12 Sexual dysfunction§ [n/N (%)] 26/48 (54) 10/25 (40) 16/23 (70) 0.040 Wexner score [mean (SD)] 6.7 (5.2) 5.5 (4.5) 7.9 (5.6) 0.011 Missing data (n) 31 15 16*Without Last-Observation-Carried-Forward.
†Patients without stoma.
‡Erectile dysfunction=IIEF-5 score <21 points.
§Sexual dysfunction=FSFI score <26.6 points.
FSFI indicates Female Sexual Function Index; IIEF-5, International Index of Erectile Function, 5-item version; IPSS, International Prostate Symptom Score.
At 12 months postsurgery, global International Prostate Symptom Score values were similar between groups (Table 2). The pIONM group had a considerably more favorable mean International Index of Erectile Function than the control group, consistent with higher scores on the 5-item version and a lower proportion of patients with erectile dysfunction. A total of 9% took drugs concomitantly for urological conditions, as did 6% for erectile dysfunction, with no significant difference between groups. Among females, severe postoperative sexual dysfunction (Female Sexual Function Index <26.55 points) was significantly less common in the pIONM group than in the control group. However, the mean Female Sexual Function Index did not differ significantly between the groups at 12 months postsurgery.
Five patients in each group needed long-term catheterization. In the pIONM group, 46% needed continence pads, compared with 63% in the control group (P=0.049). A significantly smaller proportion of patients in the pIONM group reported a feeling of fragmented emptying (56% of pIONM patients vs 75% in the control group; Supplemental Digital Content Tables 4, https://links.lww.com/SLA/E202, 5, https://links.lww.com/SLA/E203).
Safety OutcomesThe measures of oncologic safety are presented in the supplement (Supplemental Digital Content Table 1, https://links.lww.com/SLA/E199). We observed no differences between groups in tumor perforations, TME specimen quality, CRM status, or lymph node yield. Rates of anastomotic leakage (6/155; 3.9%) and the need for reoperation (6/171; 5.6%) did not differ significantly between the groups. No patient died within 30 days after surgery. In the safety population (ie, as treated), serious adverse events occurred in 36/88 (41%) patients in the pIONM group and 53/99 (54%) patients in the control groups. The investigators and the data safety monitoring board judged that none of the serious adverse events were related to the pIONM procedure. No device-related errors were observed.
DISCUSSIONThis NEUROS trial was the first prospective randomized multicenter study to address electrophysiologically controlled nerve sparing in rectal cancer surgery. Significantly fewer patients who had TME with pIONM versus without it (8% vs 19%) experienced marked urinary function deterioration at 1 year postsurgery. This result confirms the general findings in previous case-control (7% vs 40%) and prospective long-term studies (20% vs 51). It also is consistent with the results of a meta-analysis and confirms surgery without pIONM as an independent risk factor for urinary function decline.9,10,15 In their study of 189 patients with rectal cancer who underwent exclusively laparoscopic rectal excisions, Fang et al12 observed a significantly reduced rate of urinary disorders (7% vs 18%) when the procedure included 1-dimensional pIONM (cystomanometry, n=71). Similarly, pIONM was associated with a significantly reduced mean International Prostate Symptom Score after a short-term follow-up. In other studies that compared preoperative and 12-month postoperative International Prostate Symptom Scores, laparoscopic TMEs performed with pIONM (n=45 with bilateral and n=13 with unilateral 1-dimensional pIONM with electromyography) yielded significantly better results than TMEs performed without pIONM (n=29).14
In addition to confirming our primary hypothesis, our findings indicate that electrophysiologically controlled nerve sparing also appears to be advantageous in terms of fecal incontinence at 1 year postsurgery. This result is consistent with those of comparative studies showing significantly lower rates of newly developed fecal incontinence in the pIONM group at the short-term (7% vs 40%) and long-term follow-ups (21% vs 50%).9,11 In contrast, a previous retrospective study showed no significant difference in Wexner score at 12-month follow-up assessments between patients treated with versus without electromyography-based pIONM (n=50 and n=23, respectively). Although those authors attributed the discrepancy to small sample sizes, locally advanced tumors, and preexisting disorders, they found a trend toward higher Wexner score values when pIONM was not used.14
The NEUROS trial results also reveal that fragmented defecation occurred less frequently in the pIONM group compared with the control group (56% vs 75%). This interesting result suggests that another quite bothersome symptom of low anterior rectal resection syndrome, known as clustering, could be prevented with pIONM.
Exploratory analyses of the secondary outcomes showed that sexual function tended to be maintained in the pIONM group. At 1 year postoperatively, the pIONM group had a significantly higher mean International Index of Erectile Function in men and significantly lower severely impaired sexual function rate (Female Sexual Function Index <26.6 points) in women, compared with corresponding values in the control group. These results were consistent with the results of Fang et al, who reported that in 119 male patients, the non-pIONM group (n=74) presented with lower International Index of Erectile Function scores (5-item version) than the pIONM group (n=45) at 6 months postoperatively (13.6±2.0 vs 15.4±1.9; P<0.001).12 The mean baseline scores (5-item version) in our cohort (10.8±9.2 and 13.9±9.7) were significantly less favorable than the mean baseline scores in their cohort (20.3±1.3 and 20.4±1.3), which justified their significance level. Another study showed that at 1 year postsurgery, erectile dysfunction occurred less frequently among 35 male patients in the pIONM arm compared with 18 patients in the no-pIONM arm (14% vs 28%). Similarly, Female Sexual Function Index values in 34 patients indicated that severe sexual function impairment occurred more frequently in the no-pIONM arm.14 We confirmed these trends in both the 5-item version of the International Index of Erectile Function and Female Sexual Function Index. However, in our cohort, the differences between treatment groups did not reach statistical significance, particularly when Female Sexual Function Index and International Index of Erectile Function required changes of at least 8 and 15 points, respectively.
The discrepancies among these studies might be explained by findings from the ROLARR trial, which confirmed that sexual function impairments at baseline significantly influenced postoperative International Index of Erectile Function and Female Sexual Function Index scores.19 In the present trial, 57% of female and 69% of male patients were affected by sexual and erectile dysfunction at baseline, respectively. Thus, an adjusted sample size with lower baseline dysfunction rates would be necessary to confirm that pIONM could serve as a predictive factor for sexual function.
In our safety evaluation, no unanticipated events occurred during or after the electrophysiologically controlled nerve-sparing procedure. Moreover, pIONM did not compromise TME quality. The observed serious adverse events were not related to pIONM, and the duration of surgery was not significantly extended because of pIONM. Our mean time expenditure of 24 minutes was similar to that reported by others for open and laparoscopic TMEs.12,13
In addition to variations in surgery, there may have been variations in anesthesia and the pIONM procedure. For example, the lateral and anterolateral stimulation frequencies were not restricted. However, in this NEUROS trial, the translational, iteratively developed, 2-dimensional pIONM system was used in a standardized manner by well-trained teams.
Alternatives to pIONM were not considered because intrarectal manometry20 was impractical and penile tumescence evaluation, measured with a strain-gauge transducer, cannot be performed in women and did not appear to be sufficiently accurate in rectal surgery.6,7 Impedance measurement in target muscles seems suitable, at least, but needs further investigation in clinical studies.21
The pIONM system we used had overall accuracies of 88% and 90% for predicting sexual function in open and laparoscopic TME surgery, respectively. The pIONM device showed even higher accuracy in predicting postoperative urinary and ano-(neo-) rectal function.22
Evaluations of secondary endpoints in 2 previous randomized trials (COLOR II and ROLARR) suggested that expert surgeons are accomplished in autonomic nerve preservation. However, estimations of the completeness of nerve preservation during TMEs ranged from 21% to 98% in previous studies,19,22–25 compared with 43% in the present study. This broad variation could result in part from differences in the perception of risk of nerve damage.22 Moreover, the causes of neurogenic and non-neurogenic functional disorders after a TME can be multifactorial. For example, postoperative functional disorders after minimally invasive TMEs can arise from heat damage to the pelvic nerves.26 To date, no randomized controlled trial has evaluated the effects of thermal spread on nerve preservation in TME surgery. Of note, in this NEUROS trial, different energy devices were used in 84.2% of TMEs. However, the surgical approaches (open, laparoscopic, or robotic), dissection techniques, and blood loss volumes did not differ significantly between the 2 trial arms. These surgical factors should be considered in future prospective clinical studies. Indeed, patient-reported outcomes alone are unsuitable for routine quality assurance of pelvic autonomic nerve preservation, and pIONM may be useful for advancing the knowledge of these gray areas.
Because IONM is demanding27 and the accuracy of a robotics-assisted anterolateral mesorectal dissection is variable, the factors that neurosurgeons consider also are of interest to the pelvic surgeon. The training or expertise needed to perform pIONM must be investigated to determine whether pIONM requires the supervision of a clinical neurophysiologist, only automated machines, or simply a technician. Currently, neuromonitoring during robotics-assisted TMEs is considered safe. However, further improvements in display quality, connectivity, and system integration are expected.28,29
The NEUROS trial was distinguished by our choice of the most widely used validated scores in colorectal surgery for evaluating patient-reported functional outcomes.30 A bias toward either group was unlikely because randomization was stratified according to patient sex and neoadjuvant chemoradiation therapy. Furthermore, we assessed preoperative function.
This study had some limitations. First, because the German guidelines changed, the surgical approach had to be altered during the study period,3 and all participating centers changed the standard approach to minimally invasive access. However, all surgical approaches were equally distributed between the groups (Supplemental Digital Content Table 1, https://links.lww.com/SLA/E199). Second, although tumor height was evenly distributed between groups, many tumors were located in the lower third of the rectum, which increases the risks of micturition disorders, nerve damage, or both; however, these risks were not considered in our analyses. Third, as with any intraoperative technology, neuromonitoring may fail because of inherent limitations (surgeon inexperience with pIONM, technical failures). However, at the study onset, the surgeons in one participating center were highly experienced in the method, and they assisted with training surgeons in the other centers. Moreover, subgroup analyses showed that the primary endpoints were not affected by center experience, tumor height (<6 cm from the anocutaneus line), or changes in the minimally invasive surgical approach.
In summary, this NEUROS trial showed that pIONM during TME in patients with rectal cancer reduced the probability of a marked deterioration in urinary function at 1 year postsurgery, compared with TME without pIONM. In addition, the slightly lower rates of both sexual dysfunction and some symptoms of low anterior rectal resection syndrome in the pIONM group, compared with the control group, could be attributed to the controlled nerve sparing. Based on our findings that pIONM was safe in terms of serious adverse events and provided good oncological specimen quality, we suggest that pIONM could serve as a tool for facilitating nerve-sparing in TME surgery. Future research should focus on assessing the nerve-sparing potential of different dissection techniques and the efficacy of early targeted therapy in well-selected, optimally powered patient populations, with the aim of further reducing pelvic vegetative dysfunction.
ACKNOWLEDGMENTSThe authors gratefully acknowledge the members of the NEUROS study group for their continuous effort and study support: Yasmin Isenbruck-Wenk and Karen Stumm (Department of General, Visceral, and Transplant Surgery, University Medical Center of the Johannes Gutenberg-University Mainz, Mainz, Germany), and Daniel Wachtlin, Julia Wosniok, Anja Powaska, Rebecca Jathe, Michaela Schmittbetz, and Lukas Schollenberger (Interdisciplinary Center for Clinical Trials, University Medical Center Mainz, Mainz, Germany). They also are thankful to the investigators, research staff, and study nurses at all participating centers involved in patient care, for their outstanding engagement. The authors also thank the members of the Independent Data Monitoring Committee (Prof. Ferdinand Köckerling, MD, Berlin, Germany, and Prof. Felix Aigner, MD, Graz, Austria). Thanks also are due to the IKONA project consortium (BMBF FKZ 01EZ0726) and the autoPIN project consortium (BMBF FKZ 13GW0022C), who stood at the forefront of pIONM technology development and provided helpful support for the NEUROS study.
REFERENCES 1. Heald RJ, Husband EM, Ryall RD. The mesorectum in rectal cancer surgery-the clue to pelvic recurrence? Br J Surg. 1982;69:613–616. 2. Bregni G, Akin Telli T, et al. Grey areas and evidence gaps in the management of rectal cancer as revealed by comparing recommendations from clinical guidelines. Cancer Treat Rev. 2020;82:1019–1030. 3. German Cancer Society, German Cancer Aid, AWMF. Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF): S3-Leitlinie Kolorektales Karzinom, Langversion 2.1,2019, AWMF Registrierungsnummer: 021/007OL. Available at: http://www.leitlinienprogramm-onkologie.de/leitlinien/kolorektales-karzinom/. Accessed February 15, 2021. 4. Nocera F, Angehrn F, von Flüe M, et al. Optimising functional outcomes in rectal cancer surgery. Langenbecks Arch Surg. 2021;406:233–250. 5. Valentini V, Aristei C, Glimelius B, et al. Multidisciplinary Rectal Cancer Management: 2nd European Rectal Cancer Consensus Conference (EURECA-CC2). Radiother Oncol. 2009;92:148–163. 6. Hanna NN, Guillem J, Dosoretz S, et al. Intraoperative parasympathetic nerve stimulation with tumescence monitoring during total mesorectal excision for rectal cancer. J Am Coll Surg. 2002;195:506–512. 7. da Silva GM, Zmora O, Börjesson L, et al. The efficacy of a nerve stimulator (CaverMap) to enhance autonomic nerve identification and confirm nerve preservation during total mesorectal excision. Dis Colon Rectum. 2004;47:2032–2038. 8. Kneist W, Heintz A, Junginger T. Intraoperative identification and neurophysiologic parameters to verify pelvic autonomic nerve function during total mesorectal excision for rectal cancer. J Am Coll Surg. 2004;198:59–66. 9. Kneist W, Kauff DW, Juhre V, et al. Is intraoperative neuromonitoring associated with better functional outcome in patients undergoing open TME? Results of a case-control study. Eur J Surg Oncol. 2013;39:994–999. 10. Kauff DW, Lang H, Kneist W. Risk factor analysis for newly developed urogenital dysfunction after total mesorectal excision and impact of pelvic intraoperative neuromonitoring—a prospective 2-year follow-up study. J Gastrointest Surg. 2017;21:1038–1047. 11. Kauff DW, Roth YDS, Bettzieche RS, et al. Fecal incontinence after total mesorectal excision for rectal cancer-impact of potential risk factors and pelvic intraoperative neuromonitoring. World J Surg Oncol. 2020;18:12. 12. Fang JF, Wei B, Zheng ZH, et al. Effect of intra-operative autonomic nerve stimulation on pelvic nerve preservation during radical laparoscopic proctectomy. Colorectal Dis. 2015;17:O268–O276. 13. Wałęga P, Romaniszyn M, Wałęga M, et al. Intraoperative neuromonitoring of hypogastric plexus branches during surgery for rectal cancer - preliminary report. Pol Przegl Chir. 2017;89:69–72. 14. Zhou MW, Huang XY, Chen ZY, et al. Intraoperative monitoring of pelvic autonomic nerves during laparoscopic low anterior resection of rectal cancer. Cancer Manag Res. 2018;11:411–417. 15. Samara AA, Baloyiannis I, Perivoliotis K, et al. Intraoperative neuromonitoring in rectal cancer surgery: a systematic review and meta-analysis. Int J Colorectal Dis. 2021;36:1385–1394. 16. Sedrakyan A, Campbell B, Merino JG, et al. IDEAL-D: a rational framework for evaluating and regulating the use of medical devices. BMJ. 2016;353:i2372. 17. Haim N, Wexner SD. Rectal cancer-associated urinary dysfunction: a review. Curr Bladder Dysfunct Rep. 2015;10:118–124. 18. Kauff DW, Kronfeld K, Gorbulev S, et al. Continuous intraoperative monitoring of pelvic autonomic nerves during TME to prevent urogenital and anorectal dysfunction in rectal cancer patients (NEUROS): a randomized controlled trial. BMC Cancer. 2016;16:323. 19. Jayne D, Pigazzi A, Marshall H, et al. Effect of robotic-assisted vs conventional laparoscopic surgery on risk of conversion to open laparotomy among patients undergoing resection for rectal cancer: The ROLARR randomized clinical trial. JAMA. 2017;318:1569–1580. 20. Possover M, Quakernack J, Chiantera V. The LANN technique to reduce postoperative functional morbidity in laparoscopic radical pelvic surgery. J Am Coll Surg. 2005;201:913–917. 21. Schuler R, Goos M, Langer A, et al. A new method of intraoperative pelvic neuromonitoring: a preclinical feasibility study in a porcine model. Sci Rep. 2022;12:3696. 22. Kauff DW, Wachter N, Bettzieche R, et al. Electrophysiology-based quality assurance of nerve-sparing in laparoscopic rectal cancer surgery: Is it worth the effort? Surg Endosc. 2016;30:4525–4532. 23. Lange MM, Martz JE, Ramdeen B, et al. Long-term results of rectal cancer surgery with a systematical operative approach. Ann Surg Oncol. 2013;20:1806–1815. 24. Andersson J, Abis G, Gellerstedt M, et al. Patient-reported genitourinary dysfunction after laparoscopic and open rectal cancer surgery in a randomized trial (COLOR II). Br J Surg. 2014;101:1272–1279.
留言 (0)