
記住我

Geoffrey Dover, PhD, CAT(C), ATC, Tristan Castonguay, MSc, CAT(C), Matylda Lentini, BSc, CAT(C), and Ilana Patlan, BSc
Affiliation: Concordia University, Montreal, Quebec, Canada.
Objective: In the general population, there is evidence that women experience more pain than men, but this has not been fully evaluated in athletes. Therefore, the purpose of our study was to measure the differences in pain and cardiovascular variables between male and female athletes during a painful cold pressor task.
Study Design: Two groups, pre–post test design.
Subjects: Sixty healthy male university athletes (age = 22.9 ± 2.2 years, height = 179.3 ± 9.6 cm, weight = 89.1 ± 12.2 kg) and 60 healthy female university athletes (age = 22.5 ± 2.5 years, height = 164.8 ± 6.7 cm, weight = 64.9 ± 9.2 kg) participated in the study.
Intervention: We used the cold pressor task, which requires the participant to immerse their hand in cold water for 3 minutes to induce pain and to increase blood pressure.
Outcome measures: We measured pressure pain thresholds (PPT) at the upper extremity and lower extremity before and after the cold pressor task. We used the numeric pain rating scale to assess pain, and we measured heart rate, systolic blood pressure, and diastolic blood pressure before, during, and after the cold pressor task.
Results: All participants experienced a significant amount of pain during the cold pressor task. There was no difference in pain during the cold pressor task between the male and female athletes (male = 5.56 ± 2.36, female = 5.7 ± 1.69, P = 0.723). Female athletes had significantly lower upper extremity PPT scores compared with male athletes (females = 70.2 ± 24.7 N and 74.7 ± 24.3 N and males = 97.9 ± 31.6 N and 107.9 ± 35.5 N; all P < 0.001). A similar result was observed for the PPT at the lower extremity. Although there were no significant differences in heart rate before and during the cold pressor task between male athletes (68.6 ± 10.2 bpm and 70.9 ± 10.2 bpm) and female athletes (70.2 ± 8.8 bpm and 72.8 ± 9.8 bpm, P = 0.361 and P = 0.299), there were significant differences in systolic blood pressure before and during the cold pressor task (males = 129.0 ± 11.8 and 143.5 ± 11.6, females = 111.9 ± 9.4 and 129.3 ± 12.4, P < 0.001 for both).
Conclusions: Although male and female athletes experienced a similar amount of pain during the cold pressor task, pain thresholds were significantly lower in female athletes compared with male athletes, which is a separate pain construct. The differences in PPT and systolic blood pressure could indicate that female athletes have a different conditioned pain modulation compared with male athletes.
Acknowledgements: This study was partially funded by the Canadian Athletic Therapists Association.
Follow-up After ACL Reconstruction: How Long is Long Enough?Alexander J. Hoffer, MD,* and Jordan M. Leith, MD†
Affiliations: *Department of Surgery, Faculty of Medicine, University of Western Ontario; and †Department of Orthopaedics, Faculty of Medicine, University of British Columbia.
Objective: To assess the differences in patient-reported outcome measures (PROMs) at 1 year and 2 years after anterior cruciate ligament reconstruction (ACLR) and evaluate the need for follow-up 1 year after the surgery.
Study Design: A retrospective comparison of prospectively collected PROMs.
Subjects: All patients who underwent an ACLR by a single surgeon between 2016 and 2020.
Intervention: Primary ACLR with or without associated meniscal surgery by a single surgeon between 2016 and 2020. Demographics include age, sex, side, and ethnicity.
Outcome Measures: Six externally validated PROMs were collected preoperatively and at 6, standardized, postoperative times. A repeated-measures analysis of PROMs at 1 year and 2-years after the surgery and subgroup analyses based on sex, age, and associated meniscal injury were completed. Differences in PROMs were compared with previously published or calculated minimal clinically important differences for each score.
Results: One-hundred forty-five participants were included in the final analysis. All PROMs except the Veteran's Rand-12 Mental Component showed a statistical improvement at 2 years compared with 1 year after ACLR. However, only the Quality of Life and Sport and Recreation domains of the Knee Injury and Osteoarthritis Outcome Score showed a clinically significant difference at 2 years postoperatively. No major differences were found in the subgroup analyses compared with the entire included sample.
Conclusion: Overall, PROMs exhibit little to no clinically meaningful difference at 2 years compared with 1 year after ACLR. As reinjury generally triggers rereferral, a 2-year follow-up visit has low clinical utility and increases financial and opportunity costs for the patient, physician, and health care system.
Acknowledgements: None.
The impact of 2-hour exertional heat stress on exercise-induced gastrointestinal syndrome and exercise-associated gastrointestinal symptoms in masters versus young adult endurance athletesPascale Young, MDiet,* Ricardo J. S. Costa, PhD,* Rhiannon M. J. Snipe, PhD,† Stephanie K. Gaskell, BHon,* Rebekah Alcock, PhD,‡ Alice Mika, MDiet,* Christopher Rauch, BHon,* and Kayla Henningsen, MDiet*
Affiliation: *Monash University, Melbourne, Victoria, Australia; †Deakin University, Melbourne, Victoria, Australia; and ‡La Trobe University, Bundoora, Victoria, Australia.
Objective: To determine if the impact of exertional heat stress on the gastrointestinal tract varies between masters (≥40 years) and young adult (<30 years) endurance athletes.
Study Design: Cross sectional.
Subjects: Sixteen (male n = 12 and female n = 4) masters [mean (SD): age 43.9 (3.2) years, height 176 (8) cm, body mass (BM) 74.2 (11.6) kg, fat mass 19.2 (6.3)%, V̇O2max 56.3 (6.9) mL/kgBM/min, and weekly training volume 291 (287) min], and 21 (male n = 14 and female n = 7) young adult [age 25.9 (2.3) years, height 177 (7) cm, BM 69.5 (8.4) kg, fat mass 14.6 (4.9)%, V̇O2max 61.0 (7.8) mL/kgBM/min, and weekly training volume 230 (294) min] recreationally trained, nonacclimatized, endurance athletes volunteered to participate.
Intervention: Two hours running at 60% V̇O2max in 35°C ambient conditions and 29% relative humidity.
Outcome Measures: Whole-blood samples were collected before, immediately after, 1 hour after, and 2 hours after exercise and analyzed for markers of exercise-induced gastrointestinal syndrome (EIGS) (plasma concentrations of I-FABP, sCD14, LBP, IgM, and systemic inflammatory cytokines). Thermoregulatory measures (rectal temperature and thermal comfort rating), heart rate (HR), rating of perceived exertion (RPE), and gastrointestinal symptoms (GIS) were recorded every 10 to 20 minutes during exertional heat stress.
Results: Preexercise to postexercise peak magnitude of change in intestinal epithelial integrity markers did not significantly differ (P > 0.05) between masters [mean (95% CI): I-FABP 1632 (959-2304) pg/mL, sCD14 −0.17 (−1.75 to 1.42) µg/mL, LBP −0.68 (−3.54 to 2.19) µg/mL, and IgM −3.71 (−31.1 to 23.7) MMU/mL] and young adult [I-FABP 1378 (815-1940) pg/mL, sCD14 0.59 (0.05-1.13) µg/mL, LBP 1.17 (0.02-2.31) µg/mL, and IgM 38.9 (−2.31 to 80) MMU/mL] endurance athletes. Peak postexercise plasma concentrations of proinflammatory cytokine IL-1β was higher in young adult [3.04 (0.34-5.75) pg/mL, P = 0.030] vs masters [−1.08 (−3.55 to 1.39) pg/mL] endurance athletes. No difference between other systemic inflammatory cytokines was observed (P > 0.05). Severity of GIS during exercise was not different between masters [sum (range): 329 (0-69)] and young adult [608 (0-219)] endurance athletes (P > 0.05), nor were measures of thermoregulatory strain. Young adult endurance athletes presented significantly higher HR (P = 0.019) and RPE (P = 0.030) (165 bpm and 14, respectively) compared with masters (150 bpm and 12, respectively) endurance athletes along the exertional-heat stress.
Conclusions: Pathophysiology of EIGS in response to 2 hours of exertional heat stress is not substantially different in older active adults, with masters endurance athletes responding comparably to young adult endurance athletes. Despite a significant difference in some biomarkers of EIGS, levels remained within reference range and are of no clinical relevance.
Infrared Thermography: A Novel Tool for Monitoring the Healing Process of Fractures—A Systematic ReviewTristan Castonguay, MSc, CAT(C),* and Geoffrey Dover, PhD, CAT(C), ATC*,†
Affiliations: *Department of Health, Kinesiology, and Applied Physiology, Concordia University, Montreal, QC, Canada; and 2CRIR-Lethbridge-Layton-Mackay Rehabilitation Centre, Montreal, QC, Canada.
Objective: This systematic review examined the current evidence using infrared thermography for measuring the change in tissue temperature during the healing process of fractures. The quality of the evidence was evaluated with the purpose of providing recommendations for clinicians when using infrared thermography.
Data Source: We searched 3 databases (Clarivance—Web of Science, Google Scholar and PubMed.gov) for studies comparing medical imaging and infrared thermography during the follow-up period of fractures in the extremities. One researcher conducted the full-text review, and 2 researchers completed the quality assessment of the eligible studies.
Main Results: We identified 3 research studies that met our inclusion criteria. One inclusion criterion that was necessary was evaluating fractures over a follow-up period of minimum 6 weeks using both infrared thermography and another form of imaging. In all 3 studies, researchers used infrared thermography to compare the temperature of the injured limb with the uninjured limb. A total of 61 participants with either forearm or lower-leg fractures were examined. The conclusion of all 3 studies indicated that during the inflammation phase, a 1°C temperature asymmetry is statistically and clinically significant. As the fracture healed during the repair and maturation phase, a decrease in temperature asymmetry was observed in all participants. Resuming training or sport was considered safe when the temperature of the fractured limb was equal to the uninjured side. Finally, all studies were also able to correlate the temperature changes to the healing phases of the fractures.
Conclusions: According to the grading criteria used to evaluate the research articles, the body of evidence supported the use of infrared thermography once a patient was diagnosed with a fracture by traditional medical imaging. Infrared thermography can safely be used to monitor the evolution of a stress fracture. The use of infrared thermography could be useful to determine the state of healing and for a safe return to sport. Infrared thermography is a new technology, and clinicians should understand that more research is needed and that infrared thermography cannot replace traditional diagnostic imaging tools.
Acknowledgements: This systematic review was partially funded by the Canadian Athletic Therapists Association (CATA).
Ask Teachers How—A Decade of Concussion Management Community CollaborationJames Carson, MD,* Alicia Sheng, MD,* Pauline King-Taylor, BPHE, BEd,† Becky Green, MEd,† Stefanie Moser, CAT(C), and Petra Wildgoose, MD*
Affiliations: *Department of Family and Community Medicine, University of Toronto, Toronto, ON, Canada; and †York Region District School Board (retired), Aurora, ON, Canada.
Objective: To share the experiences of one Ontario community's decade long collaboration among educators and health care professionals to optimize students' return to school after a concussion.
Study Design: The key organizers of a secondary school professional development workshop on the optimal return to school after a concussion were interviewed a decade later in a qualitative manner.
Subjects: Ninety-four educators and school support personnel attended the original 2012 concussion management educational workshop.
Intervention: Presurveys and postsurveys were completed by the 2012 participants. Educators were asked for input on how best to accommodate students returning to school after concussion. With the support of a local health professional, the educators' committee then developed the Green Folder tool, which was approved by the school board and implemented within their school in 2015. The Green Folder was taken by the postconcussion student to guidance appointments, to each class, and to medical appointments to facilitate communication, expectations, and accommodations.
Outcome Measures: Key organizers were queried regarding barriers, facilitators, and overall impressions on the development and implementation of the Green Folder.
Results: Some of the biggest challenges included a lack of awareness and stigma regarding concussions among students, teachers, and parents. With ongoing education and teamwork, the tool was very well received and was enabled by open communication among all members of the student's circle of care. They also reflected upon how this collaboration ultimately led to a much larger resource for “return-to-school” postconcussion education and management. This larger resource was developed and released in 2019, and it is known as “SCHOOLFirst” (https://schoolfirstconcussion.ca/).
Conclusions: Concussion advocacy can become richer when key community stakeholders are empowered and engaged by concussion researchers in the health care professions. Our example can be heralded by many other communities in the development of similar programs.
Assessing the Importance of Past Physical Activity in Predicting Current Injury Risk Using Weighted Cumulative Exposure MethodsChinchin Wang, MSc, PhD(c),* Michal Abrahamowicz, PhD,*,† Marie-Eve Beauchamp, PhD,† Russell Steele, PhD,‡ Jay S. Kaufman, PhD,* and Ian Shrier, MD, PhD§
Affiliations: *Department of Epidemiology, Biostatistics and Occupational Health, McGill University, Montreal, QC, Canada; †Centre for Outcomes Research and Evaluation, Research Institute of the McGill University Health Centre, Montreal, QC, Canada; ‡Department of Mathematics and Statistics, McGill University, Montreal, QC, Canada; and §Centre for Clinical Epidemiology, Lady Davis Institute, Jewish General Hospital, McGill University, Montreal, QC, Canada.
Objective: Physical activity–related injury risk among children is affected by current and past activities. Past activity may predispose to injury through tissue damage and insufficient recovery or protect against injury by strengthening tissue with sufficient recovery. It is unclear what the relevant time window and relative importance of past activity are in predicting time to injury. The objectives of this study are to (1) determine the relative importance of activity done in past weeks in predicting current injury risk conditional on activity in the current week in children and (2) identify the time window over which past activity is relevant for predicting current injury risk.
Study Design: Prospective cohort study with weekly follow-up for 5.5 years.
Subjects: One thousand six hundred sixty Danish school children aged 6 to 15 years.
Observation Technique: Parents reported on the number of times their child participated in recreational activity (activity sessions) and whether they experienced pain each week. Participants with pain were followed up by a clinician who diagnosed any injuries.
Outcome Measures: The outcome was time to first clinician-diagnosed injury. Weighted cumulative exposure (WCE) functions were estimated for the association between the number of weekly activity sessions and time to first injury in each school year, conditional on activity in the current week. WCE functions were estimated using different time windows (10, 15, 20, 25 weeks), and the best fitting function was determined using the Akaike Information Criterion. We generated 95% confidence intervals accounting for repeated measures by bootstrap resampling.
Results: The best fitting WCE function included 20 weeks of past activity. Higher levels of activity recorded in the previous 2 to 9 weeks were predictive of increased risk of injury. However, given the same recent activity history, activity done more than 9 weeks earlier appeared protective.
Conclusions: WCE methods provide insight into time-specific associations between activity history and injury. Although higher levels of physical activity done recently may predict injury caused by increased fatigue and tissue damage, those who remain uninjured during this time may be less likely to be injured later on due to beneficial long-term effects of activity such as tissue strengthening.
Acknowledgements: Funding by CIHR.
The Impact of Amino Acid Based Beverage Interventions on Gastrointestinal Status in Response to Exertional-Heat StressRicardo J. S. Costa, PhD,* Kayla Henningsen, MDiet,* Stephanie K. Gaskell, BHon,* Rebekah Alcock, PhD,† Alice Mika, MDiet,* Christopher Rauch, BHon,* Samuel N. Cheuvront, PhD,‡,§ Phil Blazy,‡ and Robert Kenefick, PhD‡
Affiliation: *Monash University, Melbourne, Victoria, Australia; †La Trobe University, Bandoora, Victoria, Australia; ‡Entrinsic Bioscience (EBS), LLC, Norwood, Massachusetts; and §Sports Science Synergy, LLC, Franklin, Massachusetts.
Objective: To determine the effects of 2 differing amino acid (AA) beverage composition interventions on biomarkers of gastrointestinal status in response to exertional heat stress.
Study Design: Counterbalanced, crossover double-blinded RCT.
Subjects: After ethical approval and informed consent, 20, healthy, endurance running–trained nonheat acclimatized or acclimated male participants [mean (SD): age 32 (8) years, height 1.81 (0.05) m, body mass 77.7 (7.4) kg, fat mass 15.1 (5.1)%, and V̇O2max 59.6 (8.1) mL/kg/min] volunteered to participate.
Intervention: One week after the initial assessment, participants were randomly allocated to complete 2 exertional heat stress trials, with at least 1-week washout. Trials included a water control trial (CON) and 1 of the 2 AA beverages developed using EBS HydroActive Technology. On VS001 (4.5 g/L AA) and VS006 (6.4 g/L AA), participants were asked to consume a 237 mL prefabricated beverage with breakfast and dinner for 7 days before the exertional heat stress trial, and every 20 minutes (from 0 minute to 120 minutes) during 2 hours running at 60% V̇O2max in 35°C ambient conditions. CON received water volume equivalent.
Outcome Measures: Whole-blood samples were collected before, immediately after, 1 hour after, and 2 hours after exercise and analyzed for biomarkers of exercise-induced gastrointestinal syndrome (EIGS), including plasma concentrations of I-FABP, sCD14, LBP, IgM by ELISA, and systemic inflammatory cytokines by multiplex techniques. Physiological and thermoregulatory strain markers [i.e., physiological strain index (PSI)] and gastrointestinal symptoms (GIS) were recorded every 20 minutes during exercise.
Results: Overall, average PSI [mean (95% CI): 5.9 (5.0-6.7)] did not differ between the trials (P > 0.05). Preexercise resting biomarker concentrations of gastrointestinal status did not significantly differ between the trials (P > 0.05). Lower preexercise to peak postexercise I-FABP [Δ 249 (60-437) pg/mL, 900 (464-1336) pg/mL, 1485 (1050-1920) pg/mL], sCD14 [Δ −93 (−458 to 272) ng/mL, 12 (−174 to 197) ng/mL, 854 (527-1180) ng/mL], IgM (Δ −6.5 (−23.0 to 9.9) MMU/mL, −10.4 (−16.2 to 4.7) MMU/mL, 8.8 (3.1-14.5) MMU/mL), and systemic inflammatory profile [69 (52-86) arb.units, 62 (51-74) arb.units, 99 (59-139) arb.units] responses, but not LBP [Δ 9.0 (6.9-11.2) µg/mL, 9.2 (7.2-11.3) µg/mL; 9.8 (8.4-11.2) µg/mL], were observed on V0001 and V006 compared with CON (P < 0.05), respectively. GIS did not significantly differ between the trials .
Conclusions: The consumption of beverages containing AA, ranging 4.5 to 6.4 g/L, twice daily for 7 days, before and during exertional heat stress ameliorated the gastrointestinal integrity and systemic inflammatory responses associated with EIGS but without exacerbating GIS.
Nonsurgical Management of the Medial Collateral Ligament of the Knee: Understanding Adherence to Bracing TreatmentDana J. Hunter, MSc,*,†,‡,§,¶,‖,** Nicholas G. Mohtadi, MSc, MD, FRCSC,*,†,‡ S. Nicole Culos-Reed, PhD,§,‖,**,††,‡‡,§§ and Victor M. Y. Lun, MSc, MD,* and Amanda M. Black, CAT(C), PhD‡,§,¶,‖,**
Affiliations: *Sport Medicine Centre, Faculty of Kinesiology, University of Calgary, Calgary, AB, Canada; †McCaig Institute for Bone and Joint Health, Cumming School of Medicine, University of Calgary, Calgary, AB, Canada; ‡Sport Injury Prevention Research Centre, Faculty of Kinesiology, University of Calgary, Calgary, AB, Canada; §Alberta Children's Hospital Research Institute, University of Calgary, Calgary, AB, Canada; ¶Hotchkiss Brain Institute, University of Calgary, Calgary, AB, Canada; ‖O'Brien Institute for Public Health, University of Calgary, Calgary, AB, Canada; **Faculty of Kinesiology, University of Calgary, Calgary, AB, Canada; ††Arnie Charbonneau Cancer Institute, Calgary, AB, Canada; ‡‡Department of Oncology, Cumming School of Medicine, Calgary, AB, Canada; and §§Department of Psychosocial Resources, Tom Baker Cancer Centre, Cancer Care, Alberta Health Services, Calgary, AB, Canada.
Objective: To understand the facilitators and barriers to wearing a brace for the nonsurgical management of the medial collateral ligament of the knee.
Study Design: A qualitative study guided by patient-oriented research (POR) principles and interpretivist grounded theory (IGT).
Subjects: Sixteen patients (6 male and 10 female, age range: 32-64 years) from a randomized clinical trial (RCT) comparing the effectiveness of 2 different 6-week knee bracing protocols. The patients were recruited within a day of completing the bracing treatment.
Observation Technique: Subjects were interviewed using a semistructured guide to understand the patient's experience of wearing the brace as prescribed.
Outcome Measures: IGT was used to develop an understanding of the facilitators and barriers to MCL knee bracing adherence. The final model was coconstructed with 2 patient researchers recruited from the RCT.
Results: Five core categories were identified to classify the diverse facilitators and barriers to brace wearing: patient factors, clinical context, treatment factors, injury factors, and external factors. The resulting patient-centered model demonstrates how the complex balance between the facilitators affected patients' decision to wear the brace. Patient-specific facilitators were crucial to increasing brace wearing, especially having a strong desire to heal, experience with similar treatments, a good understanding of the purpose of the treatment, being of older age, and using positive coping mechanisms. Other facilitators of brace adherence were identified as positive social support, frequent clinical follow-ups, building effective relationships with clinicians, and higher brace satisfaction (i.e., ease of use and efficiency). Key contributors to reduced brace-wearing adherence were recognized as low treatment satisfaction (i.e., treatment duration and brace discomfort), certain sleeping habits, symptom improvement, and interpersonal hindrances (e.g., negative affect, low resilience, depression, anxiety).
Conclusions: Understanding the impact of treatment on clinical and patient-reported outcomes requires a thorough consideration of treatment adherence. This qualitative patient-oriented study provides a greater understanding of the complex nature of adherence to bracing MCL injuries. Recommendations for key knowledge users include improving bracing technology and comfort, implementing regular follow-up appointments with consistent clinicians, providing patients with high-quality information (i.e., injury and treatment pamphlet), and aiding patients in developing effective coping mechanisms and positive social support.
An Investigation of Active Force in Skeletal Muscle Fibers from Children With Cerebral PalsyGavin K. Thomas,* Venus A. Joumaa, PhD,* Tim L. Leonard, PhD,* Jason J. Howard, MD,† Robert J. Holash, PhD,* and Walter Herzog, PhD*
Affiliations: *Human Performance Lab, Faculty of Kinesiology, University of Calgary, Calgary, AB, Canada; and †Department of Orthopaedic Surgery, Nemours/Alfred I. duPont Hospital for Children, Wilmington, Delaware.
Objective: To investigate the ability of single muscle fibers isolated from children with cerebral palsy (CP) to produce active force.
Study Design: Experimental study.
Subjects: Twenty-four muscle fibers from 6 adductor longus muscle biopsies isolated from children with CP.
Intervention: Adductor longus biopsies were obtained from children with CP (n = 6, 2-12 years) who underwent tendon release surgery. Muscle biopsies were permeabilized using 1% triton X-100 for 3 hours on ice. Fibers (N = 24) were isolated and then activated using a solution containing calcium and ATP. The active force–length (F–L) relationship of the fibers was determined using maximal activation at sarcomere lengths ranging from 2.4 μm to 3.4 μm. Sarcomere lengths were determined using laser diffraction. Force was normalized to fiber cross-sectional area to obtain stress. Due to the absence of samples from typically developing children, the maximal active stress of fibers from children with CP was compared with that produced by fibers from 1-month-old mice (equivalent human age of 12-years) and adult rats, which are known to produce active stresses similar to those produced by human fibers.
Outcome Measures: The outcome measures were the active F–L relationship of fibers from children with CP, and the maximal active stress of fibers from children with CP and mouse and rat muscles.
Results: We observed a leftward shift in the F–L relationship of the fibers from children with CP compared with a theoretical human F–L relationship, that is, peak stress occurred at a sarcomere length (2.4 μm), placing it on the ascending limb of the theoretical human F–L relationship. Furthermore, the maximal active stress of the fibers from children with CP was reduced (P < 0.05) compared with young mouse and adult rat fibers (82 ± 34 kPa vs 115 ± 39 kPa, 139 ± 44 kPa, and 143 ± 27 kPa, respectively).
Conclusions: We conclude that the contractile ability of fibers from children with CP is likely compromised. Further research is needed to investigate the origin of this contractile deficiency and how active force loss could be prevented. Based on findings from previous research, we speculate that the decrease in isometric force capacity is related to a reduction in titin quantity in muscles from children with CP.
Height, Weight, Strength, and Speed Depend More on the Status of Biological Maturation than on Chronological AgeEduard Bezuglov,*,† Grigoriy Malyshev,† Larisa Shagiakhmetova,† Nadezhda Semenyuk,† Bekzhan Pirmakhanov,‡,§ and Anton Emanov†
Affiliations: *Department of Sports Medicine and Medical Rehabilitation, Sechenov First Moscow State Medical University of the Ministry of Health of the Russian Federation, Moscow, Russia; †Academy of Talents, Moscow, Russia; ‡Al-Farabi Kazakh National University, Faculty of Medicine and Health Care, Department of Epidemiology, Biostatistics and Evidence-Based Medicine, Almaty, Kazakhstan; and §FC Kairat, Almaty, Kazakhstan.
Corresponding author: Bekzhan Pirmakhanov, [email protected]
Background: Over the past years, a number of studies involving young elite soccer players have shown that parameters such as strength, speed, height, and weight are closely related to the status of biological maturity. However, there are currently no data comparing the effects of chronological age, birth quartile, and biological maturity on these parameters.
Materials and Methods: Six hundred seventy-eight male youth soccer players from 8 elite soccer academies aged between 12 and 18 years were tested. Testing has always been conducted by the same team of testers using the same equipment (Smart Jump and Smart Speed PRO systems) on standard-sized soccer fields with artificial turf. Testing was always performed in a strictly defined order and included measurement of standing height and body weight, horizontal jump, countermovement jump, 20-m sprint with 5-m and 10-m split, dribbling, juggling, and short and long passes. To determine the degree of biological maturation, growth from the predicted growth of parents, determined by the Khamis–Roche formula, was used. The dates of birth of all the players who took part in the study were also analyzed.
Results: In total, the study involved 678 soccer players aged 12.1 to 17.9 years (average age 14.0 ± 1.4 years, height 174 cm ± 10.3 cm, weight 64.0 kg ± 11.0, and body mass index 20.9 ± 2.4). When studying the relationship between age in years and months, quartile of birth, degree of biological maturation, and analyzed parameters, significant and moderate relationships were found between maturity status and height (R = 0.78, P < 0.001), weight (R = 0.77, P < 0.001), horizontal jump (R = 0.72, P < 0.001), and 5-m (R = −0.53, P < 0.001), 10-m (R = −0.66, P < 0.001), and 20-m sprints (R = −0.75, P < 0.001), and this relationship for these parameters was stronger than that with chronological age.
Conclusion: The status of biological maturity has a more significant effect on the speed, strength, and anthropometry of young elite soccer players than chronological age.
Category: Sport Injury Prevention
Exploring the Relationship Between Cumulative Internal Load and Injury Risk in Women's SoccerJemma Kim, SPT, Katie Sniffen, MS, ATC, and Oluwatoyosi Owoeye, PhD, MS, BPT
Affiliation: Department of Physical Therapy and Athletic Training, Saint Louis University, St. Louis, Missouri.
Objective: This study aimed to investigate the relationship between cumulative internal load and injury rate among National Collegiate Athletic Association (NCAA) Division 1 women's soccer athletes.
Study Design: Prospective cohort.
Subjects: Twenty-seven women's soccer athletes (mean age = 19.5 years, standard deviation = 1.14).
Observation Technique: Athletes reported rate of perceived exertion (RPE) values to team athletic trainers within 10 minutes of the end of each practice and game session over the course of 1 competitive season of 14 weeks. RPE values were multiplied by session duration (minutes) to calculate session RPE, expressed in arbitrary units (AUs), as our measure of internal load.
Outcome Measures: The study outcome was all-complaint knee and ankle injury incidence throughout the competitive season. All-complaint knee and ankle injuries were collected postseason using a modified version of the Oslo Sports Trauma Research Center-Patella Tendinopathy Questionnaire through self-report.
Results: The team median cumulative load for all 27 female soccer athletes was 21 159 (range: 3255-26 491) AUs across the 14-week season. Trends in the team's weekly median cumulative internal load per week revealed a voltage drop following a high load in week 1 to week 2 and dips during midseason and the last 2 weeks of the season. A total of 15 knee and ankle injuries (7 time-loss and 8 non–time-loss) occurred during the observation period. The overall injury incidence was 14.14 injuries per 1000 hours of exposure, equivalent to 56 injures per 100 athletes per season. Athletes who experienced an injury had a median cumulative load of 21 347 (range: 20 751-25 470) AUs throughout the season, compared with 18 777 (range: 15 365-22 691) AUs in noninjured athletes.
Conclusions: Results of this study suggest a potential association between cumulative internal load and injury risk among collegiate women's soccer athletes. Internal load monitoring and external load regulations could help maximize performance and reduce lower limb injury risk.
Acknowledgements: This study was funded by a grant from the Applied Health Sciences Research Program at the Saint Louis University and the Irma Ruebling Endowed Research Fund (PI: Dr. Olu Owoeye).
The Impact of a 48-Hour High-Carbohydrate Diet, With High or Low FODMAP Content, Before Endurance Exercise on Gastrointestinal Motility and Symptoms, and Exercise PerformanceRachel Scrivin, MSc,*,† Ricardo J. S. Costa, PhD,‡ Gary Slater, PhD,* Alice Mika, MDiet,‡ Christopher Rauch, BHon,‡ and Pascale Young, MSc‡
Affiliations: *University of the Sunshine Coast, Sippy Downs, Queensland, Australia; †Toi Ohomai Institute of Technology, Tauranga, New Zealand; and ‡Monash University, Melbourne, Victoria, Australia.
Objective: To determine the effects of a 48-hour, high-carbohydrate, high-fermentable oligosaccharide, disaccharide, monosaccharide, and polyol (FODMAP) (HCHF) or high-carbohydrate low-FODMAP (HCLF) diet on gastrointestinal motility and symptoms in response to endurance exercise, and subsequent exercise performance.
Study Design: Randomized, double-blind, crossover trial.
Subjects: Twelve (n = 10 male and n = 2 female) recreationally competitive endurance runners [mean (SD): age 42 (5) years, height 1.74 (0.08) m, body mass 72.1 (13.7) kg, fat mass 20 (8)%, and V̇O2max 53.2 (8.6) mL/kg/min] with preexisting, recurrent, exercise-associated gastrointestinal symptoms (GIS) volunteered to participate.
Intervention: Participants were randomly assigned to a 48-hour high-carbohydrate (10-12 g/kg/d) high-FODMAP (50-60 g/d) (HCHF) and a high-carbohydrate low-FODMAP (2-3 g/d) (LCLF) intervention, with a 7-day washout between the trials. After the dietary intervention, participants completed 2-hour steady-state running at 60% V̇O2max, followed by a 1-hour distance test, in temperate ambient conditions (23°C, 49% RH). Maltodextrin (10 g at 10% wt/vol) was provided every 20 minutes during steady state, plus water provided ad libitum during the entire 3 hours. A 150-mL solution containing 20 g of lactulose was provided 30 minutes into the distance test to determine orocecal transit time (OCTT).
Outcome Measures: Preexercise and postexercise breath samples breath hydrogen (H2) were collected, and Ex-GIS and rectal temperature (Tre), were measured. Every 15 minutes during steady-state exercise, HR, RPE, and Ex-GIS were recorded. During the distance test, the distance completed was recorded every 5 minutes, plus HR and RPE every 15 minutes. Breath samples were collected every 15 minutes during the 3-hour recovery. Breath samples were analyzed for hydrogen (H2) to determine OCTT.
Results: OCTT did not significantly differ between HCHF 83 (58) minutes and HCLF 95 (55) minutes (P = 0.59). Greater total-GIS were reported preexercise (P = 0.04) and during (p = 0.02) steady state on HCHF; however, greater total-GIS were reported at the 1-hour to 2-hour recovery period on HCLF (P = 0.04). There was no difference in measured HR, RPE, or Tre between the trials. Distance completed was 9.9 (1.7) km and 10.0 (1.6) km on HCHF and HCLF (P = 0.33), respectively.
Conclusions: A 48-hour HCHF diet before endurance running leads to greater GIS before and during exercise; however, this does not impact exercise strain, gastrointestinal motility, or exercise performance. Greater GIS in the 1-hour to 2-hour recovery period with the HCLF trial requires further investigation.
Acknowledgements: R. Scrivin has received an Australian Government Research Training Program Scholarship for research.
CAESM Research Abstract Submission
Contraception Choice for Female Endurance Athletes: What's Sport Got to Do With It?Stephanie E. Ryall, BSc, Heidi A. Ohrling, BSc, and Jane S. Thornton, MD, PhD
Affiliation: Schulich School of Medicine & Dentistry, Western University, London, ON, Canada.
Objectives: (1) To better understand which contraceptives female endurance athletes are currently using or have previously used, and how these contraceptives are perceived to have impacted their health and performance. (2) To characterize the contraception selection process for female endurance athletes, including common concerns, satisfaction with physician encounters, and resources consulted.
Study Design: Exploratory survey study delivered anonymously on Qualtrics. The study was open from August 2021 to March 2022. Participant recruitment through social media and emails sent to university and club coaches, and endurance sport organizations.
Subjects: Three hundred twenty-three participants met the following eligibility criteria: (1) Is a female endurance athlete ≥18 years old? (2) Has used or considered using contraceptives that require consultation with a health care professional? (3) Has thought about how contraceptives could impact athletic performance?
Results: Of the participants currently using contraception (n = 182), 50.5% use the hormonal intrauterine device (IUD), 28.6% use an oral contraceptive pill (OCP), and 13.2% use the nonhormonal IUD; 90% of hormonal IUD users reported being happy with their selection; less than 5% experienced a negative impact on training, and nearly 40% thought that it had a positive training impact likely from decreased menstrual bleeding and symptom management. In comparison, the OCP and nonhormonal IUD users were not as satisfied with their selected contraceptive methods; 73.9% of nonhormonal IUD users experience heavier and more irregular bleeding, which was consistently cited as having a major negative impact on training; 30.6% of individuals on the OCP reported adverse body composition outcomes and negative mood changes. In addition, of the athletes who received contraceptive counseling from their physician (n = 84), 38.6% did not feel that athletic performance was adequately factored into the discussion.
Conclusion: Our data suggest that the hormonal IUD is perceived to be the superior contraceptive regarding the impact on endurance performance. These results can help inform female endurance athletes inquiring about contraception, as well as the physicians advising them. This is particularly important as a significant percentage of female endurance athletes were frustrated and do not feel understood by their physicians during contraceptive counseling.
Effect of Amphetamines, Opioids, Androgenic Anabolic Steroids, and Cannabis on the Development of Chronic Traumatic Encephalopathy Features in Individuals Exposed to Mild Head Trauma: A Scoping Review and Proposed Nomenclature ChangePietro S. II Cianflone, BSc,* and Neil Craton, MD, MHK*,†
Affiliations: *Max Rady College of Medicine, University of Manitoba, Winnipeg, MB, Canada; and †School of Kinesiology and Applied Health, University of Winnipeg, Winnipeg, MB, Canada.
Objective: To determine the effects of amphetamines, opioids, androgenic anabolic steroids (AAS), and cannabis on the development of chronic traumatic encephalopathy (CTE).
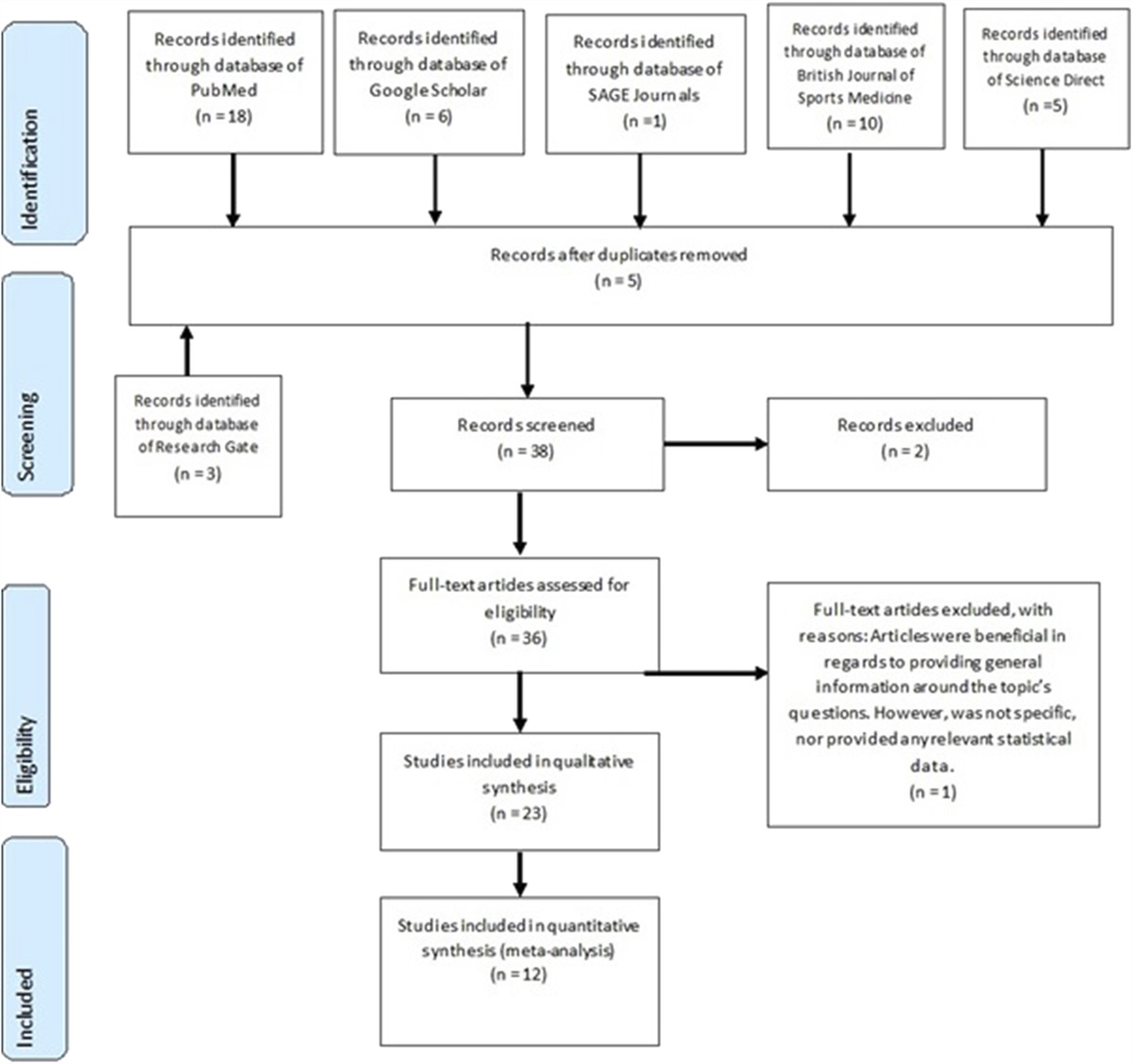
Data sources: A scoping review was conducted in the PubMed, Embase, Cochrane Library, Scopus, CINAHL, and SPORTDiscus electronic databases. Reference lists of included studies were also screened.
Main Results: Two thousand three hundred ninety-seven records were identified with an initial search. Seven studies met the following eligibility criteria: quantitative primary literature investigating amphetamines, opioids, AAS, or cannabis among humans with history of mild traumatic brain injury or concussion, with exploration of clinical and/or neuropathological features of CTE. Of these, 4 addressed cannabis use and 3 addressed endogenous AAS. Cannabis use and endogenous AAS deficiencies in individuals exposed to mild head trauma were associated with mostly adverse or neutral changes related to CTE features. Cannabis use may affect postconcussion suicidality and exacerbate postconcussive symptoms even several years after injury. Post–mild head injury AAS deficiencies were associated with cognitive, behavioral, mood, and motor changes consistent with CTE. Postinjury AAS deficiencies were also associated with brain changes suggestive of neuropathological features supporting a CTE diagnosis. No studies investigating amphetamines, opioids, or exogenous AAS met eligibility criteria.
Conclusions: The literature on the effects of amphetamines, opioids, AAS, and cannabis on CTE features in patients with mild head trauma is very limited. Knowledge gaps and opportunities for future research were identified. We proposed a nomenclature change from CTE to idiopathic degenerative encephalopathy of athletes (IDEA) to more accurately reflect the literature surrounding this condition.
Acknowledgements: The authors thank Dr. Oliver Leslie for his work on a concept paper that helped lay the groundwork for this present study. The authors thank University of Manitoba librarians Carol Cooke and Caroline Monnin, for their advice regarding methodological considerations. They also thank Dr. Brian Postl, former Dean of the Max Rady College of Medicine, who provided funding as part of the Med Summer Research Program.
ORIGINAL RESEARCH ABSTRACT
Prevalence of Depression in Retired Professional Baseball and Hockey PlayersJonathan Lockwood, MA, MD, Shannon Flatley, BSc, Yushu Wang, Carrie Esopenko, PhD, and Brian Levine, PhD
Affiliation: Rotman Research Institute, Baycrest Health Sciences, Toronto, ON, Canada.
Objective: To compare the prevalence of depression in a matched sample of retired professional baseball and hockey players.
Study Design: Cross-sectional Survey.
Subjects: Seventy-eight retired professional baseball players (major and minor league baseball) and 22 retired professional hockey players (national hockey league)
Observation Technique: (1) Professional Baseball Players Alumni Facebook Group through Qualtrics Online Survey Platform and (2) Data gathered by Esopenko, Carrie, et al. “Cognitive and psychosocial function in retired professional hockey players.” Journal of Neurology, Neurosurgery & Psychiatry 88.6 (2017):512–519.
Outcome Measures: (1) The prevalence of depression using the Patient Health Questionnaire-9 (PHQ-9) (threshold of >9) in baseball players and Beck Depression Inventory (BDI) (threshold of >8) in hockey players. (2) Prevalence of reported lifetime history of concussion.
Results: Prevalence of depression in baseball players (PHQ-9) was 19.23% and 40.91% in hockey players (BDI). History of concussion events in baseball and hockey players was mean = 0.99, SD = 1.37 and mean = 4.8, SD = 2.7, respectively.
Conclusion: There was a significant difference in the prevalence of depression between retired baseball players and hockey players. Given the differences in the prevalence of sports-related concussion between the 2 sports and in this sample, these data support the negative psychological impacts of concussion in professional athletes after they retire. The depression scores in retired baseball players suggest that there are contributing factors in addition to sport-related concussion that negatively impact the psychological well-being of athletes after they retire.
The Impact of Time from Injury to Surgery on Bucket-Handle Meniscus Tear Repair Rates: A Retrospective Cohort StudyAhmad Al-Tawari, MD,* Stephanie K. Nathanail, CAT©, MA,† Aidan Comeau, BKin,‡ Michael D. Kennedy, PhD,‡ Khanh Vu, PhD,§ and Mark F. Sommerfeldt, MD, MPH*,¶
Affiliations: *Division of Orthopaedic Surgery, Department of Surgery, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, AB, Canada; †Orthopaedic Surgery, Alberta Health Services, Edmonton, AB, Canada; ‡Faculty of Kinesiology, Sport, and Recreation, University of Alberta, Edmonton, AB, Canada; §Real World Evidence Unit, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, AB, Canada; and ¶Glen Sather Sports Medicine Clinic, University of Alberta, Edmonton, AB, Canada.
Objective: To assess the association between time from injury to surgery on meniscus repair rates in a cohort of patients with bucket-handle meniscus tears.
Study Design: Retrospective cohort study.
Subjects: Forty-nine patients (16 females and 33 males) with confirmed bucket-handle meniscus tears presenting to an orthopedic surgeon and receiving surgery between January 2020 and December 2020.
Intervention/Observation Technique: Retrospective chart review.
Outcome Measures: The primary outcome was the impact of time from injury to surgery (in weeks) on meniscal repair (binary outcome: yes or no) at the time of surgery. Data were analyzed using logistic regression. Statistical significance was set at ⍺ = 0.05.
Results: Mean patient age was 34.6 years (SD = 10.9). Twenty-nine (59%) patients presented with concomitant anterior cruciate ligament tears. Median time to surgery was 21 weeks (interquartile range [IQR] = 7.5, 51 weeks). Thirty-eight patients (78%) underwent meniscus repair, whereas 11 (78%) (22%) received a meniscectomy. The meniscus repair group demonstrated a significantly shorter time to surgery when compared with the meniscectomy group (14 weeks [IQR = 5.6, 34.1 weeks] vs 41.7 weeks [IQR = 21.6, 106.7 weeks], respectively; P = 0.01). Patients with a time to surgery of less than 21 weeks had a 6.9-fold increase in the likelihood of meniscus repair (95% CI, 1.3-36.5, P = 0.02). Patient age, sex, and concomitant anterior cruciate ligament status were not found to influence whether a repair was performed.
Conclusions: Patients with bucket-handle meniscus tears who underwent surgical treatment within 21 weeks from the time of injury demonstrated a significantly higher likelihood for repair as compared with those experiencing a longer time to surgery. Longer-term follow-up is needed to determine the rates of successful repair including the need for revision surgeries in this cohort; this question will be addressed in future work. As meniscal resection accelerates knee osteoarthritis thereby resulting in worse patient outcomes, study findings highlight the importance of accurate and time-sensitive diagnosis and surgeon referral to improve the odds of performing meniscus-sparing procedures at the time of surgery. These results can be used to better inform benchmarks/standards for timely treatment of bucket-handle meniscus tears in the Canadian setting.
CASEM—Informing Return to School Practices for Students After Concussion
Educator Perspectives on Supporting Students to Return to School Following a ConcussionHeather A. Shepherd, OT, MSc,* Isla J Shill, MSc,*,†,‡,§ Keith Owen Yeates, PhD,†,‡,¶ Nick Reed, OT, PhD,‖,**,†† Jeffrey G. Caron, PhD,‡‡,§§ Kathryn J. Schneider, PT, PhD,*,†,‡,¶¶,‖‖ Amanda M. Black, CAT(C), PhD,*,†,‡,§ and Carolyn A. Emery, PT, PhD*,†,‡,§,***
Affiliations: *Sport Injury Prevention Research Centre, Faculty of Kinesiology, University of Calgary, Calgary, AB, Canada; †Alberta Children's Hospital Research Institute, University of Calgary, Calgary, AB, Canada; ‡Hotchkiss Brain Institute, University of Calgary, Calgary, AB, Canada; §O'Brien Institute for Public Health, University of Calgary, Calgary, AB, Canada; ¶Department of Psychology, University of Calgary, Calgary, AB, Canada; ‖Department of Occupational Science and Occupational Therapy, University of Toronto, Toronto, ON, Canada; **Rehabilitation Sciences Institute, University of Toronto, Toronto, ON, Canada; ††Bloorview Research Institute, Holland Bloorview Kids Rehabilitation Hospital, Toronto, ON, Canada; ‡‡School of Kinesiology and Physical Activity Sciences, Faculty of Medicine, Université de Montréal, Montreal, QC, Canada; §§Center for Interdisciplinary Research in Rehabilitati
留言 (0)