
記住我
Vehicle speed is a major cause of RTCs and injuries.
Speed humps help reduce vehicle speeds, number of road crashes and injuries.
WHAT THIS STUDY ADDSThe first study in Ghana to use before-and-after study with controls design to examine the effect of speed humps on the severity of traffic injuries (fatal/severe/minor) on trunk roads.
Speed humps reduce the severity of road traffic injuries during crashes on trunk roads in Ghana.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICYBackgroundRoad traffic injuries (RTIs) are a major but neglected global public health burden, demanding concentrated and rigorous measures for effective and sustainable mitigation.1–3 According to the WHO, for every 23 seconds, someone is killed on the road, and between 20 and 50 million people sustain injuries worldwide.4 The Global Burden of Disease 2019 report shows that RTIs have been the leading cause of death among people aged 10–49 years since 1990 and the seventh major cause of all deaths globally.5
Over the past three decades, road fatalities and injuries have increased in Africa. The rate at which Africans die due to RTIs (24.1 per 100 000 population) is higher than the global rate,4 with the risk of dying ranging from 34% to 64% in the African regions.6 In Ghana, more than 10 000 people sustain RTIs every year since the declaration of the Decade Plan of Action for Road Safety, 2011–2020.7 From 1 January to 13 October 2021, a total of 11 858 crashes, 11 659 RTIs and 2126 road deaths were recorded by the Motor Traffic and Transport Department (MTTD) of the Ghana Police Service.8 9 Vehicle speed coupled with single-lane roads have been identified and reported in several studies for the past three decades as a major risk factors for RTCs and the severity of resultant injuries.2 3 10–12
Traffic calming (TC) interventions such as speed humps (SH) have been employed globally to mitigate crashes and RTI burden, mainly attributed to vehicle speed.10 13 Studies on TC have reported its safety for road users.10 13–15 Afukaar and Damsere-Derry16, Distefano and Leonardi17, and Elvik18 reported reductions in RTIs after TC devices were installed.16–18 Yeo and colleagues found that installing SHs lowers the likelihood of crashes and severe injuries.14
Despite the many attempts to curb this burden, estimates project that RTIs will become the third leading cause of death globally by 2030 if proper measures are not implemented.4 Studies from high and low-income countries have reported how TC interventions reduce vehicle speeds, the occurrence of crashes and number of injuries.10 14 16 19 Fewer studies have reported on the relationships between the injury severity and TC interventions.14 In Ghana, few studies have reported on the effect of TC interventions on RTIs. Studies on TC interventions in Ghana predominantly examine their influence on speed10 and crashes, but rarely on RTIs.16 The studies in Ghana either combine two or more types of TC devices and hence the effectiveness of each device is virtually unknown. Again, the studies focused on pedestrian injuries,10 16 but the current one was on all road users. Also, they only employ before-and-after study designs without a control group.16 Therefore, this study sought to use before-and-after study with controls design to examine the effect of SHs on severity of RTIs and assess the physical dimensions of SHs in selected settlements on national trunk roads traversing towns in Ghana. To the best of our knowledge, our study is the first to employ before-and-after study with controls design to assess the effect of SHs on severity RTIs.
MethodsStudy designA quasi-experimental before-and-after study with controls design (figure 1) was employed to answer the research questions. The study compared data on injury consequences 3 years before and after the SHs installation at the intervention and control sites. The addition of controls would reduce limitations associated with regression to the mean.
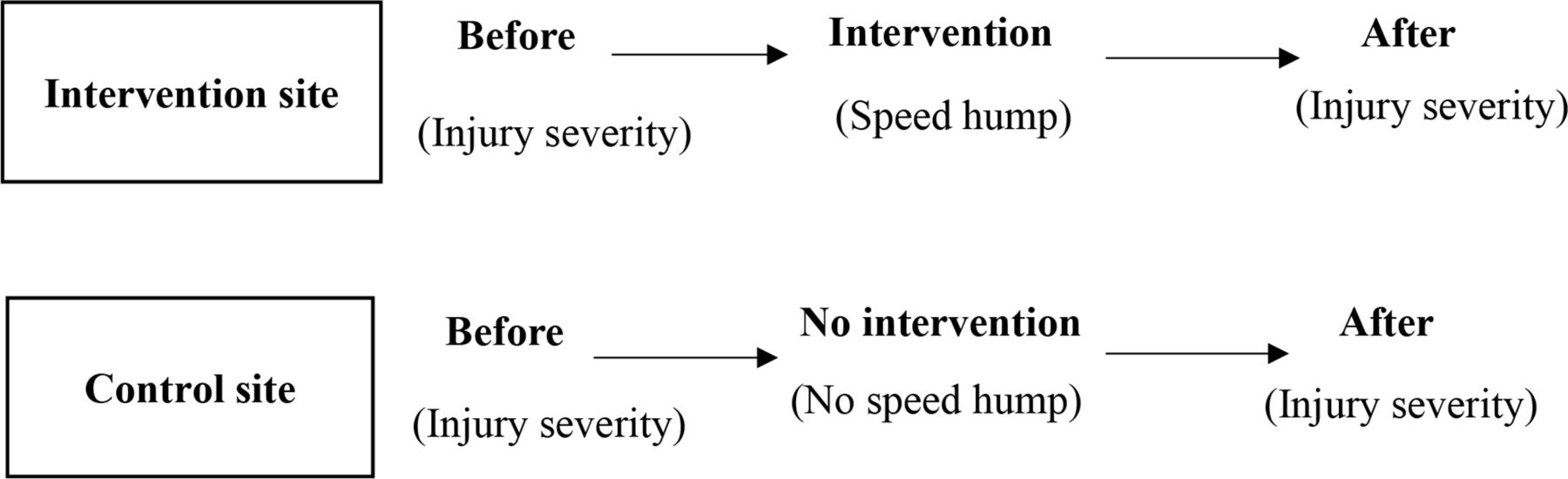 Figure 1
Figure 1 Quasi-experimental before-and-after study with controls diagram for the study.
InterventionTC interventions have been implemented on some national trunk roads that go through settlements in Ghana. National trunk roads are major roads built for long-distance travel connecting cities and have as part of their label the letter ‘N’. The implementation of these interventions was to reduce vehicle speed and crashes. In Ghana, seven types of TC measures have been approved by the Ghana Highway Authority (GHA) to be installed on trunk roads.
SHs were considered as the intervention in this study because they are the most common TC measure on national trunk roads in Ghana. GHA has recommended circular (figure 2) and trapezoidal (figure 3) SHs with crown heights of 10 cm to be used on trunk roads. The radius (for circular humps), length, slanted surface or ramp (for trapezoidal humps) are dependent on the posted speed limit.20
 Figure 2
Figure 2 Circular speed hump as reported in Ghana Highway Authority (GHA) traffic calming design guidelines.
 Figure 3
Figure 3 Trapezoidal speed hump as reported in Ghana Highway Authority (GHA) traffic calming design guidelines.
Selection of intervention and control sitesThe intervention and control sites were on the same trunk roads, and their selection was done in two stages. Initially, the National Road Safety reports were reviewed for sampling of the national trunk roads. The criteria for sampling the roads were them being in the Ashanti Region, high number of crashes recorded annually and posted settlement speed limits of 50 km/hour. Three trunk roads, namely the Kumasi–Techiman (N10), Kumasi–Sunyani (N6) and Kumasi–Accra (N6), were sampled based on the above criteria.
Second, the GHA was contacted for their inventory on SHs on the sampled trunk roads to guide selection of settlements that would serve as intervention sites. Traffic injury data were available to year 2020; hence, roads traversing settlements that had SHs installed between 2014 and 2017 were selected as intervention sites. This was done to obtain 3 years of before-and-after data. Each intervention settlement had an average of two consecutive SHs.
Settlements adjacent to the intervention site, with 50 km/hour speed limit and had no SH, were selected as the control sites. At least 95% of the vehicles that traversed the intervention sites went through the control sites as well. A total of 12 settlements, six with and without SH, were selected as intervention and control settlements, respectively.
Data collectionThe study used two main sources of data, primary and secondary. The primary data consist of the physical measurements, namely height, width, shape and the distance between each consecutive intervention. The secondary data was on RTIs sourced from the Center for Scientific and Industrial Research (CSIR)-Building and Road Research Institute (BRRI) national crash database.
Physical measurements of humpsCrown height measurementThree instruments were used: a spirit level, steel tape and 5 m straight 2×4-inch wood. The wood was held by two research assistants and placed across the top of the hump in the direction of travel. A spirit level was placed on top of the wood to ensure it was levelled. A steel tape was then used to measure the height of the hump from the top of the road pavement to the soffit of the wood. Three measurements of the height were made for each hump at different sections, and the average was recorded.
SH length and widthA precimeter (measuring wheel) was employed for this purpose. A research assistant walked with the precimeter from one end to the other end of the hump in the direction of travel to record the length. The research assistant then measured the width of the hump by walking across the road with the precimeter.
Distance between humpsA research assistant walked with the precimeter from one hump to the other consecutive one and recorded the distance between them.
RTI dataThe national crash data are a collation of all police files by MTTD. The CSIR-BRRI’s technicians extract information from Ghana Police MTTD files into standard case report forms that form the basis of its database. The case report forms extract information about the nature crashes, their location, the road, the vehicle(s) and passenger and pedestrian casualties. The information is coded and stored using a Micro-computer Accident Analysis Package software developed by the Transport Research Laboratory, UK. The injury data for the current study was retrieved from 2011 to 2020. Data from CSIR-BRRI have been observed to have some level of under-reporting, as not all crashes are documented. Some incidents of crashes and injuries are not reported, whereas others are under-reported.7 That notwithstanding, it remains the most reliable nationwide RTI database. Based on the year of installation of hump obtained from GHA, the injury data were segregated as before and after in the intervention and control settlements.
Study variablesOutcome variableThe outcome variable in this study was the severity of injury during crashes. This variable was measured in an ordered form, that is, fatal, severe and minor. Severe injury is when a casualty is detained as an in-patient for more than 24 hours, whereas minor injury is when a crash victim requires at most first aid attention.7
Exposure variablesThe main exposure variable was SH status. The presence of SH was considered as an intervention site and control if absent. Other covariates include age of victim, time of crash, road width, level of illumination of the road and collision type.
Statistical analysisDescriptive analysis used frequencies and percentages for categorical variables, while means and standard deviation (SDs) were used to summarise the physical characteristics of the SH and crash characteristics. The analysis compared the severity of RTIs at the intervention and control sites before and after the installation of SH. A one-sample t-test was used to test the difference between the recommended mean height and the mean height of the SHs from the field.
Univariable and multivariable ordered logistic regression were used to examine the influence of SHs on the severity of injury during crashes. Independently significant variables (p≤0.05) at the univariable level were included in the multivariable analysis. Also, variables considered important or potential confounders were adjusted for in the multivariable analysis. The forward stepwise approach was used in incorporating variables into the model. The backward approach was also performed. Variables were re-entered and rechecked until a parsimonious model was achieved. The Alkakne information criterion (AIC) was used as the goodness-of-fit test statistic to compare the models. The model with the minimum AIC was considered the best fit. The proportional odds assumption was tested and at both before and after analyses the p values were 0.807 and 0.730, respectively; hence, the estimates from ordered logistic regression were not considered problematic. Multicollinearity of the adjusted variables was checked using variance inflation factor. Two separate models were built, one for before and one for after, and comparison was made on the estimates. Data was analysed using STATA V.16.
Regression to the mean, which is one of the statistical limitations of before-and-after study, was not considered an issue in this study because the study did not compare injuries before and after in sites with SH only, but it compared the severity of injuries in sites with SH against sites without SHs before and after the SHs were implemented.
ResultsPhysical characteristics of SHs on the study roadsTable 1 presents the characteristics of the SH devices. Altogether, 15 SHs were surveyed in the six settlements selected as the intervention sites. The overall mean height of humps on all the road sections was 10.9 cm high, with a minimum and maximum height of 7 and 19 cm high, respectively. The highest mean (15.5 cm) height was found in Namong on the Kumasi-Techiman highway, and the lowest (8.25 cm) was found in Juaso on the Kumasi-Accra highway. A one-sample mean t-test found that the overall mean height (m=10.9 cm, SD=2.7) was significantly higher than the recommended height of 10 cm by GHA20 for all SHs (p>0.001).
Table 1Characteristics of speed hump measures on the road sections
The overall average spacing between two successive SHs estimated along the road sections was 207.17 m. The spacing between SHs is dependent on the posted speed limit: 250 m for 50 km/hour speed limit, 100 and 75 m for 40 and 30 km/hour speed limit, respectively.20 The mean spacing at Namong far exceeded the recommended spacing for the 50 km/hour posted speed limit.
Characteristics of RTIs and crashes of casualties within the study periodTable 2 presents the characteristics of the casualties and RTIs before and after the installation of the SH devices. A total of 769 RTIs were recorded over the study period. Out of the total RTIs, 388 were recorded before the SH installation, of which 173 were from the control settlements and 215 were from the intervention settlements. Three hundred and eighty-one (381) of the total RTIs were recorded after the SH installation, of which 240 were from the control sites and 141 from the intervention sites. The overall median age of the victims was 33 years, with a minimum of 1 year and a maximum of 82 years. A higher proportion (43.1%) of victims were within the ages of 30–44 years. Males (73.6%) and pedestrians (58.0%) constituted a larger portion of the victims. Of the casualty class, 57.9%, 31.6% and 10.5% were pedestrians, drivers and passengers, respectively. Crashes involving two vehicles contributed a larger proportion (54%) of the injuries. Crashes on straight and flat roads contributed to about 83.0% of the injuries. A little above half (53.0%) of the injuries occurred during the daytime. About 27.0% of the casualties originated from run-off road collisions, 20.1% from head-on collisions and 19.1% from rear-end collisions. The vehicles that contributed more injuries were cars (32.6%) and buses (29.8%).
Table 2Characteristics of road traffic injuries and crashes within the study period
Effect of SHs on RTIs during crashesTable 3 presents the crude and adjusted analyses of the influence of SHs on RTIs. In both the crude and adjusted analyses at the before stage, fatal/serious/minor injuries were higher at the intervention sites than at the control sides. Fatal/serious/minor injuries were 35% and 6% higher in the adjusted and crude analyses, respectively, though it was not statistically significant (adjusted OR (aOR)=1.35, 95% CI 0.85 to 2.14; crude OR (cOR)=1.06, 95% CI 0.73 to 1.55).
Table 3The influence of speed humps on traffic injuries adjusting for other covariates
A significant change occurred after the installation of the SH devices. At the unadjusted stage, injuries (fatal/serious/minor) were reduced by 40% at the intervention sites compared with the control sites (cOR=0.60, 95% CI 0.41 to 0.90). After accounting for variables such as time of the crash, age of casualties, collision type, day of crash, road surface condition and road width, there was a reduction of 77% in fatal/serious/minor injuries at the intervention sites compared with the control sites (aOR=0.23, 95% CI 0.11 to 0.47). Other covariates were found to influence RTIs. Increasing the width of the road was found to be associated with an increase in RTIs. It was found that an increase in road width increases fatal/serious/minor injuries by 23% (aOR=1.23, 95% CI 0.97 to 1.56).
DiscussionThe average height of SHs were significantly higher than that recommended by the GHA. SHs reduced the severity of injuries.
A notable finding was that the SHs had heights higher than the requirements of the GHA for trunk roads of this nature. Significant increases in height of SH would assumedly reduce driving speeds across the section and result in less severe injuries when crashes occur. Findings by Damsere-Derry and colleagues on the Abuakwa-Bibiani highway where average heights of humps exceed the recommended values point to situations similar to the current study.21
Before the intervention, fatal/severe/minor injuries were higher (35%) at the intervention sites than the control sites. The study found a significant reduction in the severity of injuries after the SHs were installed. Fatal/severe/minor injuries reduced by 77% after humps were installed at the intervention sites. The reduction shows the effectiveness of humps in reducing severity of injuries during crashes on national trunk roads. On the other hand, severe and minor injuries increased at the control sites in the post-intervention period.
These findings align with the reduction (22%) in severe injuries reported by Rothman et al in Canada.13 Also, Bornioli et al reported a 63% reduction in fatalities with the introduction of speed calming intervention in Bristol, UK.22 Distefano and Leonardi studied three types of speed calming measures and their effect on crashes and injuries in Italy.17 They found a decrease in injuries after the implementation of the three types of speed calming measures. One resulted in a 50% reduction in injuries, the other 38% and the last 32%. Damsere-Derry et al’s study reported higher pedestrian fatal injuries in settlements with no SH.10 Unlike the current study that was focused on all road users, that by Damsere-Derry et al was only on pedestrians. Furthermore, their study combined a number of TC devices whereas the current one focused on humps. The reduction may be as a result of the discomfort drivers and passengers experience when a vehicle travelling at a higher speed hit vertically raised object on the road. This inadvertently leads to drivers reducing speed when traversing a section of the road with a hump. It is instructive that humps assessed in this study had heights higher than that required to reduce trunk road traffic speeds to acceptable levels by GHA. A significant increase in height of humps, it is speculated would lower the average speeds across the section resulting in less severe injuries during crashes.
There is a general perception among drivers that when vertical displacement interventions are made for speed calming, depending on the height, the discomfort may be eliminated by speeding over them. This will require further investigation to determine whether the additional increase over the standard had any influence on the results obtained. Also, significant increase in height may increase travel time over the section during peak traffic as speeds are reduced. This could result in delays for traffic and formation of platoons, and lead to driver irritation which has the propensity to trigger higher speeds and overtaking manoeuvres on other sections without humps during platoon dispersion. Could this contribute to the increase in severe injuries at the control site at the post-intervention period? This may require further studies.
ConclusionThe paper presented findings from a before-and-after study with controls design of the effect of SH interventions on RTIs on trunk roads traversing the Ashanti Region of Ghana. The findings highlighted a reduction in traffic injury severity after SHs were installed at the intervention sites. The severity of injuries in the control sites on the contrary worsened in the postintervention period. The findings suggest that SHs are effective road safety measures in reducing the severity of traffic injuries. The study only used selected sections on national trunk roads; it is therefore recommended that similar studies should be conducted on regional roads (ie, roads that link district capitals to their respective regional capitals, other nearest district capitals and major industrial, trade or tourist centres) and inter-regional roads (ie, roads of inter-regional importance to provide regional coherence). There is also room for studies to determine the extent of influence the additional height of the SH above the standard contributed to the results.
Data availability statementData are available upon reasonable request. Data are available upon a reasonable request.
Ethics statementsPatient consent for publicationAcknowledgmentsWe are grateful to the Regional Transport Research and Education Centre-Kumasi (TRECK) for funding this study, the CSIR-Building and Road Research Institute, Ghana Highway Authority and the National Road Safety Authority for granting us permission and access to the roads and injury data.
留言 (0)