This prospective study was performed in the neuro-ophthalmology unit of the Lyon University Hospital between November 2019 and March 2022.
We recruited patients with bilateral vestibular hypofunction and cerebellar dysfunction (BVH-CD group) and patients with isolated bilateral vestibular hypofunction (BVH group). Data of 6 previously recorded patients (2016) were used for the BVH group [3].
All subjects met the clinical BARANY criteria A, B, C, and D. For criteria C, we only used vHIT as our study focused on compensation during high velocity head movements.
In order to reduce biases while comparing the latency of the first catch up saccade between the group of BVH patients and the group of BVH-CD patients, we aimed for these two groups to be as comparable as possible. As age has been shown to affect SL-CuS in patients with bilateral vestibular hypofunction [3], we matched mean age across our BVH-CD group and our BVH group. Even though it has not been shown that residual vestibulo-ocular reflex (VOR) impacts CuS latencies, we also chose to match residual vestibular function across both groups, based on the mean VOR gain measured during vHIT of the lateral semicircular canals.
BVH-CD Group
Inclusion criteria were:
Cerebellar dysfunction:
Obvious cerebellar atrophy on MRI
At least one of the following clinical manifestations: postural and segmental cerebellar dysmetria, cerebellar dysarthria, specific cerebellar oculomotor disorders (at least one of the following: saccade hypermetria, downbeat nystagmus, obvious deficit of the visual inhibition of the visuo-vestibulo-ocular reflex)
Subjects were not included if they had other underlying central neurological condition, otological disorder other than vestibular hypofunction, corrected standard visual acuity lower than 5/10 Snellen equivalent, ocular motor palsy, ocular instability in primary gaze position, instability of the cervical spine, or if they were taking drugs interfering with eye movements.
A total of 12 subjects were included in the BVH-CD group. Ten patients had cerebellar ataxia neuronopathy and vestibular areflexia syndrome (CANVAS) with positive RFC1 testing. Two patients had chronic progressive cerebellar dysfunction associated with bilateral vestibular hypofunction, of unknown origin. Clinical manifestation of cerebellar oculomotor disorders as well as other clinical cerebellar manifestation are shown in Table 1.
Table 1 Clinical features of cerebellar manifestations of the 12 subjects of the BVH-CD group: J_SP, jerky smooth pursuit; J_VVOR, jerky visuo-vestibular reflex; GEN, gaze evoked nystagmus; DBN, down beat nystagmus; HS, hypermetric saccades; SWJ, square wave jerks; L_DyM, limb dysmetria; WG, wide gait; DyA, dysarthria; Ad, adiadochokinesiaBVH Group
Inclusion criteria were:
Exclusion criteria were similar to the other group with the exception of the exclusion in case of any underlying neurologic disorder.
A total of 12 subjects were included in the BVH group. Etiologies were the following: 5 idiopathic, 4 iatrogenic (aminoglycoside); 1 Meniere’s disease, 1 post infectious, 1 bilateral vestibular neuritis.
MaterialVideo Head Impulse Test (vHIT)
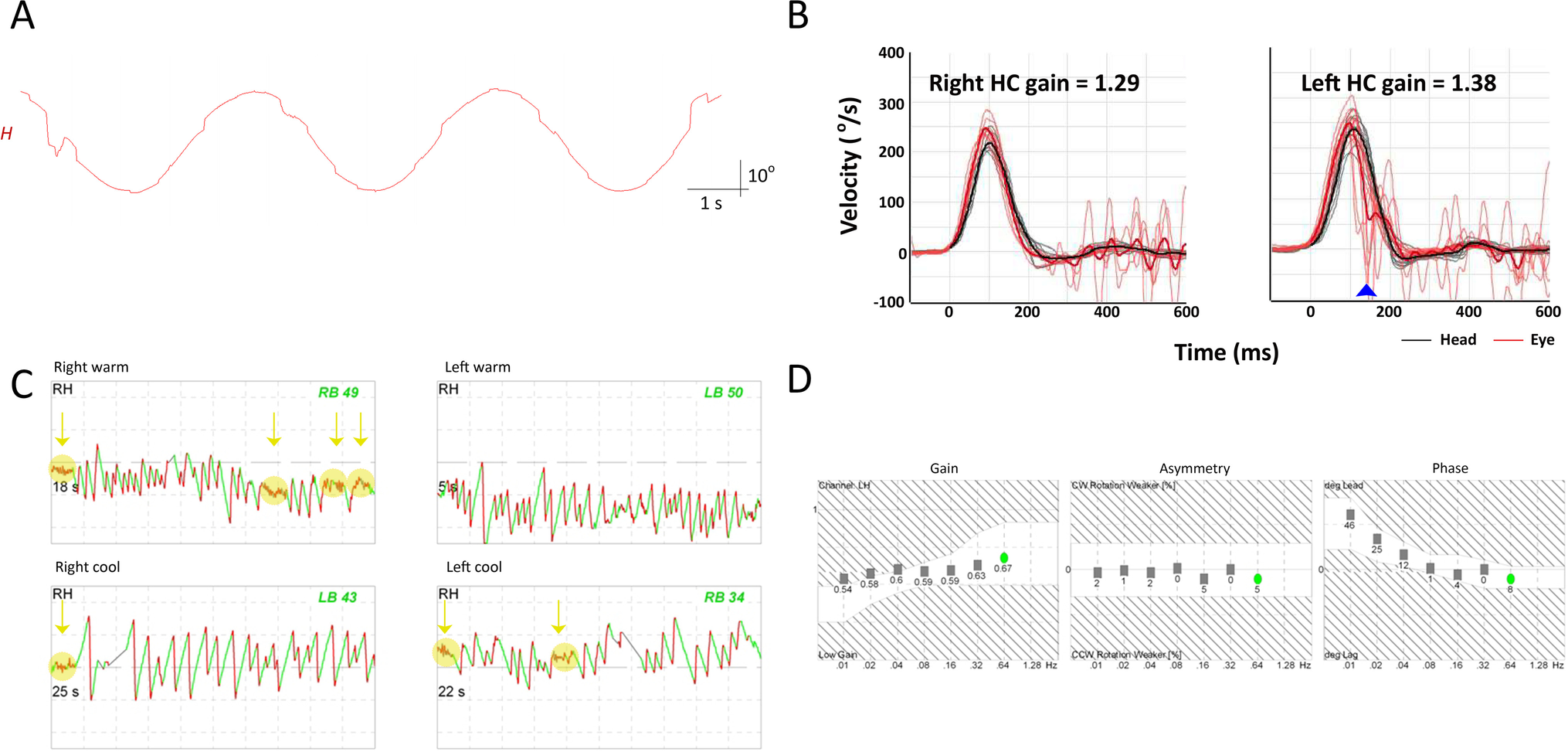
Head and eye movements during head impulse test were recorded using a lightweight portable vHIT device (Hardware: ICS Impulse, GN Otometrics, Taastrup, Denmark; Software: Otosuite Vestibular software). Head movements were recorded with a nine-axis motion sensor. Movements of the right eye were recorded with a high-velocity infrared camera. Both the head motion-sensor and eye camera were mounted on a lightweight frame and run at a 250 Hz sampling rate. The infrared camera was calibrated by having the subject gaze toward two light dots projected at eye level on the wall from built-in lasers.
Eye tracker
Visually guided saccades were recorded using high-velocity infrared cameras (EyeBRAIN® tracker now distributed by SURICOG Company, Paris, France). Movements of both eyes were recorded with a sampling rate of 300 Hz and an accuracy of 0.5°. Eye-tracker was calibrated with a build in 9-point calibration system.
MethodHead Impulse Test (vHIT)
This evaluation procedure has been described in details in a previous study[3]. In short, a single experienced examiner standing behind the subject performed outward horizontal impulses. Subjects had to gaze toward a target located 2 m in front of them. Their head was tilted forward to align the plane of their horizontal semicircular canals with the horizontal plane. A minimum of 10 valid horizontal head impulses (head speed > 200°/s) was achieved in each direction. Head and eye velocity data were then exported in CSS format for off line analysis.
Visually Guided Saccades (VGS)
Horizontal visually guided saccades were recorded in 3 different conditions: STEP, GAP, and OVERLAP. In all conditions, participants were seated in a dimly lit room facing a computer screen 60 cm in front of them. Their head was stabilized using a head and chin rest. For each trial, subjects first had to look at a dot in the center of the screen. Then they fixated a second dot as soon as it appeared at 12° or 20° from the central dot, either to the left or the right. After 1000 ms, the second dot disappeared, and the central dot appeared again for 2400 to 3600 ms until the next trial started.
For the STEP condition, the central dot disappeared at the same time as the second (lateral) dot appeared. For the GAP condition, the central dot disappeared 200 ms before the lateral dot appeared. For the OVERLAP condition, the central dot never disappeared. In each paradigm, twelve randomized outward saccades (6 to the left and 6 to the right) were recorded at 12° and at 20°. Thus, a total of 72 visually guided saccades were recorded.
Analysis of Head and Eye Movements
Data analysis for both vHIT and VGS was done in a program developed in our lab and running on MATLAB v.8.1 (MathWorks, MA, USA).
Details of the vHIT analysis have already been published [3]. In short, movements were first identified automatically and differentiated from artefacts by using a 5°/s head or eye velocity threshold. Then for each identified movement, five cursors defined, respectively, the starting and ending positions, the starting and ending times, and the time of maximum velocity. Each automatically detected movement was checked and cursors could be manually adjusted. In line with the previously described protocol, we chose to identify a maximum of three eye movements per head impulse (vestibulo-ocular reflex and up to 2 catch-up saccades). Covert saccades (CS) were defined as saccades occurring before the end of the head movement and overt saccades (OS) after the end of the head movement. The first catch-up saccades were defined as the first corrective saccade and could correspond to covert or overt saccades. For each head impulse, VOR gain was calculated as the amplitude ratio between eye movement and head movement at the end of VOR sequence. The end of the VOR sequence was defined as either the start of the covert saccade or the maximum point of VOR amplitude in case of absence of covert saccades. Saccadic gain was calculated as the ratio of eye movement amplitude during CS or OS and of total head movement amplitude. Latencies were calculated as the onset time of each eye movement (VOR, CS, OS) relative to the beginning of head movement. For each subject, the occurrence of CS (frequency in percent) was determined as the total number of CS relative to the total number of head impulses. The consistency of CS initiation was determined by the mean of individual standard deviation of the latency.
For visually guided saccades, analysis was done on both eyes. Eye movements were identified automatically by using an eye velocity threshold of 30°/s to differentiate movements from artefacts. Cursors were manually adjusted if necessary. We analyzed the latency, amplitude, and gain of primary saccades and only the amplitude and gain of secondary saccades by using the average between the values of both eyes. Gain was defined as the ratio between the actual saccade amplitude and the amplitude required to capture the target. Latency was defined as the difference in time between the appearance of the second dot and the beginning of the eye movement. Primary saccades measured in STEP condition were considered accurate if their amplitude was 12° + / − 1 for a target amplitude of twelve degrees or 20° + / − 2 for a target amplitude of twenty degrees; they were considered hypometric or hypermetric if their amplitude was below or above these thresholds, respectively.
Statistical Analysis
All data were stored and analyzed using JASP (JASP Team, Version 0.16.2, 2022). Statistical analyses were done using independent samples Student t test, Mann–Whitney test, or ANOVA depending on the normality of the distribution, as established by Shapiro–Wilk test, and the number of variables tested. All tests were two-tailed, and a statistical threshold p value < 0.05 was used.

留言 (0)