
記住我









Disclaimer: this video summarises a scientific article published by BMJ Publishing Group Limited (BMJ). The content of this video has not been peer-reviewed and does not constitute medical advice. Any opinions expressed are solely those of the contributors. Viewers should be aware that professionals in the field may have different opinions. BMJ does not endorse any opinions expressed or recommendations discussed. Viewers should not use the content of the video as the basis for any medical treatment. BMJ disclaims all liability and responsibility arising from any reliance placed on the content.
WHAT IS ALREADY KNOWN ABOUT THIS SUBJECTORAL Surveillance, which included patients with rheumatoid arthritis (RA) aged ≥50 years with ≥1 additional cardiovascular (CV) risk factor, was the first study to evaluate the safety of Janus kinase inhibitors in a CV risk-enriched RA population.
Primary findings indicated an increased risk of major adverse cardiovascular events (MACE) with tofacitinib versus tumour necrosis factor inhibitors (TNFi) (hazard ratio=1.33; 95% confidence interval (CI) 0.91 to 1.94). The non-inferiority criterion was not met (upper limit of 95% CI was >1.80).8
The increased risk of MACE with tofacitinib versus TNFi was more pronounced in patients aged ≥65 years than in patients aged <65 years.8
Risk of malignancies (excluding non-melanoma skin cancer) and infections was also higher with tofacitinib versus TNFi in ORAL Surveillance.8 26
WHAT THIS STUDY ADDSThis post hoc analysis of ORAL Surveillance shows an increased risk of MACE with tofacitinib 5 mg and 10 mg two times per day versus TNFi that was primarily observed in patients with a history of atherosclerotic cardiovascular disease (ASCVD; ie, history of coronary artery disease, cerebrovascular disease or peripheral artery disease) at baseline.
Risk of MACE did not appear different with tofacitinib 5 mg two times per day versus TNFi in patients without a history of ASCVD; but, given the exploratory nature of the analysis and the low event rate, we cannot rule out an increased risk of MACE in patients with several CV risk factors.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICYThis exploratory analysis of MACE in ORAL Surveillance underscores the value of including patients with a history of ASCVD for appropriate risk enhancement when investigating CV safety of RA treatments.
Our findings emphasise the importance of rheumatologists assessing overall CV risk, including medical history of ASCVD, when considering tofacitinib as a treatment for patients with RA.
IntroductionCompared with the general population, individuals with rheumatoid arthritis (RA) have a greater risk of cardiovascular (CV) disease.1 2 This is attributed to RA-associated systemic inflammation and traditional CV risk factors,2–7 and both require effective control to mitigate the risk. The European Alliance of Associations for Rheumatology (EULAR) recommends regular CV risk assessments in patients with RA using validated risk prediction models.2
ORAL Surveillance was a post-authorisation safety study conducted, in part, due to observations of increased serum lipid levels with the Janus kinase inhibitor, tofacitinib.8–10 The study was the first to evaluate the relative risk of adjudicated major adverse cardiovascular events (MACE) and malignancies with tofacitinib versus tumour necrosis factor inhibitors (TNFi) in patients with RA aged ≥50 years with ≥1 additional CV risk factor. For combined tofacitinib doses (5 mg and 10 mg two times per day) versus TNFi, non-inferiority was not shown for adjudicated MACE (incidence rate (IR) of 0.98 per 100 patient-years, 95% CI 0.79 to 1.19, versus IR of 0.73 per 100 patient-years, 95% CI 0.52 to 1.01; hazard ratio (HR)=1.33, 95% CI 0.91 to 1.94).8 For context, in the ENTRACTE study of patients with RA aged ≥50 years with ≥1 CV risk factor, rates of MACE per 100 patient-years were 1.70 with etanercept and 1.82 with tocilizumab.11
ORAL Surveillance included patients with RA and other risk factors that impact absolute risk of MACE,8 and this CV-risk enriched population likely reflected a spectrum of CV risk. Guidelines on CV disease prevention distinguish between patients with or without atherosclerotic CV disease (ASCVD).12 ASCVD includes a history of coronary artery disease (CAD), which was one of the eligibility criteria for the study, but also cerebrovascular disease (CeVD) and peripheral artery disease (PAD) (table 1).12 13 Patients with ASCVD are generally considered to have high to very high absolute risk of MACE.12 In recent CV outcome trials of patients with type 2 diabetes, MACE IRs in placebo-treated patients with ASCVD were 4.0–6.5 per 100 patient-years, compared with 1.3–3.3 per 100 patient-years, in patients without ASCVD but with multiple CV risk factors.14 Here, we further evaluate risk of MACE with tofacitinib versus TNFi in the ORAL Surveillance overall population, and in patients with or without a history of ASCVD.
Table 1ASCVD is defined based on events, diagnoses and procedures associated with atherosclerosis in arteries of the heart, head and neck and the periphery
MethodsStudy design and patientsORAL Surveillance (NCT02092467) was a phase IIIb/IV randomised, open-label, non-inferiority, safety endpoint study conducted from March 2014 to July 2020 in patients with active moderate-to-severe RA despite methotrexate treatment who were aged ≥50 years with ≥1 additional CV risk factor (current smoking, hypertension, high-density lipoprotein cholesterol (HDL-c) <40 mg/dL, diabetes mellitus, family history of premature coronary heart disease (CHD), RA-associated extra-articular disease and/or history of CAD).8
Patients were randomised 1:1:1 to receive oral tofacitinib 5 mg or 10 mg two times per day, or subcutaneous TNFi (adalimumab 40 mg every 2 weeks (North America) or etanercept 50 mg once weekly (rest of the world)). All patients continued their prestudy stable dose of methotrexate unless modification was clinically indicated. In February 2019, the tofacitinib 10 mg two-times-per-day dose was reduced to 5 mg two times per day after the Data Safety Monitoring Board noted an increased frequency of pulmonary embolism in patients receiving tofacitinib 10 mg two times per day versus TNFi and an increase in overall mortality with tofacitinib 10 mg versus 5 mg two times per day and TNFi.
Evaluation of history of ASCVD and baseline CV riskA history of ASCVD was defined as the composite of history of CAD, CeVD and PAD. A history of CAD was an eligibility criterion in ORAL Surveillance (reported as ≥one of history of myocardial infarction (MI), unstable angina, stable angina pectoris, coronary artery procedures or other CHD).8 A history of CeVD (including ischaemic stroke and transient ischaemic attack) and PAD was identified in patients’ general medical history through Medical Dictionary for Regulatory Activities’ preferred terms (online supplemental table 1).
In patients without a history of ASCVD, 10-year risk of events associated with ASCVD (ie, MACE) was calculated by ASCVD-Pooled Cohort Equations (ASCVD-PCE).15 Scores werecalculated based on patients’ baseline age, sex, race (white/black/other), smoking status (yes/no), systolic blood pressure, antihypertensive treatment (yes/no), total cholesterol, HDL-c and diabetes (yes/no). In line with EULAR recommendations, a 1.5 multiplier was applied to all ASCVD-PCE scores.2 Based on the resulting scores, and as suggested by the American College of Cardiology/American Heart Association,16 patients without a history of ASCVD were assigned to the following 10-year risk categories: high (≥20%), intermediate (≥7.5–<20%), borderline (≥5–<7.5%) and low (<5%).
OutcomesMACE and its components were based on adjudicated events assessed by an external, independent adjudication committee. MACE was defined as the composite of CV death (ie, death due to MI, stroke, sudden cardiac death, heart failure, CV procedures, CV haemorrhage and other CV causes, but not death due to pulmonary embolism), non-fatal MI and non-fatal stroke (including reversible focal neurological defects with imaging evidence of a new cerebral lesion consistent with ischaemia or haemorrhage).
Statistical analysesOutcomes were analysed using the safety analysis set, which included all randomised patients receiving ≥1 dose of study drug. For patients randomised to tofacitinib 10 mg two times per day who had their dose reduced to 5 mg two times per day in February 2019, the data collected after the dose switch were counted in the tofacitinib 10 mg two-times-per-day group.
CV events were counted within the predefined risk period, based on 60-day on-treatment time, defined as time from first to last study dose +60 days or to last contact date (if a patient died, last contact date was death date), whichever was earliest. Patients without events were censored at the end of the risk period.
Crude IRs were expressed as the number of patients with first events per 100 patient-years, along with two-sided 95% CIs using the exact Poisson method.17 HRs and two-sided 95% CIs for pairwise comparisons among treatment groups (tofacitinib doses vs TNFi) were estimated using Cox proportional hazard regression models.
Subgroup analyses were conducted to assess for an association between history of ASCVD or baseline risk of MACE (ie, categories of CV risk in patients without history of ASCVD) with risk (HRs and IRs) of MACE, MI and stroke with tofacitinib versus TNFi. Across these exploratory analyses, no multiplicity adjustments were applied. Statistical analyses of treatment by history of ASCVD interactions are described in the online supplemental material.
The number needed to harm (NNH) was calculated as the reciprocal of the difference in IRs between tofacitinib and TNFi.18 Positive NNH was defined as patient-years of tofacitinib exposure needed for one more patient to report an additional event versus TNFi. Negative NNH was defined as the reverse. When the 95% CI of the IR difference includes 0, the 95% CI of the NNH has 2 disjoint (positive and negative) intervals, implying harm in either tofacitinib versus TNFi (positive) or TNFi versus tofacitinib (negative). NNH for patients exposed for 5 years was calculated by dividing the number of patient-years needed to harm by 5.
Patient and public involvementPatients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
ResultsPatientsIn total, 4362 patients were randomised and treated(tofacitinib 5 mg two times per day, n=1455; tofacitinib 10 mg two times per day, n=1456; TNFi, n=1451). Median follow-up was 4.0 years; 3111/4362 (71.3%) patients completed the trial and 2745/4362 (62.9%) completed trial treatment.8 Full patient demographics and baseline disease characteristics are described elsewhere.8 Table 2 summarises CV risk factors and the CV risk profile (online supplemental figure 1) of the study population versus patients with and without a history of ASCVD. These were well-balanced across treatment groups in ORAL Surveillance; 14.7% (640/4362) of patients had a history of ASCVD. Patients with a history of ASCVD were more likely to be ≥65 years, male, past smokers and have a history of diabetes mellitus, hypertension or hyperlipidaemia, compared with those with no history of ASCVD (table 2).
Table 2Demographic and baseline disease characteristics in the ORAL Surveillance overall population and in patients with and without a history of ASCVD
Risk of adjudicated MACE outcomes with tofacitinib versus TNFi in ORAL SurveillanceRisk of MACE, MI and sudden cardiac death were increased with both tofacitinib doses versus TNFi as reflected by HRs >1.0 and higher IRs (figure 1 and online supplemental figure 2). Risk of non-fatal MI with tofacitinib 5 mg two times per day versus TNFi was noticeably increased (HR=2.32; 95% CI 1.02 to 5.30; figure 1). Stroke HRs and IRs across treatment groups are shown in figure 1 and online supplemental figure 2.
 Figure 1
Figure 1 Adjudicated MACE outcomes with tofacitinib versus TNFi in ORAL Surveillance. HRs are shown on a logarithmic scale. Arrows indicate that the CI extends beyond the graph axis. For patients randomised to the tofacitinib 10 mg two-times-per-day group who had their dose of tofacitinib reduced to 5 mg two times per day, the data collected after patients were switched to tofacitinib 5 mg two times per day were counted in the tofacitinib 10 mg two-times-per-day group. HRs (95% CIs) are based on two simple Cox proportional hazard models (one for comparing combined tofacitinib doses vs TNFi, and the other for comparing tofacitinib 5 mg and 10 mg two times per day vs TNFi), with treatment as the only covariate. HRs and 95% CIs were NI when the total number of patients with events was ≤2 for the corresponding pair of treatments in the comparison or when one of the treatments in the comparison had 0 events. IRs express number of patients with first events per 100 PY. †Results reported in Ytterberg et al 8 and included for reference. *HR 95% CI excludes 1. BID, two times per day; CI, confidence interval; CV, cardiovascular; HR, hazard ratio; IR, incidence rate; MACE, major adverse cardiovascular events; MI, myocardial infarction; n, number of patients with events; N, number of evaluable patients; NI, non-informative; PY, patient-years; TNFi, tumour necrosis factor inhibitor.
Across treatment groups, the most frequent cause of CV death was sudden cardiac death (figure 1). One patient had fatal heart failure (tofacitinib 10 mg two times per day), and one died of other CV causes (TNFi).
HRs for MACE with tofacitinib versus TNFi in a total time analysis, including all events up to last contact date regardless of when study drug was discontinued, were consistent with the primary analysis (online supplemental figure 3). MACE IRs by 6-month intervals are shown in online supplemental figure 4.
Risk of MACE with tofacitinib versus TNFi according to a history of ASCVDAmong patients with a history of ASCVD, MACE was reported in 17/204 (8.3%), 17/222 (7.7%) and 9/214 (4.2%) of patients in the tofacitinib 5 mg two-times-per-day, tofacitinib 10 mg two-times-per-day and TNFi treatment groups, respectively. MACE HRs (95% CI) were 1.96 (0.87 to 4.40) for tofacitinib 5 mg two times per day versus TNFi, 2.01 (0.89 to 4.50) fortofacitinib 10 mg two times per day versus TNFi and 1.98 (0.95 to 4.14) for combined tofacitinib doses versus TNFi (figure 2A and online supplemental figure 5). Based on the IR differences, this corresponds to NNH of 16 (95% CI −∞ to −91 and 7 to ∞) and 15 (95% CI −∞ to −117 and 7 to ∞) patients who would need to be treated with tofacitinib 5 mg and 10 mg two times per day, respectively, versus TNFi, over 5 years to have 1 additional MACE (figure 2A; online supplemental table 2).
 Figure 2
Figure 2 Risk of MACE with tofacitinib versus TNFi by history of ASCVD. (A) HRs (95% CIs) are based on two simple Cox proportional hazard models (one for comparing combined tofacitinib doses versus TNFi, and the other for comparing tofacitinib 5 mg and 10 mg two times per day vs TNFi), with treatment as the only covariate. IRs express number of patients with first events per 100 PY. NNH (PY) should be interpreted as the number of PY of exposure to tofacitinib required to have one additional MACE versus TNFi. NNH (5-year) should be interpreted as the number of patients who would need to be treated for that duration with tofacitinib rather than with a TNFi to result in one additional MACE. *IRD 95% CI excluded 0. †Results reported in Ytterberg et al 8 and included for reference. ‡NNH 95% CIs are reported in online supplemental table 2. (B) Treatment-by-HxASCVD interaction p values for HRs (χ2 test with 1 degree of freedom) and IRD (2-sided, normal approximation of difference in IR). See supplementary material for details. (C) Cumulative probability of patients with adjudicated MACE events, calculated based on the Kaplan-Meier estimate, in patients with history of ASCVD (left panel) and without history of ASCVD (right panel). HRs are shown on a logarithmic scale. Arrows indicate that the CI extends beyond the graph axis. For patients randomised to the tofacitinib 10 mg two-times-per-day group who had their dose of tofacitinib reduced to 5 mg two times per day, the data collected after patients were switched to tofacitinib 5 mg two times per day were counted in the tofacitinib 10 mg two-times-per-day group. BID, two times per day; CI, confidence interval; CV RF, cardiovascular risk factor; HR, hazard ratio; HxASCVD, history of atherosclerotic cardiovascular disease; IR, incidence rate; IRD, incidence rate difference; MACE, major adverse cardiovascular events; n, number of patients with events; N, number of evaluable patients; NNH, number needed to harm; PY, patient-years; TNFi, tumour necrosis factor inhibitor.
In patients without a history of ASCVD but with CV risk factors, MACE was reported in 30/1251 (2.4%), 34/1234 (2.8%) and 28/1237 (2.3%), in the tofacitinib 5 mg two-times-per-day, tofacitinib 10 mg two-times-per-day and TNFi treatment groups, respectively (figure 2A). HRs (95% CI) for MACE were 1.03 (0.62 to 1.73) for tofacitinib 5 mg two times per day versus TNFi, 1.25 (0.76 to 2.07) for tofacitinib 10 mg two times per day versus TNFi and 1.14 (0.73 to 1.78) for combined tofacitinib doses versus TNFi (figure 2A and online supplemental figure 5). Based on the IR differences, this corresponds to NNH of 869 (95% CI −∞ to −64 and 55 to ∞) and 124 (95% CI −∞ to −100 and 38 to ∞) patients who would need to be treated with tofacitinib5 mg and 10 mg two times per day, respectively, versus TNFi, over 5 years to have 1 additional MACE (figure 2A; online supplemental table 2). P values for the treatment by history of ASCVD interaction (combined tofacitinib doses vs TNFi) for MACE were 0.196 for the HRs and 0.059 for the IR difference (figure 2B).
Kaplan-Meier curves for MACE (figure 2C) indicated separation between the tofacitinib and TNFi groups by month 3 in patients with history of ASCVD, and no separation between treatment groups in patients without history of ASCVD.
Risk of MI and stroke with tofacitinib versus TNFi according to history of ASCVDIn patients with a history of ASCVD, treatment with tofacitinib5 mg or 10 mg two times per day was associated with increased risk of MI and stroke versus TNFi (figure 3 and online supplemental figure 5). Risk of MI was also increased with tofacitinib versus TNFi in patients without a history of ASCVD (figure 3 and online supplemental figure 5). In the assessment of MI and stroke according to history of ASCVD, the number of events overall was low, and these results should be interpreted with caution.
 Figure 3
Figure 3 Risk of MI and stroke with tofacitinib versus TNFi by history of ASCVD. (A) HRs are shown on a logarithmic scale. Arrows indicate that the CI extends beyond the graph axis. For patients randomised to the tofacitinib 10 mg two-times-per-day group who had their dose of tofacitinib reduced to 5 mg two times per day, the data collected after patients were switched to tofacitinib 5 mg two times per day were counted in the tofacitinib 10 mg two-times-per-day group. HRs (95% CIs) are based on two simple Cox proportional hazard models (one for comparing combined tofacitinib doses vs TNFi, and the other for comparing tofacitinib 5 mg and 10 mg two times per day vs TNFi), with treatment as the only covariate. IRs express the number of patients with first events per 100 PY. (B) Treatment-by-HxASCVD interaction p values for HRs (χ2 test with 1 degree of freedom) and IRD (two-sided, normal approximation of difference in IR). See supplementary material for details. BID, two times per day; CI, confidence interval; CV RF, cardiovascular risk factor; HxASCVD, history of atherosclerotic cardiovascular disease; IR, incidence rate; IRD, incidence rate difference; MI, myocardial infarction; n, number of patients with events; N, number of evaluable patients; PY, patient-years; TNFi, tumour necrosis factor inhibitor.
Association between baseline CV risk scores and risk of MACE, MI and stroke with tofacitinib versus TNFi in patients without a history of ASCVDPatients without a history of ASCVD were grouped by their 10-year risk of MACE.2 MACE IRs, regardless of treatment group, were highest in patients at high risk (ie, ≥20% 10-year risk of MACE) (figure 4 and online supplemental figure 6). There was no difference in risk of MACE with tofacitinib 5 mg or 10 mg two times per day versus TNFi in patients at high or intermediate risk. While HRs for tofacitinib versus TNFi were >1.0 in patients with low or borderline risk, the number of events was low.
 Figure 4
Figure 4 Risk of MACE with tofacitinib versus TNFi in patients without a history of ASCVD, according to CV risk categories. HRs are shown on a logarithmic scale. Arrows indicate that the CI extends beyond the graph axis. Patients without HxASCVD were categorised according to their 10-year risk of MACE, per the ASCVD-PCE risk calculator. In line with EULAR recommendations, a 1.5 multiplier was applied to all ASCVD-PCE scores.2 Because of missing ASCVD-PCE score, two MACE could not be associated with baseline CV risk (n=1 (MI) in the tofacitinib 5 mg two-times-per-day group and n=1 (stroke) in the tofacitinib 10 mg two-times-per-day group). For patients randomised to the tofacitinib 10 mg two-times-per-day group who had their dose of tofacitinib reduced to 5 mg two times per day, the data collected after patients were switched to tofacitinib 5 mg two times per day were counted in the tofacitinib 10 mg two-times-per-day group. HRs (95% CIs) are based on two simple Cox proportional hazard models (one for comparing combined tofacitinib doses vs TNFi, and the other for comparing tofacitinib 5 mg and 10 mg two times per day vs TNFi), with treatment as the only covariate. IRs express the number of patients with first events per 100 PY. †Results reported in Ytterberg et al 8 and included for reference. ASCVD-PCE, atherosclerotic cardiovascular disease-Pooled Cohort Equations; BID, two times per day; CI, confidence interval; CV, cardiovascular; EULAR, European Alliance of Associations for Rheumatology; HxASCVD, history of atherosclerotic cardiovascular disease; IR, incidence rate; MACE, major adverse cardiovascular events; n, number of patients with events; N, number of evaluable patients; PY, patient-years; TNFi, tumour necrosis factor inhibitor.
MI IRs were highest in patients with a high CV risk score (figure 5 and online supplemental figure 7). There was an increased risk of MI with tofacitinib 5 mg two times per day versus TNFi in patients with high 10-year risk of MACE. There were fewer MIs reported in the other risk categories.
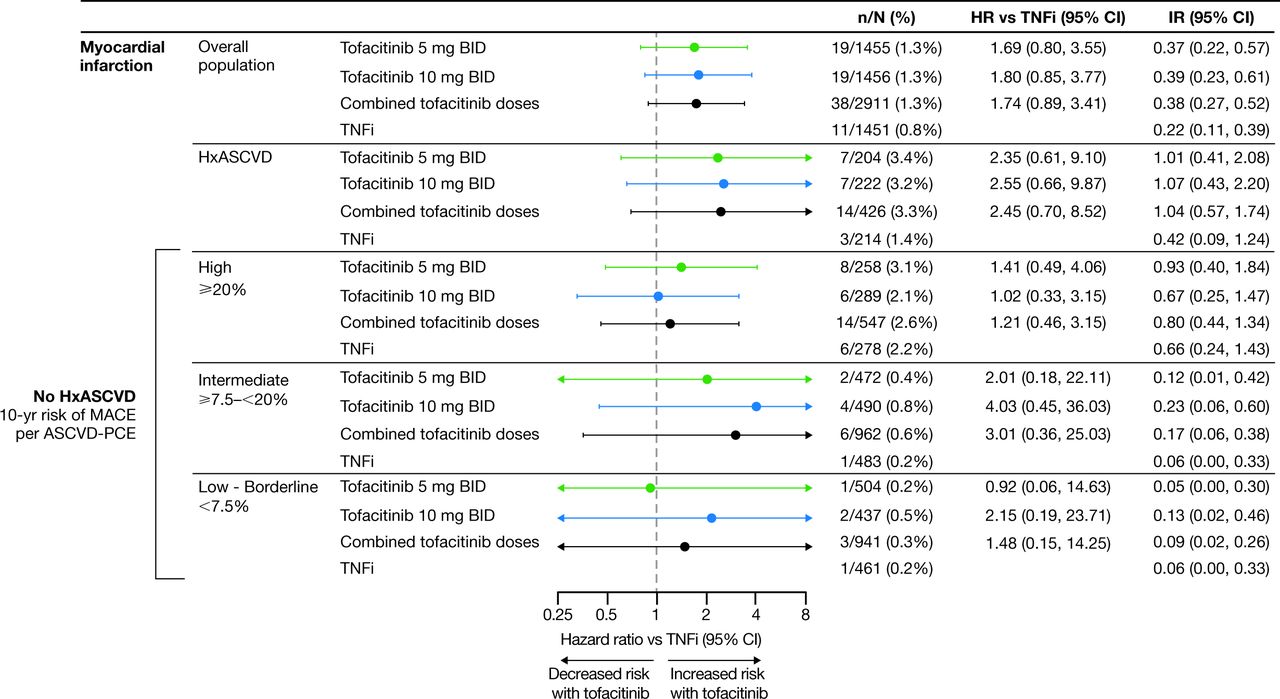 Figure 5
Figure 5 Risk of MI with tofacitinib versus TNFi in patients without history of ASCVD, according to CV risk categories. HRs are shown on a logarithmic scale. Arrows indicate that the CI extends beyond the graph axis. Patients without HxASCVD were categorised according to their 10-year risk of MACE, per the ASCVD-PCE risk calculator. In line with EULAR recommendations, a 1.5 multiplier was applied to all ASCVD-PCE scores.2 Because of missing ASCVD-PCE score, one MI in the tofacitinib 5 mg two-times-per-day group could not be associated with baseline CV risk. For patients randomised to the tofacitinib 10 mg two-times-per-day group who had their dose of tofacitinib reduced to 5 mg two times per day, the data collected after patients were switched to tofacitinib 5 mg two times per day were counted in the tofacitinib 10 mg two-times-per-day group. HRs (95% CIs) are based on two simple Cox proportional hazard models (one for comparing combined tofacitinib doses vs TNFi, and the other for comparing tofacitinib 5 and 10 mg two times per day vs TNFi), with treatment as the only covariate. IRs express the number of patients with first events per 100 PY. ASCVD-PCE, atherosclerotic cardiovascular disease-Pooled Cohort Equations; BID, two times per day; CI, confidence interval; CV, cardiovascular; EULAR, European Alliance of Associations for Rheumatology; HR, hazard ratio; HxASCVD, history of atherosclerotic cardiovascular disease; IR, incidence rate; MACE, major adverse cardiovascular events; MI, myocardial infarction; n, number of patients with events; N, number of evaluable patients; PY, patient-years; TNFi, tumour necrosis factor inhibitor.
The association between baseline CV risk and stroke IRs was less apparent than observed for MACE and MI (figure 6 and online supplemental file 8). Overall, event numbers in each risk category were low.
 Figure 6
Figure 6 Risk of stroke with tofacitinib versus TNFi in patients without a history of ASCVD, according to CV risk categories. HRs are shown on a logarithmic scale. Arrows indicate that the CI extends beyond the graph axis. Patients without history of ASCVD were categorised according to their 10-year risk of MACE, per the ASCVD-PCE risk calculator. In line with EULAR recommendations, a 1.5 multiplier was applied to all ASCVD-PCE scores.2 Because of missing ASCVD-PCE score, one stroke in the tofacitinib 10 mg two-times-per-day group could not be associated with baseline CV risk. For patients randomised to the tofacitinib 10 mg two-times-per-day group who had their dose of tofacitinib reduced to 5 mg two times per day, the data collected after patients were switched to tofacitinib 5 mg two times per day were counted in the tofacitinib 10 mg two-times-per-day group. HRs (95% CIs) are based on two simple Cox proportional hazard models (one for comparing combined tofacitinib doses versus TNFi, and the other for comparing tofacitinib 5 mg and 10 mg two times per day vs TNFi), with treatment as the only covariate. IRs express the number of patients with first events per 100 PY. ASCVD-PCE, atherosclerotic cardiovascular disease-Pooled Cohort Equations; BID, two times per day; CV, cardiovascular; EULAR, European Alliance of Associations for Rheumatology; HxASCVD, history of atherosclerotic cardiovascular disease; IR, incidence rate; MACE, major adverse cardiovascular events; n, number of patients with events; N, number of evaluable patients; PY, patient-years; TNFi, tumour necrosis factor inhibitor.
DiscussionPrimary analyses of ORAL Surveillance, which included patients aged ≥50 years with ≥1 additional CV risk factor and was the first study to evaluate tofacitinib safety in a CV risk-enriched RA population, found an increased risk of MACE with tofacitinib versus TNFi.8 In this post hoc analysis, increased risk of MACE was primarily identified in patients with a history of ASCVD (ie, pre-existing CAD, CeVD or PAD). In patients without a history of ASCVD but with CV risk factors, there did not appear to be a detectable difference in risk of MACE with tofacitinib 5 mg two times per day or the combined tofacitinib doses versus TNFi.
ORAL Surveillance was powered to assess non-inferiority for risk of MACE with combined tofacitinib doses versus TNFi and not powered to compare individual MACE components across treatment groups.8 The exploratory analyses on CV outcomes and subgroup analyses we provide, therefore, need to be interpreted cautiously and as hypothesis-generating. Notwithstanding, our analysis of the overall study population supplements the primary analysis of the study and shows increased risk of MI and sudden cardiac death with tofacitinib versus TNFi in this CV risk-enriched population.
Almost 15% of the patients in ORAL Surveillance had a history of ASCVD. In this subgroup, we found increased risk of MACE, MI and stroke with tofacitinib versus TNFi. In the remaining 85% of patients without a history of ASCVD, who nevertheless had CV risk factors, we did not find increased relative risk of MACE with tofacitinib versus TNFi. This observation is supported by our assessment of relative risk across categories of predicted MACE risk; there was no clear difference in risk of MACE in patients without a history of ASCVD who had high (≥20%) or intermediate (≥7.5–<20%) predicted 10-year risk at baseline. Approximately one-third of the ORAL Surveillance population had low or borderline absolute risk of MACE, and the low number of MACE in this group makes assessment of relative risk less certain.
A large observational study that used USA claims data to assess risk of CV outcomes (composite of hospitalisation for MI or stroke) with tofacitinib versus TNFi in patients with RA (Safety of TofAcitinib in Routine care patients with Rheumatoid Arthritis; STAR-RA) was recently published.19 Evidence for an increased risk of CV outcomes with tofacitinib was not identified in this real-world evidence cohort. However, STAR-RA included a cohort that mirrored ORAL Surveillance inclusion and exclusion criteria (randomised controlled trial (RCT)-duplicate cohort). The primary outcome of the RCT-duplicate cohort aligned with the increased risk of MACE with tofacitinib versus TNFi observed in ORAL Surveillance (ie, approximately 25% relative risk increase with tofacitinib 5 mg two times per day vs TNFi).8 19 STAR-RA also prespecified subgroup analyses of patients with or without previous CV disease. These results were also similar to ORAL Surveillance; risk of CV outcomes appeared to be increased with tofacitinib versus TNFi in patients with, but not in those without, pre-existing CV disease.19
Our analysis of MACE in ORAL Surveillance underscores the importance of investigating the long-term safety of RA treatments in appropriately designed, prospective, randomised and comparative trials of sufficient size and duration to adequately evaluate safety events of interest, including CV adverse events. Consequently, for ORAL Surveillance to be declared complete, ≥1500 patients had to be followed for 3 years and the study was conducted in a CV risk-enriched population to ensure accumulation of a sufficient number of CV events. To the best of our knowledge, the only similar studies in RA are the ENTRACTE and PRECISION trials that assessed CV safety of tocilizumab versus etanercept and celecoxib versus naproxen versus ibuprofen, respectively.11 20 In ENTRACTE and PRECISION, 11% (347/3080) and 24% (584/2436) of patients with RA had previous CV disease
留言 (0)