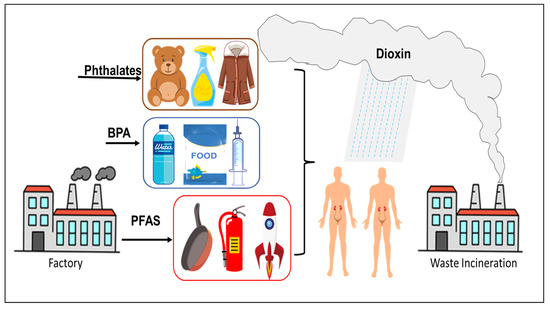
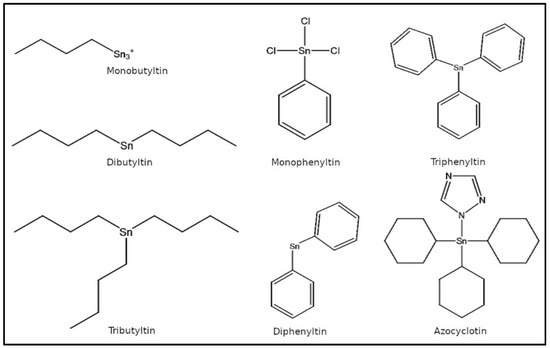
Per- and polyfluoroalkyl substances are a class of chemicals (
Figure 2b) used in many industrial and consumer products with the main function of resisting heat, stains, water, and grease [
62,
63]. Classic examples include Teflon, coating on fast-food wrappers, non-stick pans, floor polish, carpets, furniture fabrics, firefighting foams, clothing treatments, and many others [
64,
65]. It has been estimated that over 98% of Americans have these chemicals in their body [
66,
67,
68,
69]. PFAS can be classified into long chain and short chain chemicals based on the number of carbon atoms (usually between 4 and 12) and they have a long half-life and are difficult to metabolize (because of the strong covalent C–F bond). In general, shorter chain chemicals (n ≤ 6) are easier to excrete than longer chain chemicals (n ≥ 6). Previous studies have found that urine was the main mode of excretion of PFAS in mice and monkeys [
70,
71]. High concentrations of PFAS were detected in human urine, and renal excretion in humans and accounts for approximately one-fifth of the total excretion based on their serum half-lives [
72,
73]. Analysis of blood and urine samples from adults showed that a variety of PFAS were detected, including perfluorooctane sulfonates (PFOS), perfluorooctanoic acid (PFOA), perfluorononanoate (PFNA), perfluorohexanesulfonic acid (PFHxS), and perfluorinated decanoic acid (PFDA), and that the level of PFAS in urine was positively correlated with that in blood [
74]. 3.1. Accumulation of PFAS in the KidneyRenal excretion is an important excretory pathway of PFAS in humans and animals, and the kidney plays an essential role in the metabolism and transport of PFAS. After exposure to PFAS in rainbow trout, the degree of accumulation was blood > kidney > liver > gallbladder [
75,
76]. The distribution of 24 types of PFAS in eight different tissues of Orcinus orca was reported, and the highest concentration of PFAS was found in the liver, followed by the blood and kidney [
77]. PFAS were measured in samples from 31 harbor porpoises (Phocoena relicta) stranded on the Black Sea coast and PFOS was found to account for 90% of all PFAS, which were highest in the liver (327 ± 351 ng/g wet weight) and kidney (147 ± 262 ng/g wet weight) tissues [
78]. Both long-chain and short-chain PFAS were also detected in the organs and tissues of the sea leopard (Phoca vitulina) in the Netherlands [
79,
80]. In another study, PFAS accumulation in the tissues and organs of the Baltic guillemots (Uria algge) were noted. PFOS remained the most abundant, with a median concentration of 127 ng/g weight in the kidney [
81]. The distribution of 16 PFAS in the liver, blood, kidney, adipose tissue, and muscle of 18 Arctic foxes aged 1–3 years was also noted, with the concentration of PFAS being highest in the liver, followed by the blood and kidney [
82]. These data suggest that the tissue distribution and accumulation patterns of PFAS in organisms vary considerably. However, the kidney has always been an important organ for PFAS accumulation in animal species. Compared with long-chain PFAS, short-chain PFAS (e.g., perfluorobutyric acid, PFBA) have a relatively short half-life in blood and do not accumulate at high levels in human kidney tissue based on the analysis of seven lung and nine kidney samples from cancer patients [
83]. Since studies on kidney toxicology are sparse, this makes a strong argument for investigations on chronic exposure in relation to accumulation and kidney diseases. 3.2. Relationship between PFAS and CKDPFAS are ubiquitous and difficult to metabolize, and thus, their possible toxic effects on animals and humans have attracted significant attention [
84,
85,
86,
87,
88,
89,
90]. However, some studies suggest that there may be no causal relationship between chronic kidney disease (CKD) and PFAS. To investigate the longitudinal association between PFOA and PFOS exposure and the incidence of CKD in patients with diabetes, PFOA and PFOS levels in serum were measured in nearly 1000 patients with diabetes and it was found that PFOS levels were significantly associated with a lower risk of CKD incidence. The interaction between PFOA and PFOS exposure and CKD was not statistically significant [
91]. In a study of 73 normal weight pregnant women who did not have gestational diabetes mellitus or preeclampsia, the concentration of PFNA, PFOA, PFOS, and PFHxS in the blood changed from early to late pregnancy. The levels of these PFAS decreased during pregnancy, but were not linked to changes in the estimated glomerular filtration rate (eGFR) or glomerular pore size. Collectively, these studies suggest that changes in renal function are not caused by PFAS [
92].On the contrary, other studies have shown that PFAS was closely related to a decline in renal function. EGFR was one of the diagnostic factors of CKD, and studies have shown that PFAS can affect the level of eGFR. PFAS levels in 61 CKD patients were found to be significantly higher than in the healthy control group [
93]. The levels of hemoglobin, serum albumin, and eGFR were significantly lower while the levels of potassium and uric acid were higher in the CKD group. PFOS levels were found to be significantly higher in CKD patients than controls. By measuring serum concentrations of PFOA, PFOS, PFNA, and PFHxS in adolescents living near chemical plants and comparing their eGFR with another 10,000 adolescents, the association between eGFR and serum PFOA might serve as an indicator of decreased renal function [
94]. Serum samples from 53,650 adults (5210 with diabetes) were evaluated for four different PFAS. All PFAS had a strong positive correlation with eGFR in patients with CKD or anemia, and these relationships were more significantly associated in patients with diabetes. PFAS are inversely associated with renal function in CKD and diabetes, suggesting that exposure to PFAS could be associated with decreased renal function [
95,
96,
97,
98]. After following 1237 non-diabetic women aged 45 to 56 years until 2017, a study by Park [
99] suggested that PFAS may increase the risk of diabetes in middle-aged women. 3.3. Effect of PFAS on RCC and Renal FunctionSeveral discrepancies exist in studies on the association between PFAS and kidney cancer. Reports from 18 epidemiological studies on the association between PFOS exposure and human cancer risk indicated that the relative risks of PFOA and PFOS do not indicate a dose–response relationship between exposure and kidney cancer. Positive associations with PFOA exposure were detected in community settings, but because occupational exposure to PFOS was one to two orders of magnitude higher than environmental exposure, epidemiologic evidence does not support the hypothesis of a causal dose–response relationship between PFOS exposure and human cancer [
100].In contrast, other studies have demonstrated that the kidney was one of the target organs of PFAS. Data from 324 patients showed that a doubling of serum PFOA concentration was associated with an approximately 70% increase in RCC risk when PFAS concentrations were serially simulated. Higher concentrations of certain PFAS and the highest incidence of RCC were also observed in African Americans compared to non-Hispanic whites [
101,
102]. This study was also supported by the study from Steenland et al. [
103], in which the association between PFOA and RCC was examined in nearly 1000 renal cancer cases. The pooled analysis indicated that PFOA was associated with renal cancer in human studies, for every 1 ng/mL increase of serum PFOA, the logarithmic ratio of RCC increased by 0.1349. These results provide strong evidence that PFOA is a renal carcinogen.Since the association between PFOA and RCC has yielded conflicting conclusions in different studies, PFOA exposure was converted to serum PFOA concentrations and meta-analysis was used to estimate cancer risk. In the meta-analysis, risk for RCC rose 16% for each 10 ng/mL increase in serum PFOA. Thus, the association of PFOA with RCC is most likely causal and makes a strong argument for further research on the mechanisms underlying this association [
104].Recently, studies are beginning to emerge on the effect of PFAS in select cancers (liver, prostate, kidney, etc.) [
105], but mechanistic studies on the role of PFAS are sparse. Although epidemiological evidence points to kidney cancer as one of the cancers triggered by PFAS, very few studies have examined the role of PFAS in kidney disease or renal cell carcinoma.A study by Park [
106] showed that after being absorbed by the human body, PFAS are first combined with serum proteins and then deposited in various organs of the body such as the liver, kidney, and testis, and that PFAS cannot be excreted, resulting in a variety of toxic outcomes. The effect of PFAS on gap junctional intercellular communication (GJIC) in a dolphin renal epithelial cell line showed that PFOS, perfluorooctane sulfonamide (PFOSA) and perfluorohexane sulfonic acid (PFHA) could rapidly inhibit GJIC, while perfluorobutane sulfonic acid (PFBS) had no significant effect on GJIC. In humans, urinary excretion of short-chain PFAS was found to be higher, whereas other elimination pathways were found to be more dominant for long-chain chemicals [
107,
108]. These results suggest that the toxic effects of PFAS on organisms could possibly depend on its structure rather than the properties of its functional groups.Only a few studies exist on the mechanism of PFAS exposure and kidney response. Examination of over 70 studies studies in the fields of epidemiology, pharmacokinetics, and toxicology showed that PFAS exposure causes renal tubular tissue and cellular changes. PFAS exposure altered several pathways associated with kidney disease, including oxidative stress, peroxisome proliferator-activated receptor (PPAR) pathway, and epithelial–mesenchymal transition (EMT) [
109]. By evaluating the role of PFAS in Xenopus A6 renal epithelial cells, the inductive effects of these chemicals were attributed to the stimulation of DNA/RNA, secondary protein structures, lipids, and fatty acids, which ultimately lead to cell death [
110]. PFOA exposed to male and female rats showed accumulation in liver, kidney, and small intestinal microsomes. Significant uridine diphosphate -glucuronosyltransferase (UDPGT) activity was observed in all tests, but no evidence of PFOA-glucuronide formation was observed either by highly sensitive radio-chromatography or by liquid chromatography-mass spectrometry (LC/MS) [
111]. Recent studies by Wen et al. [
112] showed that exposure to PFOS resulted in increased expression of renal injury markers Acta2 and Bcl2l1, decreased DNA methylation, and the upregulation of histone demethylases Kdm1a and Kdm4c. In addition, PFOS was shown to induce renal injury and upregulation of transcription factors Nef2l2, Hes1, Ppara, and Ppard. These results suggest a potential adverse effect of PFOS on renal fibrosis and carcinogenesis.
A number of studies have shown that the kidney may be at risk due to exposure to EDCs, including PFAS. However, there are still several important knowledge gaps in our understanding of kidney disease and kidney cancer due to the overlapping populations, limited modeling boundaries, and lack of mechanistic studies. Elucidating the effects of PFAS exposure on genetic, biological, environmental, occupational, and other risk factors is critical. Further studies on the direct and indirect mechanisms of nephrotoxicity, including experimental models, metabolic analysis, and translation to epidemiology is warranted. In addition, how environmental toxicants such as PFAS drive differences in kidney disease among different populations remains poorly understood.
Occupational workers are commonly exposed to high levels of PFAS with greater risk compared to the general population. A study (data from 1950–2009) analyzing cancers and cancer deaths among ~30,000 firefighters (21–29 years of employment) found that cancers of respiratory, digestive, and urinary systems were the highest [
113]. In a study of 40 occupational workers and 52 population-based controls in China, a total of 14 biomarkers related to oxidative stress, fatty acid β-oxidation disorder and kidney injury were identified in occupational workers [
114]. HEK-293 cells were exposed to three widely used aqueous film forming foams (AFFFs). All AFFFs induced cytotoxicity and markedly inhibited cell proliferation when exposed to only one-tenth of the working concentration of fire suppression [
115]. Therefore, the health effects of occupational exposure to PFAS on workers should not be ignored [
116]. Studies from meta-analysis focused on cancer risk among firefighters indicated that firefighters were at increased risk of developing multiple myeloma, non-Hodgkin lymphoma, prostate, kidney, lung, and testicular cancer. Eight additional cancers were also listed as having a “possible” association with exposures to fire training activities [
117,
118]. Risk for these cancers among firefighters may be related to direct exposures to complex toxicants during fire training activities through inhalation and contact with PPE contributing to the modulation of biochemical or physiological pathways that put firefighters at increased baseline risk of developing cancer [
119]. Cancer is also one of the leading causes of death among firefighters according to the Centers for Disease Control and Prevention [
113,
117,
118]. Research is needed to reveal toxicity due to occupational exposure in the study of PFAS.
Currently, many traditional PFAS are being phased out and are being replaced by commercial compounds such as GenX, F-53B, and short-chain variants. Even more challenging is the existence of hundreds of undiscovered PFAS compounds whose health effects are unknown. Because of the dramatic increase in the production of novel alternative PFAS compounds, there is an urgent need to understand the relationship between PFAS exposure and kidney disease to find key biomarkers triggered due to PFAS toxicity.


留言 (0)