1. IntroductionAmputation is a procedure that involves the removal of a body part. Acquired amputation results from an operation that aims to remove a body part following trauma or disease [
1]. Further, a physical disability caused by the loss of limb function due to amputation of the upper or lower extremities is known as an amputation disability. Accordingly, lower-extremity amputees (LEAs) have reduced gait function, less energy efficiency during walking, and difficulties managing prosthetic devices [
2]. Moreover, they often experience pain, falling, and chronic wounds due to prosthetics; hence, they experience restrictions on modifying their lifestyle and participation in regular exercise [
3]. LEAs often suffer from musculoskeletal diseases, are less physically active, and are vulnerable to cardiovascular diseases [
4]. Therefore, amputee rehabilitation should include a long-term health management strategy after acute-phase prosthetic rehabilitation [
5]. Considering the clinical characteristics and the importance of the general health and exercise management of LEAs, a comprehensive approach for managing appropriate lifelong health is essential.Digital health encompasses various platforms and systems that apply technological solutions to enhance healthcare delivery. Digital therapeutics (DTx) is one such category of digital health solutions that provides evidence-based, software-driven therapeutic interventions for the prevention and management of a medical disorder or disease [
6]. Recently, a medical service model through a digital healthcare system has gained applications in the clinical field [
7,
8,
9,
10]. A web-based coaching program for clinicians was developed to manage the amputees in general outpatient clinics. Here, we designed a health-management program for LEAs that included self-directed exercise and health management with regular medical clinic supervision [
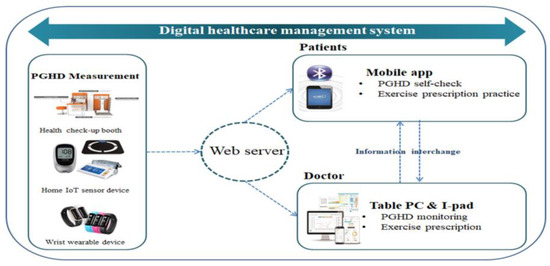
11]. To improve this program’s adherence and effectiveness, we applied a digital healthcare system that contained mobile applications, wearable devices for amputees, and a health check-up booth in the hospital. This study aimed to evaluate the effect of our novel digital healthcare management system on LEAs. 4. Discussion
To our knowledge, this was the first study to evaluate the effectiveness and safety of self-directed physical-strength training and cardiovascular exercise using a digital healthcare management system developed for patients with LLA. This study showed a statistically significant improvement in the grip strength, lower-limb muscle strength, thigh circumference, and HbA1c level in patients with LLA.
Skeletal muscle plays an important role in the metabolism and activities of daily living [
22]. Reduced skeletal muscle mass and function increase the risks of various chronic diseases, including insulin resistance, hyperglycemia, and atherosclerosis; they also induce disability, falls, and osteoporosis [
23]. The measurements of grip strength and lower-limb muscle strength were used as a representative method that measured skeletal muscle in a previous study [
24]. The lower-limb muscle and grip strengths were correlated with each other [
25]. Therefore, increasing or maintaining the grip and the lower-limb muscle strength and mass plays an important role in a patient’s overall health. This study measured the muscle strength of knee flexion and extension of the intact limb, thigh circumference, and grip strength, all of which increased in a statistically significant manner. This meant that the physical-strength training that used the digital healthcare management system increased the muscle strength and mass of the skeletal muscle. A previous study of a 12-week personalized exercise program that consisted of stretching, muscle-strength training, balance training, and cardiovascular exercise in patients with LLA reported that the gait function and lower-limb muscle strength improved [
26]. A study by Lee et al. that evaluated a web-based exercise program in older adults reported that the overall muscle strength improved, thereby improving gait and balance and preventing falls [
27]. The significant effects of personalized and web-based exercise programs were similar to the results of this study, which used a system developed from a mixture of those two programs. In addition, the grip strength, lower-limb muscle strength, and thigh circumference increased in this study due to the lower-limb muscle-strength training along with the functional exercise used while considering the characteristics of the patients.Resistance training improves the muscle mass and strength, physical function, mental health, bone density, insulin sensitivity, blood pressure, lipid profile, and cardiovascular health in adults. In addition, cardiovascular exercise increases insulin sensitivity, mitochondrial density, vascular compliance, vasoreactivity, pulmonary function, immune function, and cardiac output [
28,
29,
30,
31]. Furthermore, regular exercise reduces the resting heart rate, increases resistance to myocardial dysrhythmias, reduces atherosclerosis by improving blood lipids, and prevents or delays the onset of type 2 diabetes. Since serum lipid variables affect the metabolism of healthy individuals and patients in various ways, it is very important to keep serum lipid levels in healthy ranges [
32]. Exercising reduces the levels of TC, TG, and LDL-C and increases the level of HDL-C [
33,
34]. Previous studies reported that a combination of cardiovascular exercise and resistance training was more effective than performing these alone and that performing moderate- to low-intensity exercise showed positive results on certain serum lipid variables compared to high-intensity exercise [
35,
36]. However, another study reported that no changes in serum lipid variables were observed after cardiovascular exercise and resistance training [
37]. These conflicting study results may have been due to the differences in the experimental environments. This study did not show statistically significant changes in the serum lipid profile, which might have been due to the lower level of adherence to the cardiovascular exercise than the level of adherence to the physical-strength training. In contrast, the Hb1Ac test showed a statistically significant change. A study by Connelly et al. reported that for adults with type 2 diabetes, IoT-based physical activity that promoted intervention would be more effective than the general treatment [
38]. Using devices such as wearable activity trackers and pedometers can change behaviors by monitoring physical activities [
39]. In this study, behavioral changes may have resulted from the continuous monitoring of activity levels and blood glucose on the web using IoT-based wearable devices and blood glucose monitors.The lungs acquire the oxygen required for exercising and release carbon dioxide from the body [
40]. Since the body uses more energy during exercise, the oxygen demand increases. The lungs also play an important role in motor ability [
40]. The FVC and FEV are physiological elements that signify the ability of pulmonary function [
41]. In this study, no statistically significant changes in the FVC and FEV1 were observed. In a previous study that assessed the effect of trampoline training as a cardiovascular exercise for 8 weeks in adolescent participants, no significant change in the FEV1 was observed [
42]. In a study that used an ICT-based healthcare service in patients with a spinal cord injury, an improvement in the pulmonary function was observed, although it was not statistically significant [
43]. The results of this study were similar to those of previous studies, which might have been due to the absence of respiratory muscle training, which is a key factor in improving pulmonary function and in short-term interventions [
43]. The World Health Organization defines the quality of life as an individual perception of a person’s life position in the context of culture and value system, as well as the tasks, expectations, and standards set by environmental conditions [
44]. The quality of life may vary depending on multiple factors and can indicate various aspects of human life. A study by Grzebień et al. reported that among various factors that determined the quality of life of a patient after amputating their lower limb, appropriate treatment and rehabilitation should be the first priority [
45] and that an increase in physical activities was a factor that influenced the quality of life. In this study, changes in the quality of life and activity levels were observed, although they were not statistically significant. In a recent study, the quality of life, physical activity, and opportunity for social engagement in Korean adults during the COVID-19 pandemic were lower compared to those during the pre-COVID-19 period [
46]. This may have been due to the fact that more individuals spent a lot of time indoors by working at home and refraining from outdoor activities due to the spread and prolongation of COVID-19 while the study was conducted.An average of 25% of patients do not comply with prevention and disease management activities (e.g., exercise, diet, medication, and screening) in the disease state. Adherence can drop to 50% or below in some medical conditions and environments [
47]. To increase adherence, this study used a digital healthcare service that allowed for two-way communication between the doctor and patient and monitoring of the patients’ adherence to the exercise programs [
48]. The results showed a relatively high level of non-adherence of 19.5%, which was lower than the mean level (25%) of non-adherence reported in previous studies [
47]. The score for satisfaction in the satisfaction survey was high. In particular, the items that indicated that the device was helpful in health management and motivation showed high scores. The overall determination of medical outcomes and answers to the self-subjective survey questions showed that self-directed exercise using the digital healthcare management system could be considered a healthcare model for patients with amputation.
This study had some limitations. This study could not be generalized to all patients with LLA because we only included patients who met the inclusion criteria. In addition, we did not follow up regarding how long the effects lasted after the intervention. Since this was a pilot study, the sample size was small. There was a lack of information to verify the clinical efficacy because the study had no control group. Moreover, whether the patients’ physical-strength training and cardiovascular exercise performance rates were accurately measured could not be verified. Randomized controlled trials should be conducted by supplementing the limitations mentioned above and expanding the sample size to generalize the study results in the future. Furthermore, a strategic method should be established to reduce the study participants’ non-adherence to exercise programs.



留言 (0)