
記住我



The parents or legal guardians returned to the center all the leftover containers (empty containers and containers with products) to record the amount of product dispensed and the amount of infant formula used up to the time of the visit; the corresponding weighing was performed and the percentage of product ingested by the participants was determined. Finally, the grams of formula consumed by each infant, measured by weighing the leftover formula or as indicated in the parents’ diary corresponding to the periods between visits 1–2, 2–3, and 3–4, were available. The participants of this study included in the formula-feeding groups were considered compliant if they took at least 80% of the formula during the first six months while in the breastfeeding group it was considered a valid external control if more than 80% of the feedings were breastfeeding. All infants included in the BFD group, except one, consumed more than 80% human milk during the first six months.
Based on the record of the amount of product dispensed and the amount of infant formula used (measurement of leftover) we estimated the average daily intake from visits 1 to 4 for the STD group (130.2 ± 14.7 g/d, equivalent to 671 ± 76 kcal/d of energy and 13.8 ± 1.56 g/d of protein) and the INN group (134.0 ± 18.2 g/d, equivalent to 655 ± 89 kcal /d of energy and 12.60 g/d of protein).
A GLM-ANOVA was performed for grams of formula consumed per day, and significant differences were observed for visit, sex, and infant birth weight, but not the formula used (data not presented).
The primary variable (weight gain) consisted of the difference in infant weight (in g/day) between the initial recruitment visit and the 6-month visit, divided by the number of days between the two visits. This analysis was performed on the 187 infants who completed until visit 4 (6 months). The difference between visit 1 and visit 4 was calculated in days of 187 children individually (Table 3). When analyzing the mean difference in weight gain between the groups of children treated with the STD and INN formulas (Table 3), there was no statistically significant difference in weight gain between the two formulations. On the other hand, an ANOVA of the weight difference between visits 1 and 4 was performed for the STD and INN formulas controlling for gender, maternal body mass index (BMI), and birth weight. There were significant differences in weight difference between visits 1 and 4 as a function of gender and infant birth weight, but not as a function of formula or mother’s BMI (Table 3). The grams consumed per day were also related to the difference in weight between visits 1 and 4. Based on the weighing of leftover dispensed formula, a multivariate analysis of variance (MANOVA) of the difference in weight of the children between visits 1 and 4 was performed as a function of formula consumed (STD, INN), gender (male, female), maternal BMI (25), birth weight (3500), and grams ingested per day. A moderate positive correlation (r = 0.535) was observed between mean grams ingested per day (measured by weighing leftover formula) and weight gain between visits 1 and 4 of the infants. This correlation changed significantly by gender (males achieved larger weight differences for the same daily grams of formula consumed) and by birth weight (infants with birth weights > 3500 g achieved larger weight differences for the same daily grams of formula consumed) but not as a function of maternal BMI or formula used.This same MANOVA as a function of grams ingested daily according to the parental diary also showed a positive correlation (r = 0.626) between mean grams ingested per day (obtained from parental diary entries) and weight gain between visits 1 and 4 of the infants. This correlation changed significantly by gender (boys achieved larger weight differences for the same daily grams of formulation consumed) and by birth weight (children with birth weights >3500 achieved larger weight differences, especially those who consumed more daily grams of formula) but not as a function of maternal BMI or formula used.
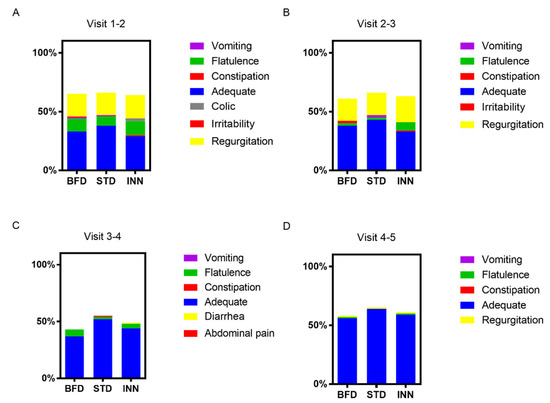
Secondarily and as foreseen in the study protocol, the weight gain of the infants who received each of the formulas studied was compared with the BFD group. The results of this analysis are shown in Table 3, where it can be seen that BFD infants had a significantly lower weight gain at 6 months of age than that shown by infants fed with either of the two formulas evaluated (STD and INN).The same analysis was performed for the variable weight gain at 12 months of study. Table 3 shows the number of children in each of the three groups studied with weight values recorded at visit 1 (21 days of age) and visit 5 (12 months ± 2 weeks). A comparison of the means of weight gain from the different formulations (STD vs. INN, STD vs. BFD, and INN vs. BFD, Table 3) revealed that at 6 months there was no significant difference in weight gain (measured in g/day) as well as at 12 months between the STD and INN formulas. The total weight of the STD formula group remained significantly higher than the BFD group at 12 months; however, the INN group exhibited a trend to be different from breastfeeding between visits 1 and 5 (p = 0.057). A GLM-ANOVA (data not presented) showed significant differences for visit (pp = 0.004), but not for formula exclusively (p = 0.381). The largest effect size was associated with the visit factor.No significant differences were observed in length and head circumference, as well as tricipital and subscapular skinfolds and mean upper arm circumference (Table 4 and Table 5).In the case of BMI, the ANOVA (Table 6) showed significant differences for visit (ppp = 0.487). The largest effect size was associated with the visit factor (0.4230, data not provided). In addition, we have reported that it was from the third visit onwards that the mean BMI was higher in the STD and INN formulas compared to the BFD group; hence, the interaction effect appeared as significant (Table 6). For the body fat percentage, the ANOVA (Table 6) showed significant differences for visit (p = 0.005), but not for the interaction between the formula and visit (p = 0.958) or for formula (p = 0.249). The largest effect size was associated with the visit factor (0.0236, data not shown). Finally, for the lean mass, the ANOVA (Table 6) showed significant differences for visit (pp = 0.054) or for formula (p = 0.215). The largest effect size was associated with the visit factor (0.6093, data not provided).In the case of BMI percentiles, the ANOVA (Table S1) revealed significant differences for visit (p = 0.009) and the interaction between formula and visit (p = 0.006), but not for formula (p = 0.504). The largest effect size was associated with the visit factor (0.0222, data not provided). In the ANOVA, there were significant differences in the height percentiles for visit (p = 0.011), for the interaction between formula and visit (pp = 0.433, Table S1). The largest effect size as associated with the visit factor (0.0154, data not shown). Finally, in the weight percentiles, the ANOVA (Table S1) showed significant differences for visit (ppp = 0.368). The largest effect size was associated with the visit factor (0.0228, data not provided).The time course of the study showed a difference between breastfed infants presenting stools of a more liquid consistency (Table S2), although these differences ceased to be significant at visit 5 (see Table S2). Likewise, the daily number of stools was higher in breastfed infants at visits 1, 2, and 3, but these differences ceased to be significant at visits 4 and 5 (Table 7).Figure 1 shows the tabulation of the different categories of digestive tolerance between every two visits. An increase in the percentage of children with high tolerance was seen throughout the study without significant differences between the different formulas and compared with the BFD group.The infant’s behavior was re-coded as altered mood or pleasant mood according to the guardians or parents. Table S3 shows how the percentage of infants with altered behavior decreased throughout the study. No significant differences were observed among the three ways of feeding.The study found no differences in tolerability between the different groups (Table S4). Regarding to the safety of the different formula, the majority of the adverse events (n = 754) were mild—Grade 1 (94.3%), 13 were moderate—Grade 2 (1.6% of the total), and none were severe— Grade 3. The intensity was not recorded for 33 of the events (4.1%) (Table 8). There were no differences between the different groups concerning the intensity of the events. For example, 93.0% of events were mild in the BFD group, 91.8% in the INN group, and 97.6% in the STD group.Most of the gastrointestinal symptoms were mild, with one growth failure within the BFD group that led to the introduction of artificial breastfeeding together with breastfeeding; two events, neonatal constipation and abdominal pain, recorded for one infant within the INN group, led to a change in formula and the abandonment of the study; and two (infantile colic and infant reflux) were recorded for one infant within the STD group and led to a change in formula and the abandonment of the study (Table 8).For morbidities that occurred with a frequency greater than 1%, BFD infants exhibited the lowest incidence and infants fed the INN formula experienced significantly fewer general disorders and disturbances compared with the STD group. Indeed, the infants who were fed STD formula had a significantly higher incidence of atopic dermatitis, bronchitis, and bronchiolitis events than the infants who were fed BFD or INN formula. (Table 9). 4. DiscussionThe present randomized, double-blind, placebo-controlled clinical trial was designed to determine whether a novel starting infant formula with reduced protein content and lower casein to whey protein ratio by increasing the content of α-lactalbumin influenced weight gain and body composition compared to a standard formula at 6 and 12 months of age. Furthermore, this product contains higher levels of DHA and ARA, as well as a postbiotic thermally inactivated (BPL1TM HT), compared with standard infant formula. An exclusively breastfed population was followed up as a reference. At 6 and 12 months, infants receiving either INN or STD formula gained more weight than the BFD group, while no difference was observed between STD and INN formulas. BMI was also higher in infants fed either formula than in those breastfed. Regarding body composition, length, head circumference, and tricipital/subscapular skinfolds, we found that all of the measures were similar between all groups. It is important to note that the INN formula was considered safe based on weight gain and body composition, which were within the normal limits, according to WHO standards. Compared to both formulas, BFD produced stools that were more liquid in consistency. Throughout the study period, all groups exhibited similar digestive tolerance and infant behavior. In terms of the total number of adverse events reported, the STD formula had the highest number, followed by the INN formula and finally, the BFD group. However, the majority of them were not related to the type of feeding. Besides, infants fed either BFD or the INN formula exhibited significantly lower episodes of atopic dermatitis, bronchitis, and bronchiolitis events than those fed the STD formula.
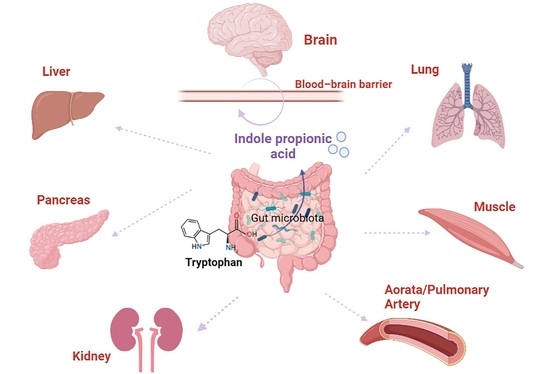
In addition to exposure to metabolic and endocrine factors during pregnancy [47], protein intake in formula-fed infants during the first year of life may have a significant impact on growth later in life and the risk of obesity and metabolic disorders in adulthood [20,48]. Indeed, the protein content of infant formula is usually greater than that of human milk to provide all essential amino acids in adequate quantities [49]. Scientific evidence indicates that infants fed a formula containing more protein gain more weight during the first year of life and are heavier at 2 years of age than infants consuming a formula containing less protein [48], which reduces the risk of obesity at school age [24]. In our RCT, infants fed either INN or STD formula gained more weight than the breastfed group at 6 months as measured by differential daily weight gain per day (g). Similar results have been reported in other earlier studies [50] even with a relatively low content of protein [51]. However, previous studies on formulas with a reduced protein-to-energy ratio of up to 1.8 g/100 kcal have shown more modest differences in growth patterns compared with breastfed infants, similar to our findings [48,52,53], which supports the hypothesis that the protein-to-energy ratio plays a key role for weight gain. In our study the intake of INN formula was slightly higher than the STD formula, thus compensating for the lower energy content and protein of the former. Compensation for lower energy density and protein has been reported in other studies [51]. After 12 months, the STD group was significantly higher than the BFD and INN groups. We should note that the INN formula contains 8% less protein per 100 kcal than the STD. Thus, in the first six to eight weeks of life, there is almost no difference between breast milk and formula-fed infants in terms of growth (gain in weight and length). Indeed, it has been previously reported that formula-fed infants gained weight and length more rapidly than breastfed infants from about two months of age to the end of their first year of life [54]. Interestingly, the results of a recent review suggest that the difference in weight gain between formula-fed and breastfed infants is relatively small, comparable, and significantly less than the nutritionally significant differences used in determining sample size [55].In addition to the total protein content, the whey/casein ratio in infant formulas seems to be important for the first year of life. Whey proteins, particularly β-lactoglobulin and α-lactalbumin, are rapidly digested and participate in the building of muscle mass [25], and particularly, α-lactalbumin is the major protein in human milk [26]. Thus, the addition of bovine α-lactalbumin to infant formula modifies the plasma amino acid pattern of the receiver infant, allowing a reduction in the protein content of the formula. On the other hand, casein proteins are water-insoluble high-molecular-weight molecules that are a source of phosphate and calcium in human milk, because of the highly phosphorylated nature of β-casein and α-S1-casein, and the requirement for calcium in forming the aggregates of casein micelles [56]. Nevertheless, the amount should be controlled to avoid improper digestion in early life. In this context, using cow’s milk as the protein source in infant formula might result in an α-casein-dominant formula, which differs from whey-protein dominance in human milk. Further, bovine whey contains a high concentration of β-lactoglobulin, which is absent in human milk [57]; therefore, adding bovine α-lactalbumin to infant formula makes it more similar to that of breastfed infants [58]. Moreover, α-lactalbumin is relatively rich in tryptophan, which may result in satisfactory growth and plasma tryptophan levels similar to those of breastfed infants and infants fed standard formula [59]. Nevertheless, in our study, both formula-fed infants gained weight more rapidly compared with exclusively breastfed infants, and there was no significant difference between the groups in terms of length, head circumference, tricipital and subscapular skinfolds, and upper arm circumference, suggesting that both formulas cause similar body composition in infants.The proportion of fatty acids present in infant formulas is important to ensure the correct growth and development of infants. In the last 20 years, formulas have been supplemented with LC-PUFA in amounts similar to breast milk. Despite the new EU regulation that indicates that AA does not need to be included, intervention studies assessing the impact of DHA- and AA-supplemented formulas have resulted in numerous positive developmental outcomes (closer to breastfed infants) including measures of specific cognition functions, visual acuity, and immune responses [60,61,62]. AA has different biological functions compared to DHA, for example, AA has exclusive functions in the vasculature and specific aspects of immunity. Undeniably, most of the trials include both DHA and AA, and test development specific to DHA such as neural and visual development. DHA suppresses membrane AA concentrations and its function. Infant formula with DHA and no AA runs the risk of cardio- and cerebrovascular morbidity and even mortality through suppression of the favorable oxylipin derivatives of AA [63]. International expert consensus suggests that infant formulas that contain DHA at a concentration of 0.3% to 0.5% by weight of total fat and AA at a minimum level equivalent to the amount of DHA should be clinically tested [29,30]. In this study, we used an advanced formula enhanced with a double amount of DHA/AA in comparison with an STD formula to provide evidence about weight gain and body composition, among other outcomes. Throughout the study, the percentage of children with high tolerance increased without significant differences between formulations and compared to the group receiving BFD. According to the guardians or parents, the infant’s behavior was classified as altered mood or pleasant mood. There was a decrease in the number of infants with altered behavior throughout the study. The three methods of feeding did not show any significant differences.The INN formula was also supplemented with a thermally inactivated postbiotic Bifidobacterium animalis subsp. lactis, BPL1TM [40,64], which may confer some benefits regarding body composition, metabolism, and gut microbiota composition. Probiotics have many health benefits by modulating the gut microbiome; nonetheless, techno-functional limitations have made it gradually shift from viable probiotic bacteria towards non-viable postbiotics, paraprobiotics, and/or probiotics-derived biomolecules, so-called postbiotics [64]. Since the experimental formula of the present study was supplemented with BPL1TM HT, it should be noted that in vivo studies reported that this strain can be considered a Generally Recognized as Safe (GRAS) substance. In terms of the intensity of GI symptoms, tolerability, and safety, there were no differences between the different groups (BFD, STD, and INN formula). In different contexts and using different methods, infants are fed a variety of products. The formula for infants is available in many variations, many of which are superior to other methods of feeding and some of which are inferior to others. On the other hand, there was a significant difference between BFD group presenting stools of a more liquid consistency, although this difference no longer existed at visit five (12 months). Additionally, BFD infants had more stools per day at visits 1, 2, and 3, but these differences ceased to be significant at visits 4 and 5. STD formula group reported the most GI symptoms, followed by the INN formula and BFD group. Triacylglycerol composition of infant formulas can influence the characteristics of stools i.e., appearance and consistency. As the fat sources differed between the STD and the INN formulas, we can hypothesize that the changes observed in fecal consistency might be due in part to this feature.There were no differences in safety across the study between the different groups. Several differences were observed between the two formulas, showing a significant reduction in general disorders and disturbances among children who received the INN formula. STD formula-fed infants were more likely to cause atopic dermatitis, bronchitis, and bronchiolitis than BFD or INN formula-fed infants. Eczema or atopic dermatitis is a common chronic inflammatory skin disease, mostly occurring in children. Indeed, a meta-analysis showed that probiotic supplementation during both the prenatal and the postnatal period reduced the incidence of atopic dermatitis in infants and children, suggesting that starting probiotic treatment during gestation and continuing through the first 6 months of the infant’s life may be of benefit in the prevention of atopic dermatitis [65]. In this context, a study demonstrated that prenatal and postnatal supplementation with a mixture of B. bifidum BGN4, B. lactis AD011, and L. acidophilus AD031 is an effective approach in preventing the development of eczema in infants at high risk of allergy during the first year of life [66]. Hence, the lower incidence of atopic dermatitis observed in the INN formula group compared to the STD group might be mediated by the supplementation of the postbiotic BPL1TM HT. Likewise, respiratory tract infections represent one of the main health problems in children of different ages [67]. Finally, changes in the intestinal microbiota will need to be assessed.There are some limitations to this study. There were no significant correlations between the type of feeding and the number of adverse events. Nevertheless, the number of infants in the present study was calculated for growth as the main variable and not for morbidity.
In conclusion, this clinical trial involved the evaluation of a novel infant formula with reduced content of total protein and modification of the whey/casein ratio by increasing the content of α-lactalbumin, increased levels of both AA and DHA, and postbiotic in comparison with standard infant formula. For exploratory analysis, a third unblinded group of breastfed infants was used. Both formulas gained more weight at 6 and 12 months than the BFD group, while no differences were observed between STD and INN formulas. Infants fed both formulas had a higher BMI than those fed BFD. Body composition, head circumference, and tricipital/subscapular skinfolds were similar between the two groups. We should note that the INN formula is safe and it showed a reduction in atopic dermatitis, bronchitis, and bronchiolitis in infants compared to STD formula. The consistency of the stools produced by BFD was more liquid in comparison with both formulas. For further analysis, it would be necessary to examine more precise health biomarkers and to carry out long-term longitudinal studies.
留言 (0)