1. IntroductionCoeliac disease (CD) is a chronic small intestinal immune-mediated enteropathy triggered by dietary gluten and related proteins found in wheat, rye, and barley, occurring in genetically predisposed individuals, those with HLA (Human Leukocyte Antigen) DQ2 and/or DQ8 haplotypes. In patients with CD, ingestion of dietary gluten results in autoimmune intestinal mucosal damage characterised by villous atrophy, crypt hyperplasia, and an increased number of intraepithelial lymphocytes [
1,
2,
3,
4]. Patients with CD may present with a wide range of symptoms or may be asymptomatic. Gastrointestinal symptoms and signs include chronic or intermittent diarrhoea, weight loss, failure to thrive, nausea or vomiting, chronic abdominal pain, cramping or distension, chronic constipation, and abnormal liver biochemistry. There is also a broad spectrum of possible extraintestinal symptoms, such as dermatitis herpetiformis, stunted growth, delayed puberty, amenorrhoea, recurrent aphthous stomatitis, iron-deficiency anaemia, fracture with inadequate traumas, irritability, arthritis, and chronic fatigue [
2,
3,
4,
5]. There is an evident shift from gastrointestinal to extraintestinal symptoms in children, and recent data suggest that the frequency of those symptoms is similar in adults and children [
6,
7]. Patients with autoimmune diseases and chromosomopathies, such as diabetes mellitus type I, autoimmune liver disease, autoimmune thyroid disease, Down syndrome, Turner syndrome, William’s syndrome, and patients with IgA deficiency have a higher risk of developing CD and should be screened periodically. First-degree relatives of patients with CD are also a high-risk group in whom active screening should always be conducted [
4]. The diagnostic procedure involves the assessment of coeliac disease-specific antibodies, such as antibodies to tissue transglutaminase (tTG), endomysial antibodies (EMA), and immunoglobulin G (IgG)-deamidated gliadin peptides (DGP) or other IgG type antibodies in patients with IgA insufficiency, and sometimes an endoscopic procedure with small bowel biopsies. In children, according to the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) guidelines, under certain conditions, the diagnosis can be established with a strongly positive tTG antibody titre, if confirmed with positive EMA antibodies in a second blood sample, without the need for small intestinal biopsy [
8]. The therapy for confirmed CD is a strict lifelong gluten-free diet which results in a full clinical and histological remission occurs, with reduced morbidity and mortality [
9,
10]. Standard serology testing is used to establish a diagnosis, but it is only available at specialised centres, especially EMA antibodies. New and improved point-of-care (POC) methods are non-invasive and could help reduce diagnostic delay in asymptomatic individuals, especially in areas with limited access to laboratory-based testing [
11,
12,
13]. Although there are many promising results on POC testing, they are still not included in diagnostic algorithms for CD, mostly due to conflicting results on specificity and sensitivity of various POC tests, especially in asymptomatic children [
12,
14]. The global prevalence of CD is 1% and differs among countries. In the United States, the overall prevalence is 1%, significantly higher in Caucasians. In Europe, the highest prevalence of CD is found in Sweden (3%) and Finland (2.4%), while it is lower in Italy (0.7%), Western Ireland (0.6%), and Germany (0.3%) [
3,
15,
16,
17,
18]. There are limited data on CD prevalence in Croatia, determined by research conducted 20 years ago in one region of the country. The cumulative incidence was found to be 1.9:1000 live births and a prevalence of 0.21% [
19,
20]. A more recent study performed in Croatia tried to determine the prevalence of CD in first-grade school children using the IgA anti-tTG POC test, and not a single child with CD was detected [
21].
The aims of our study was to determine the prevalence of CD using the rapid IgA and IgG DGP POC test in first-grade school children and to asses the characteristics of children found by POCT screening, such as sex, body mass index (BMI), and the presence of symptoms.
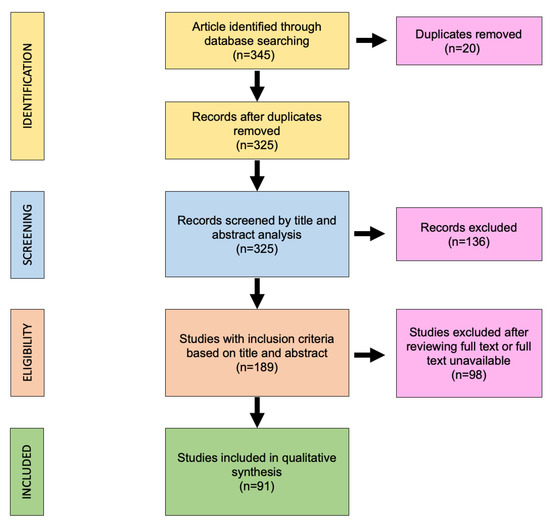
3. ResultsThere were 1404 children (51% girls, average age 7.23 years) included in the study and tested with POC. The results of the POC tests are as follows: for 1307 (93.1%) children, POCT was negative and showed normal total IgA and negative DGP. Out of the remaining children, 85 children (6.05%) had positive POCT (with normal total IgA and positive DGP), and 12 children (0.85%) were IgA-deficient but DGP-negative. None of children tested with POC were negative for total IgA but positive for DGP (
Figure 1).Children with a positive rapid POC test result (n = 85; 6.05%) were referred to paediatric gastroenterology. At appointment, a paediatric gastroenterologist obtained data about presence of CD symptoms and family history for CD, associated diseases, body weight, and body height. BMI was calculated as a ratio of body weight in kilograms (kg) and body height in meter (m)2. They were all clinically examined and advised to perform CD serology testing (total IgA and anti-tTG). Caregivers of four children refused to do further diagnostic testing and two were excluded because they were older than first-graders (those were symptomatic older brothers of two included patients). Out of 79 POC positive children referred for further testing, 8 had positive IgA antibodies against tTG. Concerning the children with IgA insufficiency (regarded as levels of IgA less than 0.2 g/L), we used IgG-DGP antibodies, and all IgA insufficient children were negative for CD. Finally, seven children were diagnosed with CD (0.5%) and one child who had normal intestinal mucosa on intestinal biopsy samples was diagnosed with a potential CD. Six children (86%) with CD had anti-tTG ≥ 10 times the upper limit of normal (ULN), and one had 1.5 times the ULN. Six children underwent upper endoscopy (one had Marsh 2, and two 3a, one 3b, and two 3c), and one child was diagnosed with no-biopsy approach according to ESPGHAN guidelines (
Table 1) [
8].Out of 71 POC-positive children but negative for CD, 32 children (45%) had the following symptoms: abdominal pain (20), constipation (10), prolonged diarrhoea (2), frequent vomiting (2), recurrent aphthous ulcers (2), and one failure to thrive. In children later diagnosed with CD, four children had symptoms, all four having recurrent abdominal pain, plus one who also had constipation and one who had frequent aphthous ulcerations. We compared CD children with those who were positive for POC but had negative anti-tTG, and we did not find any significant differences in age nor BMI. Children diagnosed with CD were not symptomatic more often than those who were positive for POC but had negative serology (
Table 2). However, when compared regarding only abdominal pain, children diagnosed with CD complained of abdominal pain significantly more often (p = 0.002). 4. DiscussionCD is a global, common disease with a rising prevalence in the last 50 years and a broad spectrum of disease manifestations, affecting approximately 1% of the population [
24,
25,
26]. However, the increasing prevalence is most probably due to case-finding-screening strategy, better serological tests, and raised awareness of physicians [
27]. CD is only relatively uncommon in Southeast Asia and sub-Saharan Africa, while there are reports that it is under-recognised in China [
24,
28,
29]. The prevalence of CD is also low in some European countries, such as Estonia, even despite a dramatic increase in incidence during the last 35 years [
30]. The two major determinants of CD prevalence are HLA haplotype and wheat consumption, but other risk factors appear to be in relation to the development of CD, such as environmental factors, geographic region, ethnicity, and origin [
31,
32]. The data on CD prevalence and risk factors in Croatia are limited. One study performed in a healthy high-school-student population showed the prevalence of 0.21%, and another, which used the IgA anti-tTG POC test, did not find any cases in more than 1400 of 7-year-old children [
20,
21]. In our study, the prevalence of CD in a population of first-grade children was 1:200 (0.5%) individuals, which is considerably higher than that previously reported. The prevalence in our cohort could have been higher, as the study did not include blood serology tests on POC-negative individuals, and we cannot exclude the possibility of missing CD patients due to possible false negative POC tests. This study used the SimtomaX Blood Drop test to detect immunoglobulin IgA and IgG antibodies against DGP. According to studies, the test showed good high sensitivity (95–100%) and specificity (93.1–95.7%) in ruling out symptomatic CD individuals [
22,
23]. In this study, we had a significant number of false-positive tests, and we can only speculate that the patients who had faint lines in their test were also referred to paediatric gastroenterology, as a similar experience was shown in other studies [
33]. As other researchers suggest, with a large number of false-positive tests, as was our experience, the role of the test cannot replace conventional serology, but it can be used as a triage test to decide if conventional serology is necessary [
34]. However, the opinions of researchers on determining the prevalence of CD with rapid POC tests are not unilaterally positive. In study by Dekanić et al., 1487 children were screened, and not a single child with CD was detected; thus, the authors concluded that the POC test was not useful. The researchers used a different lateral flow test determining the presence of endogenous tTG IgA and total IgA, which, according to existing research, also showed a good sensitivity and specificity in different age groups [
21,
35]. Other studies also showed lower sensitivity and specificity of rapid POC tests than expected, resulting in a lower CD prevalence in examined populations [
36]. According to researchers, proper training in interpreting the results could improve the strength of the test [
11,
21]. All of the presented data suggest that POC tests could be used to identify patients with undiagnosed CD, but further studies and validation are required in finding the optimal test, especially in the paediatric population. According to our study’s findings, 43% of children detected by this screening and diagnosed with CD were asymptomatic and otherwise would not be diagnosed with CD. Our results are in concordance with global trends, as the data show that 90% of the patients remain under-diagnosed or undiagnosed in clinical practice due to being asymptomatic or oligosymptomatic [
2,
11,
12]. Out of symptomatic patients (57%), all children had mild, recurrent abdominal pain, and one patient had constipation and another recurrent aphthous ulcers. As the symptoms were mild and not of a concern to parents, they were not investigated by primary physician. Although clinically silent, our patients had significant intestinal mucosal lesions. Our study results are also in agreement with global trends, highlighting the importance of diagnosing clinically silent patients. Recent studies and reviews suggest that patients diagnosed later in childhood have mild or non-existing gastrointestinal symptoms. In addition, when the disease manifests, the clinical symptoms are often extraintestinal and monosymptomatic [
27]. Our results are in agreement with those of other studies concerning the clinical presentation of coeliac disease in this region of Europe. As per study by Riznik et al., from data on 653 children and adolescents in Central Europe (including Croatia), the most common symptom was abdominal pain in monosymptomatic and polysymptomatic children, especially in the older group of children. [
37]. We recognise that our small cohort of diagnosed CD patients in this study makes it difficult to recognise true differences with POCT-negative children, but nonetheless, the results are still in agreement with those other studies describing clinical characteristics of CD patients in this population [
37,
38]. Complications of CD are common, and CD is known to have long-term complications and an increased risk of malignancy and mortality. There is evidence that untreated disease is associated with delayed puberty, epilepsy, osteoporosis, behavioural disturbances, reduced educational performance, and malignancies (small intestinal adenocarcinoma and T-cell lymphoma) [
11,
39,
40]. Although there are only few studies regarding the long-term health-economic aspect of CD, complications and morbidity present an important socio-economic factor, and timely CD diagnosis is associated with a significant overall healthcare cost reduction [
40,
41]. Screening for CD fulfils most of the criteria for mass screening (prevalence, known morbidity and disease complications, and available treatment), but due to the poor understanding of natural course of the disease and the outcome of asymptomatic patients, there are still no recommendations for mass screening, except in high-risk groups [
42]. There is also debate as to whether population screening for CD is beneficial regarding the compliance to diet and quality of life, but studies report that a gluten-free diet improved quality of life in both symptomatic and asymptomatic screened populations and that the adherence to a gluten-free diet was good after the diagnosis was established by screening [
43,
44]. Active screening is important in high-risk groups, such as first-degree relatives and in individuals with autoimmune diseases and developmental diseases, such as diabetes mellitus type 1, autoimmune liver disease, autoimmune thyroid disease, Down syndrome, Turner syndrome, William’s syndrome, and individuals with IgA deficiency, who have a higher risk of developing CD. Those patients should be actively screened for CD periodically [
2,
3,
4,
45]. Other studies have also shown the importance of active screening of the risk groups and asymptomatic screening as almost 20% of the newly found CD patients can be found with the aforementioned methods [
37]. There is a clear need for a rapid, cheap, and discriminative POC test that could facilitate the triage of suspected CD patients. The aforementioned is mostly crucial in areas with no availability to coeliac-specific serology testing, especially EMA antibodies, which are determined in only specialised laboratories. The proposed test should have optimal specificity and sensitivity, or it should have minimal false negative results while still being cost effective. Those tests could be most useful for primary care physicians and could help relieve the referrals to secondary and tertiary health care institutions. Furthermore, there is a clear need for education about coeliac disease among patients and healthcare professionals, which could altogether reduce the delay in diagnosis [
46].
This study has potential limitations. The data on the incidence and prevalence of CD in Croatia are limited and rely on the results of one study in a limited region of country. Our study aimed to determine the prevalence (using a rapid POC test) and clinical characteristics of CD found by screening among first-grade schoolchildren in Zagreb, Croatia. As the prevalence of CD could differ among other regions in Croatia, we cannot estimate the overall prevalence in Croatia, and there is a need for further research. Croatia has interesting geographical features, with a Mediterranean coastline, large number of islands, and classical continental region; as such, it would be interesting to study possible differences in CD prevalence in those regions. However, approximately one quarter of Croatia’s population is centralised around Zagreb County. Furthermore, this POC test is reported as highly sensitive, but as not all children screened with POC had performed the serology test, we could not determine whether there were false negative POC results and, therefore, missed CD patients. We also screened seven-year-old children, and there is a debate as to what age is appropriate for the timing of screening. Finally, as the test we conducted is qualitative, an unintentional error could have occurred in reading the test results, as a faint positive line could have been missed.



留言 (0)