
記住我










Background: The evolving proportion of the population considered immunologically naive versus primed for more efficient immune memory response to SARS-CoV-2 has implications for risk assessment. We sought to chronicle vaccine- and infection-induced seroprevalence across the first 7 waves of the COVID-19 pandemic in British Columbia, Canada.
Methods: During 8 cross-sectional serosurveys conducted between March 2020 and August 2022, we obtained anonymized residual sera from children and adults who attended an outpatient laboratory network in the Lower Mainland (Greater Vancouver and Fraser Valley). We used at least 3 immunoassays per serosurvey to detect SARS-CoV-2 spike and nucleocapsid antibodies. We assessed any seroprevalence (vaccineor infection-induced, or both), defined by positivity on any 2 assays, and infection-induced seroprevalence, also defined by dual-assay positivity but requiring both antinucleocapsid and antispike detection. We used estimates of infection-induced seroprevalence to explore underascertainment of infections by surveillance case reports.
Results: By January 2021, we estimated that any seroprevalence remained less than 5%, increasing with vaccine rollout to 56% by May–June 2021, 83% by September–October 2021 and 95% by March 2022. Infection-induced seroprevalence remained less than 15% through September–October 2021, increasing across Omicron waves to 42% by March 2022 and 61% by July–August 2022. By August 2022, 70%–80% of children younger than 20 years and 60%–70% of adults aged 20–59 years had been infected, but fewer than half of adults aged 60 years and older had been infected. Compared with estimates of infection-induced seroprevalence, surveillance case reports underestimated infections 12-fold between September 2021 and March 2022 and 92-fold between March 2022 and August 2022.
Interpretation: By August 2022, most children and adults younger than 60 years had evidence of both SARS-CoV-2 vaccination and infection. As previous evidence suggests that a history of both exposures may induce stronger, more durable hybrid immunity than either exposure alone, older adults — who have the lowest infection rates but highest risk of severe outcomes — continue to warrant prioritized vaccination.
The British Columbia Centre for Disease Control (BCCDC) has a long-established serosurvey protocol to monitor population susceptibility to emerging or re-emerging respiratory viruses. The approach was first deployed during the influenza A (H1N1) pandemic in 2009 to monitor changes in seroprevalence across successive pandemic waves and the mass vaccination campaign.1–7 The methodology is predicated upon serial cross-sectional convenience sampling of anonymized residual sera from children and adults of all ages in the most populated Lower Mainland region of BC.8,9
Adapting this protocol, the BCCDC launched its first SARS-CoV-2 serosurvey in March 2020, just before the World Health Organization’s declaration of the COVID-19 pandemic. 10 Baseline assessment was followed by additional serosurveys that spanned the time from mRNA vaccine availability in mid-December 2020, through 7 pandemic waves associated with multiple variants of concern to August 2022 (Figure 1).11–13 Using these serosurveys, we sought to track the evolving proportion of the population that remained immunologically naive and, thus, fully susceptible to COVID-19, versus the evolving proportion that was immunologically primed (through vaccination or infection) and, thus, poised for more efficient memory response in mitigating the risk of SARS-CoV-2. Recognizing the spectrum of illness, including asymptomatic or mild infections, and variable diagnostic access, case identification and reporting, we also used estimates of infection-induced seroprevalence to explore the potential underascertainment of infections by surveillance case reports.
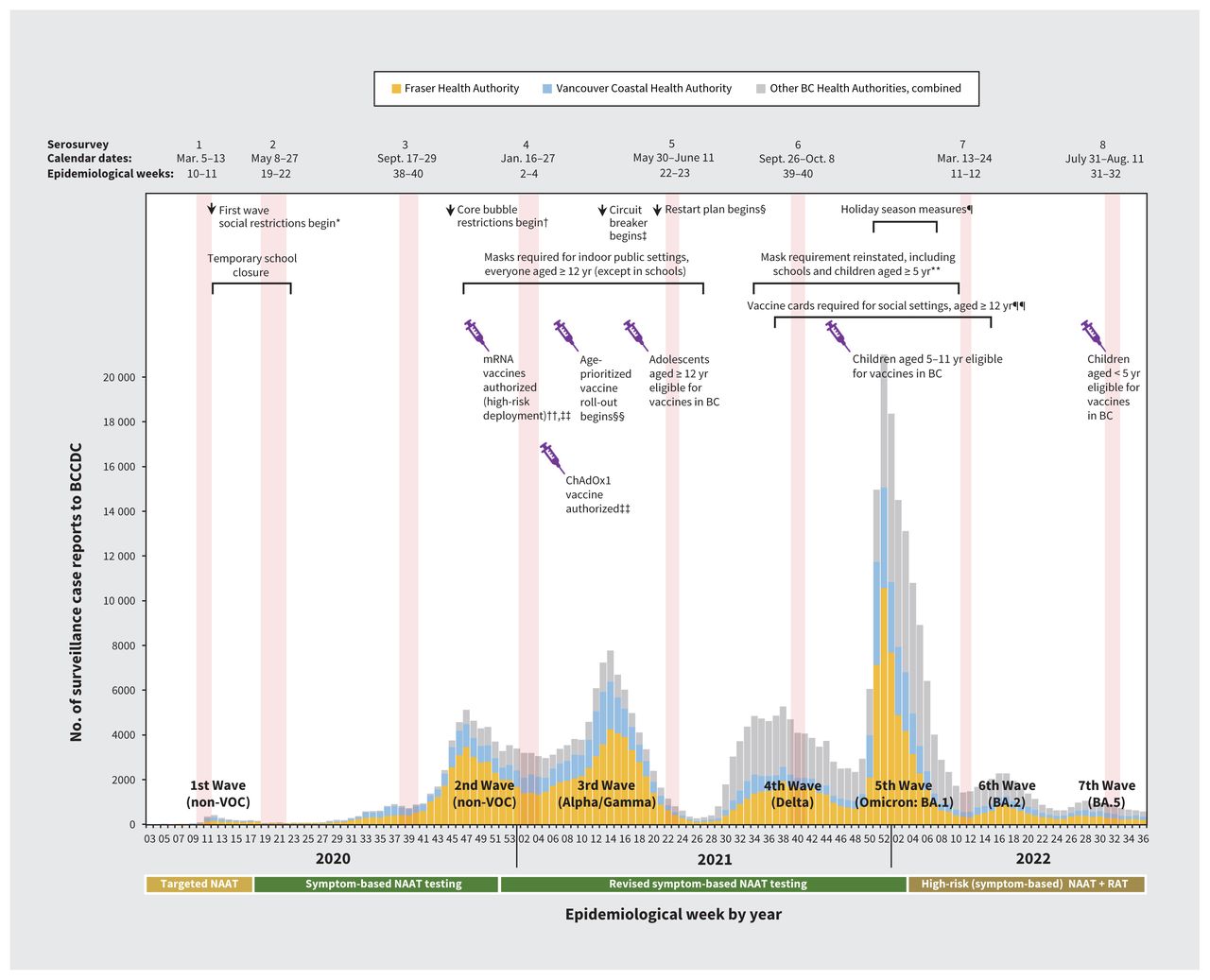 Figure 1:
Figure 1: Provincial surveillance case reports to the British Columbia Centre for Disease Control (BCCDC) by epidemiological week from January 2020 to September 2022, with timing of serosurveys and select public health measures, in BC, Canada. We group case tallies by epidemiological week (7-d period) as per standard surveillance methods for comparing data by period from year to year. Epidemic waves are enumerated sequentially and are displayed with the predominant variant of concern (VOC). Publicly funded access to nucleic acid amplification tests (NAATs) or rapid antigen tests (RATs) is displayed below the X-axis. For details on public health measures, vaccines, schedules and coverage estimates, see Appendix 1, Supplementary Material 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.221335/tab-related-content. *Nonessential travel discouraged, health care service delivery adjusted, public gatherings > 50 people prohibited. Provincial state of emergency declared. †Interactions limited to households or “core bubble” (immediate family or those in same dwelling) or to a maximum of 2 other people if living alone. ‡Dine-in food services and indoor fitness activities banned, only essential travel permitted. §Gradual return to gatherings, recreational travel, in-person work, which was interrupted by the fourth wave. ¶Indoor and personal gatherings limited, 50% capacity limit at venues of > 1000 people, sports tournaments paused. Social restrictions lifted during epidemiological week 7, 2022. **Mask mandates lifted during epidemiological week 10, 2022. ††The first 2 spike-based mRNA vaccine formulations were authorized during epidemiological weeks 50 and 52, 2020, respectively, with mRNA vaccines comprising most doses (> 90%) administered in BC and Canada across the pandemic. In epidemiological week 8, 2021, a chimpanzee adenoviral-vectored (ChAdOx1) vaccine was also authorized. ‡‡Vaccines (mRNA) initially deployed to high-risk individuals, including residents and staff of long-term care and assisted-living facilities, essential visitors within those settings and health care workers. §§Community-based vaccine roll-out, prioritized by age, beginning with the oldest adults in mid-March 2021. Access to booster doses followed similar prioritization sequence, inclusive of clinically extremely vulnerable individuals of any age. ¶¶Single-dose vaccine card required for entry into social and recreational settings starting in epidemiological week 37, 2021; 2-dose cards were required beginning in epidemiological week 43, 2021. Vaccine cards were ultimately repealed in epidemiological week 14, 2022.
MethodsStudy design and settingEight cross-sectional serosurveys were undertaken between March 2020 and July–August 2022 in the Lower Mainland (Greater Vancouver and Fraser Valley) region of BC, where about 60% of the provincial population (of about 5 million) resides.8,9 The timeline of SARS-CoV-2 serosurveys in relation to pandemic waves, publicly funded nucleic acid amplification testing, vaccine roll-out and other mitigation measures are shown in Figure 1, with additional details provided in Appendix 1, Supplementary Material 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.221335/tab-related-content.11–13
Sampling approachWe obtained anonymized residual sera from children and adults visiting LifeLabs, the only outpatient laboratory network in the Lower Mainland. Two health authorities are responsible for surveillance in the Lower Mainland, namely the Fraser Health Authority (population 1.9 million) and Vancouver Coastal Health Authority (population 1.2 million).8,9 Residents of either health authority could participate, with eligible municipalities shown in Appendix 1, Supplementary Figure 1. At each serosurvey, a convenience sample of sera was selected by age group, equally by sex, from the LifeLabs central processing centre. For the first 2 serosurveys, we sampled 100 sera per age group, but thereafter, sampling increased to 200 per age group (< 5 yr, 5–9 yr, 10–19 yr, 20–29 yr, 30–39 yr, 40–49 yr, 50–59 yr, 60–69 yr, 70–79 yr, ≥ 80 yr).14 We excluded people who were specifically seeking SARS-CoV-2 antibody testing (which was limited in BC) and residents of long-term care, assisted-living or correctional facilities because of different pre-test likelihood of positivity.
Serological testingAt each serosurvey, we used at least 3 commercially available chemiluminescent immunoassays that targeted spike (S1) or nucleocapsid (NP) proteins.15,16 For seroprevalence estimation, we defined seropositivity as a signal above the manufacturer’s cut-off threshold on at least 2 chemiluminescent immunoassays (i.e., dual-assay positivity). Before the availability of S1-based vaccines,13 we assumed any dual-assay seropositivity to be from infection. From January 2021, infection-induced seropositivity required that at least 1 of the 2 positive assays included anti-NP detection.
We undertook serological testing in real time, with adjustment based on evolving understanding of assay characteristics and their local availability. For the first 3 serosurveys in 2020, we screened sera with Ortho (S1 total antibody) and Abbott (NP immunoglobulin [Ig] G) assays at the BCCDC Public Health Laboratory. For specimens positive on either of these assays, we also tested with the Siemens (S1 receptor-binding domain IgG/IgM) assay. With vaccine roll-out, anti-NP detection became more important, but concerns related to waning antibody levels and reduced anti-NP sensitivity also arose, particularly for the Abbott assay.17–21 For the fourth and fifth serosurveys, we supplemented testing with the Roche (NP total antibody) assay at the Providence Health Care Special Chemistry Laboratory, as volume permitted. In the event a specimen returned discordant results on the Abbott and Roche NP assays, we accepted anti-NP positivity on either assay (in conjunction with anti-S1) as evidence of infection. For the sixth and seventh serosurveys, all sera were tested by Ortho, Siemens and Roche assays. By the eighth serosurvey, BCCDC no longer offered Ortho testing, replacing it instead with the Abbott (S1 receptor-binding domain IgG) assay.15,16,22
Statistical analysisSeroprevalence estimationWe assessed 2 seroprevalence categories: any seroprevalence (induced by vaccine, infection or both), defined by any dual-assay positivity, and infection-induced seroprevalence, also defined by dual-assay positivity but requiring both anti-NP and anti-S1 detection. Detection of anti-NP indicated infection-induced antibody as no vaccines used in Canada contained NP antigen. Primary seroprevalence estimates with 95% credible intervals (CrIs) were based on Bayesian analysis,23–25 standardizing for age, sex and health authority. We derived cumulative and period-specific estimates, the latter conservatively reflecting the rate of new infections between specified serosurveys under the assumption of no meaningful waning of antibody levels and no reinfections. Bayesian methods are detailed in Appendix 1, Supplementary Material 2. High assay sensitivities and specificities have been reported for each chemiluminescent immunoassay, 15,16,22,26 but typically without addressing potential variation by vaccination status, time since exposure, severity or age.27–29 Like others,30,31 we did not adjust for sensitivity or specificity in the primary analyses but explored their effects as outlined in Appendix 1, Supplementary Material 2, based on assumptions detailed in Appendix 1, Supplementary Material 3.
Surveillance underascertainment ratiosAll cases of SARS-CoV-2 confirmed by nucleic acid amplification testing were laboratory-reportable to local public health authorities and to BCCDC. Provincial surveillance reporting excluded reinfections and those positive only by rapid antigen test.11 We used infection-induced seroprevalence estimates and health authority–specific population census statistics to derive the estimated number of infections in the Lower Mainland. We derived surveillance underascertainment ratios with 95% CrIs by dividing estimated infections by surveillance reports from both health authorities, including cumulative and period-specific surveillance underascertainment ratios, the latter assuming no reinfections as per surveillance reporting. Additional methodological details are provided in Appendix 1, Supplementary Material 4, including exploratory investigation that included reinfections as 10% or 25% of all infections.
Ethics approvalSera were provided to BCCDC under legal order of the Provincial Health Officer (B.H.), and the study was approved by the University of British Columbia Clinical Research Ethics Board (H20–00653).
ResultsOf 14 000 sera collected, 13 765 (98.3%) contributed to the study. Of 235 sera excluded owing to insufficient volume, 215 (91.5%) were collected during the earliest 2 serosurveys, mostly (n = 189, 80.4%) from children younger than 10 years (Table 1 and Appendix 1, Supplementary Table 1).
Table 1:SARS-CoV-2 seroprevalence survey and participant characteristics
Age and sex distributions reflected the Lower Mainland source population (Table 1 and Appendix 1, Supplementary Table 2). Sera disproportionately came from the Fraser Health Authority (59%–74% by serosurvey) compared with the proportion of this health authority’s population in the Lower Mainland (61%), notably among children younger than 10 years (Appendix 1, Supplementary Table 3). The Fraser Health Authority also reported disproportionately more cases of SARS-CoV-2 (about two-thirds) of Lower Mainland SARS-CoV-2 cases (Figure 1).
SeroprevalenceAny seroprevalenceOverall vaccine- and infection-induced seroprevalence remained 1% or lower through the first 3 serosurveys to September 2020, and was less than 5% by the fourth serosurvey in January 2021 (Figure 2, Table 2 and Appendix 1, Supplementary Table 4). Seroprevalence rose to 56.2% by May–June 2021 (fifth serosurvey) and was higher with increasing age, consistent with age-prioritized vaccination, except among the oldest adults (≤ 70 yr) who were the earliest vaccinated by age (Appendix 1, Supplementary Material 1). By September–October 2021 (sixth serosurvey), overall seroprevalence reached 82.7%, reflecting increased vaccination of younger adults and adolescents, as well as delivery of second doses (Appendix 1, Supplementary Material 1). By March 2022 (seventh serosurvey) and July–August 2022 (eighth serosurvey), seroprevalence reached 95% or more, reflecting both higher vaccination (including third doses) and infection rates.
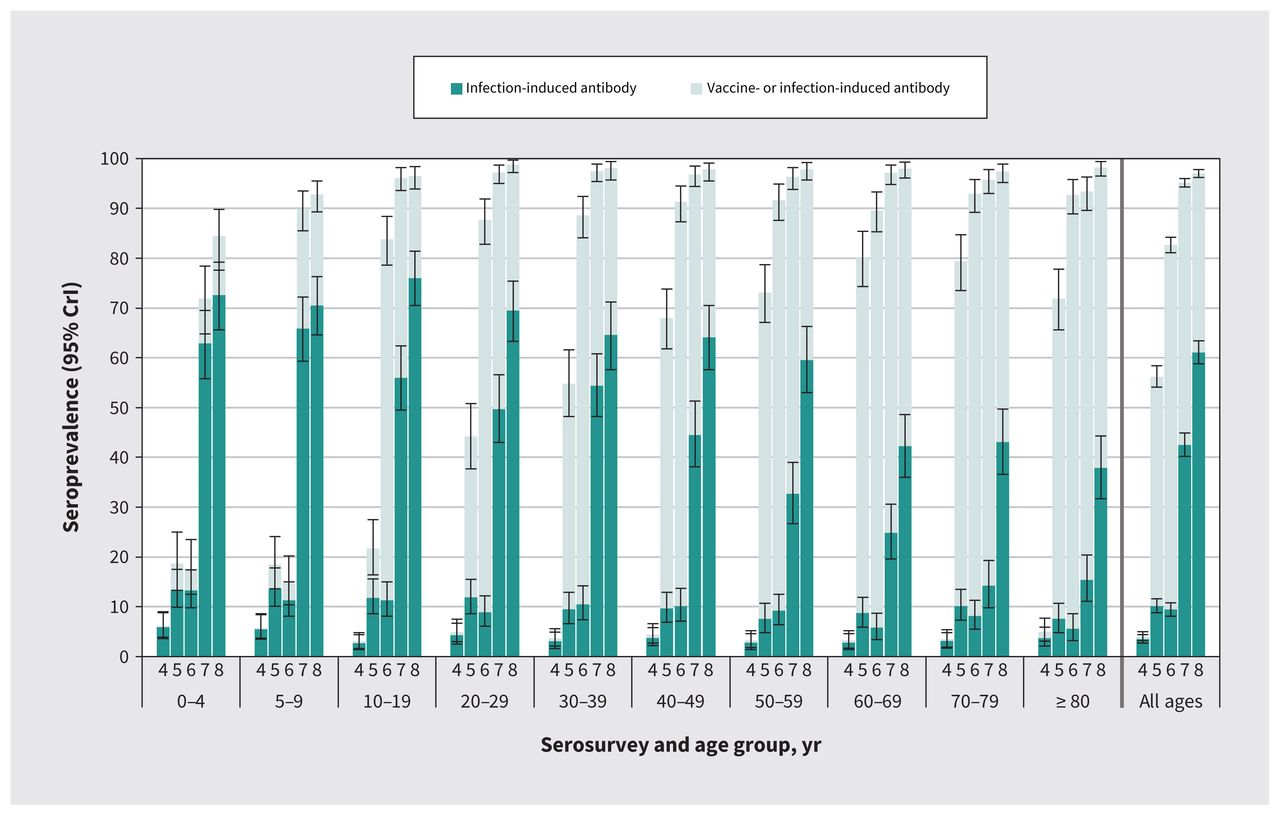 Figure 2:
Figure 2: Seroprevalence (any and infection-induced) by age group and serosurvey (serosurvey 4 in January 2021, serosurvey 5 in May–June 2021, serosurvey 6 in September–October 2021, serosurvey 7 in March 2022, serosurvey 8 in July–August 2022). Darker bars represent the infection-induced seroprevalence, which may or may not include vaccinated individuals. Lighter plus darker bars together provide a combined estimate of “any” seroprevalence (vaccine-induced, infection-induced or both). Displayed seroprevalence estimates are based on Bayesian analysis, standardized for age, sex and health authority within the Lower Mainland, British Columbia, Canada. Analysis details are in Appendix 1, Supplementary Material 2, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.221335/tab-related-content. Full results are in Table 2 and Appendix 1, Supplementary Table 4 (any seroprevalence) and Appendix 1, Supplementary Table 5 (infection-induced seroprevalence). Note: CrI = credible interval.
Table 2:SARS-CoV-2 seroprevalence by serosurvey and category (any or infection-induced), by age group
Infection-induced seroprevalenceCumulative infection-induced seroprevalence remained less than 15% overall through September–October 2021 (sixth serosurvey) (Figure 2, Table 2 and Appendix 1, Supplementary Table 5). At least one-third were newly infected between the sixth and seventh serosurveys (Figure 3 and Table 3), with cumulative infection-induced seroprevalence reaching 42.5% by March 2022. Thereafter, one-fifth were newly infected between the seventh and eighth serosurveys, with 61.1% having evidence of previous infection by the July–August 2022 serosurvey.
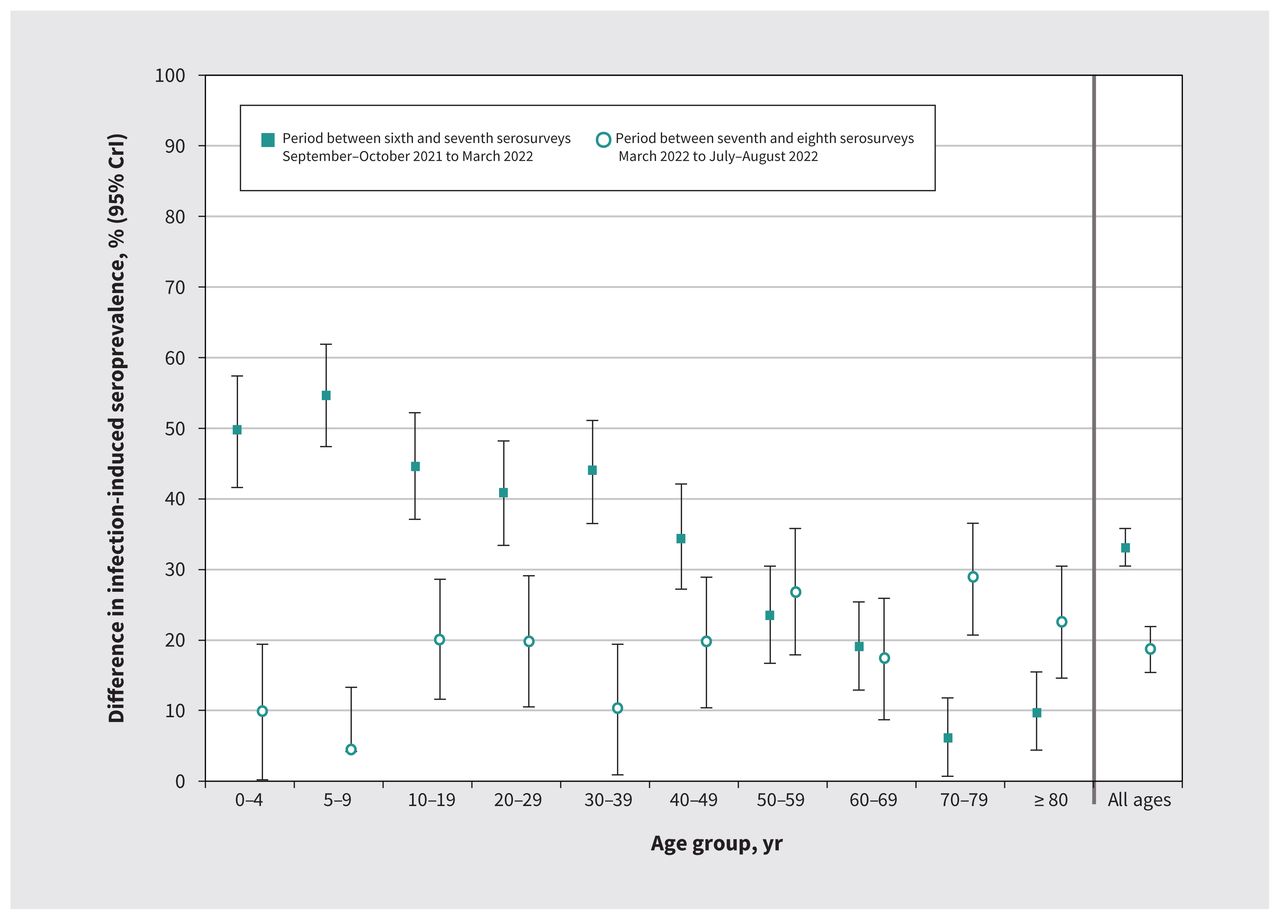 Figure 3:
Figure 3: Difference in infection-induced seroprevalence by age group between the sixth and seventh (September–October 2021 to March 2022), and the seventh and eighth (March to July–August 2022) serosurveys. Displayed seroprevalence estimates are based on Bayesian analysis — standardized for age, sex and health authority within the Lower Mainland, British Columbia, Canada — and are predicated on the assumption of no reinfections and no antibody waning. In that context, estimates represent the rate of new infections between specified serosurveys, stratified by age group. Analysis details are in Appendix 1, Supplementary Material 4, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.221335/tab-related-content. Full results are in Table 3 and Appendix 1, Supplementary Table 9. Note: CrI = credible interval.
Table 3:Period-specific seroprevalence and surveillance underascertainment ratio estimates between the sixth and seventh and the seventh and eighth serosurveys
Infection-induced seroprevalence decreased with increasing age. In general, age groups with the highest period-specific infection rates between the sixth and seventh serosurveys had the lowest rates between the seventh and eighth serosurveys. The highest rate of new infections was between the sixth and seventh serosurveys for all age categories younger than 50 years, whereas adults aged 70 years and older had their highest rates of new infections between the seventh and eighth serosurveys. Adults aged 50–59 and 60–69 years had comparable rates of new infection during both periods.
About half (45%–55%) of children aged 0–4, 5–9 and 10–19 years were newly infected between the sixth and seventh serosurveys (Figure 3 and Table 3). Rates of new infections were slightly lower (34%–44%) but with overlapping 95% CrIs among young adults aged 20–29, 30–39 and 40–49 years. Cumulatively, more than half of children were already infected by March 2022, reaching about three-quarters (70%–76%) by August 2022; rates were comparable or slightly lower (64%–70%), with overlapping 95% CrIs, among young adults (Figure 2 and Table 2). By March 2022, less than one-quarter (14%–25%) of older adults aged 60–69, 70–79 or 80 years and older had been infected. With their highest period-specific infection rates between the seventh and eighth serosurveys, still fewer than half (38%–43%) of these older adults were infected by July–August 2022.
Estimates of any seroprevalence were comparable by health authority, but infection-induced estimates were consistently higher for the Fraser Health Authority (Appendix 1, Supplementary Tables 4 and 5). Seroprevalence estimates did not differ meaningfully when stratified by sex (Appendix 1, Supplementary Tables 4–7). Crude and Bayesian-adjusted estimates were similar (Appendix 1, Supplementary Tables 4–7), and are also shown by individual assay in Appendix 1, Supplementary Table 8.
Surveillance underascertainment ratiosSurveillance case reports underestimated infections by 12-fold between the sixth and seventh and 92-fold between the seventh and eighth serosurveys, more than in previous periods (Table 3, Figure 4 and Appendix 1, Supplementary Table 9). Surveillance underascertainment ratios were highest among children aged 10–19 years and lowest among adults aged 80 years and older, with overlapping 95% CrIs between most other pediatric and adult age groups. Cumulative surveillance underascertainment ratios by serosurvey are also shown in Appendix 1, Supplementary Table 10.
 Figure 4:
Figure 4: Period-specific surveillance underascertainment ratios (SUARs), overall and by age group between (A) the sixth and seventh (September– October 2021 to March 2022) serosurveys, and (B) the seventh and eighth (March 2022 to July–August 2022) serosurveys, Lower Mainland, British Columbia, Canada. Precise values, including period-specific surveillance case report tallies, new infection rates and SUARs, are in Table 3 and Appendix 1, Supplementary Table 9, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.221335/tab-related-content. Note: CrI = credible interval.
Exploratory sensitivity analysisAdjustment for assay sensitivity and specificity had little impact on estimates of seroprevalence or surveillance underascertainment ratios (Appendix 1, Supplementary Table 11 and Table 12). Assuming reinfections constituted as much as one-quarter of all period-specific infections did not affect the order of magnitude of estimates of surveillance underascertainment ratios between the sixth and seventh (16-fold), or the seventh and eighth serosurveys (123-fold) (Appendix 1, Supplementary Table 13).
InterpretationThrough 8 serosurveys spanning the first 2.5 years of the COVID-19 pandemic, we chronicled evolution of pediatric and adult seroprevalence in the Lower Mainland, BC. During the first year of the pandemic, when extraordinary measures were in place to curtail transmission, virtually everyone remained immunologically naive. Thereafter, age-based vaccine roll-out dramatically changed the immunoepidemiological landscape such that, by September 2021, more than 80% of the study population had antibody evidence of immunological priming, while more than 85% remained uninfected. By August 2022, after a series of Omicron waves, overall vaccine and infection-induced seroprevalence exceeded 95%, with 60% having been infected, including at least three-quarters of children but less than half of older adults.
Multiple immunological, epidemiological and modelling studies suggest that having had both vaccination and infection exposures contributes to stronger, broader and more durable hybrid immunity than with either exposure alone, especially against severe outcomes.32–47 The extent to which such exposure history should guide recommendations regarding booster doses depends on several factors, recognizing that a large proportion may not even be aware of their previous infection status.48 Moreover, the antigenic relatedness and immunological interactions between previously infecting viruses, the original monovalent vaccines, more recently updated bivalent vaccine strains, and currently circulating or emerging variants are complex and dynamic. Overall, our age-related findings to date are consistent with children being the least vaccinated and most infected subgroup, whereas older adults are the most vaccinated and least infected. Although everyone may benefit somewhat from additional vaccine doses, the relative incremental value of boosting by age depends on individual- and population-level risk assessment, notably related to severe outcomes. Over the longer horizon, the determinants and potential impact of post-COVID-19 conditions may further add to the complexity of risk assessment.49–53 Amidst this uncertainty, however, the prioritization of older adults, who are still at greatest risk of severe outcomes, remains most consistent with immunization goals to prevent serious morbidity and preserve health care capacity as the 2022–23 respiratory virus season begins.11,13
A strength of our serosurveillance approach is our sampling all age groups and both sexes simultaneously, enabling their direct comparison and extending the information available from more restricted population subsets (e.g., prenatal sera from women of childbearing age, or blood donors who are mostly younger adults). We found the highest infection rates among children, closely followed by young adults, which may reflect their greater interconnectedness, including between siblings and parents in the household, as well as with peers in schools and the community.54–56 The lowest cumulative infection rates were among older adults, which may reflect their greater vaccination rates and social isolation. Their increased rate of new infections between March and August 2022, after relaxation of public health measures and societal reopening, may reflect their lower likelihood of having previously acquired hybrid (vaccine-plus infection-induced) immunity.
In the United States, similar age-related gradation in accumulated infection rates (highest in children and lowest in older adults) has been reported.57 Pediatric seroprevalence estimates elsewhere in Canada are limited. Among children aged 17 years and younger who attended emergency departments in the Greater Montreal Area, 50%–60% had detectable anti-NP by June 1, 2022,58 similar to what we observed in March 2022, but lower than what we observed in July–August 2022. Differences may reflect provincial variation in the implementation of public health measures such as school closures or masking requirements. 59 Among Canadian adult blood donors 17 years of age and older, 54% had serological evidence of infection by the end of July 2022; estimates were highest among younger adults aged 17–24 years (71%) and lowest among adults aged 60 years and older (38%), which is also similar to our own findings.60,61
Our serosurveillance findings showed substantial underestimation of infections by standard case-based surveillance reporting, notably during the post-Omicron period. More restricted access to nucleic acid amplification testing and abundant community access to nonreportable rapid antigen testing likely contributed to underascertainment. Although other surveillance indicators may be warranted, including those for which access to testing is more consistent (e.g., among patients admitted to hospital) or sustainable (e.g., wastewater sampling), the derivation of severe outcome risks per SARS-CoV-2 case still requires accurate case tallies. In that regard, ongoing serosurveillance and associated estimates of surveillance underascertainment ratios are needed to inform the magnitude of increase in case denominators (and commensurate fold-decrease in severe outcome risks per case) required for accurate risk assessment and the optimal targeting of interventions.
LimitationsBy assuming no antibody waning or reinfection, our cumulative and period-specific infection-induced seroprevalences are likely underestimates and may best be summarized as “at least” that percentage infected. Among children younger than 5 years, discrepancy between our estimates of any and infection-induced seroprevalence by August 2022 may be a measure of such underestimation, given their very recent vaccine eligibility and negligible vaccine coverage. As vaccination may reduce viral loads, underestimation of infection-induced antibody may be greater among more highly vaccinated individuals.62,63 To improve upon anti-NP detection, we used both Abbott and Roche assays beginning in January 2021 (as described in Appendix 1, Supplementary Table 1), switching to the latter (with its improved sensitivity) for the final 2 serosurveys, when waning antibody levels may have been a greater concern.17–21 Convenience sampling is inherently subject to bias, but we show good concordance in the age and sex profiles of our participants with our source population, which we further standardized in Bayesian analyses. We cannot comment on discrete ethnic or socioeconomic groups who, although not specifically excluded, were also not specifically evaluated. Residual clinical specimens are more likely to come from people with underlying comorbidities who may differ in their exposure risk and immune responses, which could contribute to an underestimation of infection-induced seroprevalence, as would our exclusion of individuals who were specifically seeking SARS-CoV-2 antibody testing. In the other direction, sera collected in the follow-up of post-COVID-19 sequelae may have contributed to some overestimation. All surveillance data, as used here in estimation of surveillance underascertainment ratios, are subject to incomplete or missing information. Given our assumption of no reinfections, the higher the actual rate of reinfection, the greater the extent to which our surveillance underascertainment ratios may be conservative underestimates; however, in exploratory analyses in which we allowed reinfections to comprise as much as 25% of all infections, period-specific estimates were of similar order of magnitude. Finally, extrapolation to other geographic areas should take into account the specific context we provide here, such as in-person school attendance, mask mandates, vaccination program adjustments and other mitigation measures that may differ elsewhere.
ConclusionBy August 2022, most children and adults younger than 60 years in the Lower Mainland, BC, had acquired evidence of both SARS-CoV-2 vaccination and infection, which likely provides stronger, broader and more durable hybrid immunity than either exposure alone, especially against severe outcomes. With the lowest infection rates but highest risk of severe outcomes, older adults continue to warrant prioritized vaccination.
AcknowledgmentsThe authors acknowledge the serological testing oversight and contribution of the British Columbia Centre for Disease Control (BCCDC) Public Health Laboratory and Providence Health Care Special Chemistry Laboratory, including Tamara Pidduck, Jesse Kustra, Laura Burns, Gahyun Cheon and Bonny So. They thank Rhonda Creswell and Iva Tong of LifeLabs for diligent supervision of serum collection; Dr. Manish Sadarangani for his co-leadership of the SARS-CoV-2 Immunity Study referenced in Supplementary Material 3; and Dr. May Ahmed, Hannah Caird and Macy Zou for their supportive surveillance analyses at the BCCDC, as well as the many other frontline, regional and provincial practitioners, including clinical and public health providers, epidemiologists, medical health offficers and others for their significant contributions to surveillance case reporting and COVID-19 control measures in British Columbia.
FootnotesCompeting interests: Danuta Skowronski reports grants from the Canadian Institutes of Health Research and the British Columbia Centre for Disease Control Foundation for Public Health, paid to her institution, for other SARS-CoV-2 work. Romina Reyes is chair of the BC Diagnostic Accreditation Program committee. Mel Krajden reports grants paid to his institution from Roche, Hologic and Siemens. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Danuta Skowronski, Samantha Kaweski and Suzana Sabaiduc contributed to the conception and design of the work. Samantha Kaweski, Shinhye Kim, Suzana Sabaiduc, Bonnie Henry and Romina Reyes contributed to data acquisition. Samantha Kaweski, Michael Irvine, Erica Chuang, Mieke Fraser, Suzana Sabaiduc, Paul Levett, Martin Petric, Mel Krajden and Inna Sekirov contributed to data analysis. Danuta Skowronski, Samantha Kaweski, Michael Irvine and Bonnie Henry contributed to data interpretation. Danuta Skowronski drafted the manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: Funding was provided in part by the Public Health Agency of Canada (Grant number: 2021-HQ-000067) and the Michael Smith Foundation for Health Research (Grant number 18934). The views expressed herein do not necessarily represent the views of the Public Health Agency of Canada.
Data sharing: Data sharing will be considered upon reasonable request to the corresponding author with appropriate review and aggregation, as required to comply with the provincial legislation under which the data were assembled, and respecting privacy and confidentiality requirements.
Accepted October 27, 2022.This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
留言 (0)