
記住我









Healthcare-Associated Infections (HAIs) Are one of the major threats to hospitalized patients and a major public health burden. HAIs are nosocomial-acquired infections that are not present or incubating in the patient on their hospitalization but they should manifest at least 48 h after admission to the hospital (1–3). HAIs are considered those infections acquired in any healthcare facilities such as hospitals, nursing homes, ambulatory, rehabilitation centers, and any other facilities, both public or private, which provide healthcare or diagnostic service to individuals (4). HAIs have become one of the major challenges for the healthcare services of western countries due to an aging society and the increased level of immunocompromised patients in healthcare facilities, in particular for those in intensive care units (ICUs) (1, 5–8). HAIs incidence increase with prolonged hospitalization and with the utilization of invasive life-prolonging procedures including venous and arterial catheterizations, tracheal intubation, urinary catheterization, invasive intracranial pressure monitoring, and placement of sterile site drainage catheters (1, 5, 6, 9). Moreover, HAIs represent one of the most frequent complications of hospitalization worldwide, with an annual incidence ranging approximately from 5 to 15% of all hospitalized inpatients. Consequently, increasing attention has been given to HAIs by government health institutions (for instance the European Centre for Disease Prevention and Control and the Centre for Disease Control) which have implemented specific surveillance programs to collect data and have issued regulations for the mandatory reporting of such infections. In Europe, every year, more than 4 million people developed HAIs, with 16 million (6%) additional hospital days and ~37.000 deaths. In Italy, specifically, between 450 and 700 thousand people are affected by HAIs every year. According to a 2013 national prevalence study, the prevalence of patients with at least one HAI is 6,3% (1, 10–15).
Given the clinical impact and the costs associated with HAIs, current research in this field is aimed to develop protocols for HAIs prevention or management and among the different possible solutions the first suggested was a more accurate hygiene protocol (1, 2, 15). Everything started in 1846, with Ignaz Semmelweis and his contributions in terms of hand washing, so much so that since then hand hygiene has been proposed multiple times as an important solution to control the spread of HAIs (10, 16). Nevertheless, proper hands washing is observed in < 40% of cases–even in units with critically ill patients–due to poor bath-room placement, lack of time, forgetfulness or rejection of the usual recommendations, or negligence (17–19). Therefore, since HAIs arise from complex systems influenced by many factors, it is needed a more pluralistic approach for proper infection control, which cannot be limited to hand washing but should involve a multidisciplinary team including hospital doctors, infection control nurses, microbiologists, architects, and engineers with expertise in building design and facilities management.
Among the factors which influence the development of HAIs, there are the biological characteristics of the infectious agents involved as well as the susceptibility of the host to both exogenous and endogenous microorganisms (5, 20, 21). The human body harbors trillions of microbes that form a diverse ecosystem including bacteria, viruses, fungi, and protozoa; in particular, collectively they are named “human microbiota” and their genomes are referred to as the “human microbiome” (22–26). Previous studies had argued that, within the human body, microbial cells outnumber human cells 10-fold (27, 28), but recent research has demonstrated that the microbial cells are abundant as the human ones, with a more realistic ratio of about 1.3 between the former and the latter (29). The human microbiome plays an essential role in health, lipid metabolism, colonization resistance to transient organisms, and immune response (30–32) and can be influenced by different factors such as body location (33, 34), diet (35), sex (36, 37), ethnicity (38), and age (38, 39). In addition, the microbial community can also be shaped by habits (40), relationships (41, 42), disease state (43, 44), and environment (42, 45). With the latter a bidirectional influence exists; indeed, on the one hand, the environment can influence the microbiota of people who live there, on the other hand, humans release their bacteria into the surrounding environment, changing its microbial composition (27). Moreover, the Human Microbiome Project and other studies on the human microbiome have revealed a wide diversity in composition and abundance of the microbiome within an individual (alpha diversity) with differences that appear consistent between individuals (beta diversity) (33, 34, 46). In terms of human microbiome complexity, the increased number of studies on the human microbiome and the huge contribution to defining the role of the microbiome in health and diseases allowed us to highlight the direct/indirect mechanisms of action with which the microbiota act to confer protection against pathogens (7). Once pathogens entered the organism, in addition to the protection conferred by the microbiota, antimicrobial therapies could be useful were it not for the increased number of antimicrobial-resistant (AMR) microorganisms (47, 48). Nowadays, despite gram-negative bacteria remain still being associated with HAIs, gram-positive bacteria (such as Enterococci and Staphylococcus epidermidis) have become most frequently associated with HAIs in the context of both surgical site or bloodstream infection (1, 48). However, despite all these changes and the identification of the high number of possible factors (such as host genetics, age, nutrition, and environment) which can influence the human microbiota and its role in health and disease, it is poorly understood what “healthy microbiota” really means (24, 46). Therefore, this systematic review aims to analyze in detail how variations in the microbiome can be associated with HAIs. In particular, studies on the microbiota of patients, healthcare environment (HE), medical equipment, or healthcare workers (HCW) and how it could be transmitted among the different subjects will be analyzed in order to define alarming factors for HAIs spreading and to identify strategies for HAIs control or prevention.
Methods Research parametersThis systematic review was performed in adherence to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (49). A systematic literature review regarding HAIs, the related microbiota, and methods for HAIs control and prevention was conducted using public electronic databases (PubMed and Scopus).
The works were selected according to the query: ((((“Healthcare-associated infection”) OR (“Healthcare-associated infections”)) AND (microbiome)) OR (((“nosocomial infection”) OR (“nosocomial infections”)) AND (microbiome))) AND ((control) OR (prevention)). One of the reviewers (A.D.) carried out the initial search of the papers and the consensus of research supervisors (L.C. and P.T.) was required.
Inclusion and exclusion criteriaInclusion criteria were as follows: (1) English language; (2) Date of publication, i.e., articles published from 2000 to 2022; (3) Availability of both abstract and full text; and 4. only articles dealing with the role of the microbiome in the prevention of HAIs in healthcare facilities settings.
Papers have been excluded applying the following exclusion criteria: (A) systemic reviews or any other works (for instance chapter of a book) which is not experimental or which did not analyse the relationship among HAIs and the microbiota of different sources such as HCW, patients, HE or healthcare instrumentation (HI – medical equipment); (B) articles which are focussed on fungi or virus and not on bacteria; (C) articles which explained how HAIs are treated highlighting the emergence of new drugs; (D) articles which considered HAIs without an overview of the microbiota correlated; (E) articles which analyzed the microbiota of patients but in infections or other diseases which are not HAIs or; (F) articles which included content not relevant to the aim of the review.
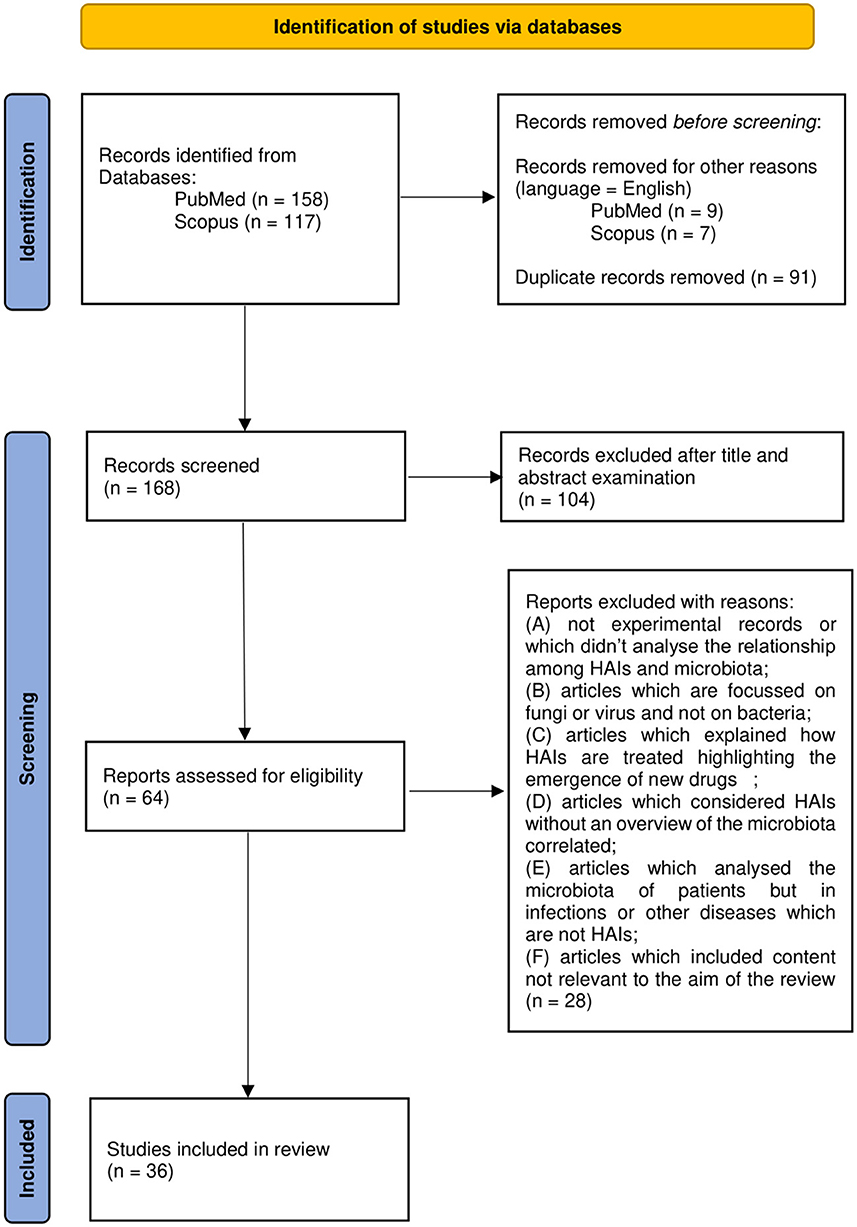
Research workflowA total of 272 works were identified through database searching. An English language filter was applied to start the screening process and narrow the search to 256 works. Duplicates (91 works) were removed manually. Then, the process continued through the screening of titles and abstracts which was followed by the evaluation of the full text of those works not excluded on the basis of the latter.
A total of 165 works were thus examined on the basis of title and abstract. A total of 62 articles were further evaluated by full-text examination to exclude irrelevant content based on the previous criteria (A-F). After a full-text reading of the selected papers, 36 were considered eligible and included in the review. Results management was performed with the use of Microsoft Office software such as Excel and Word. Zotero software was used to edit and organize the bibliography. The PRISMA flow chart in Figure 1 summarizes the workflow of the screening and selection process described above.
Figure 1. Preferred Reporting Items for Systemic Reviews and Meta-Analyses (PRISMA) 2020 flow diagram.
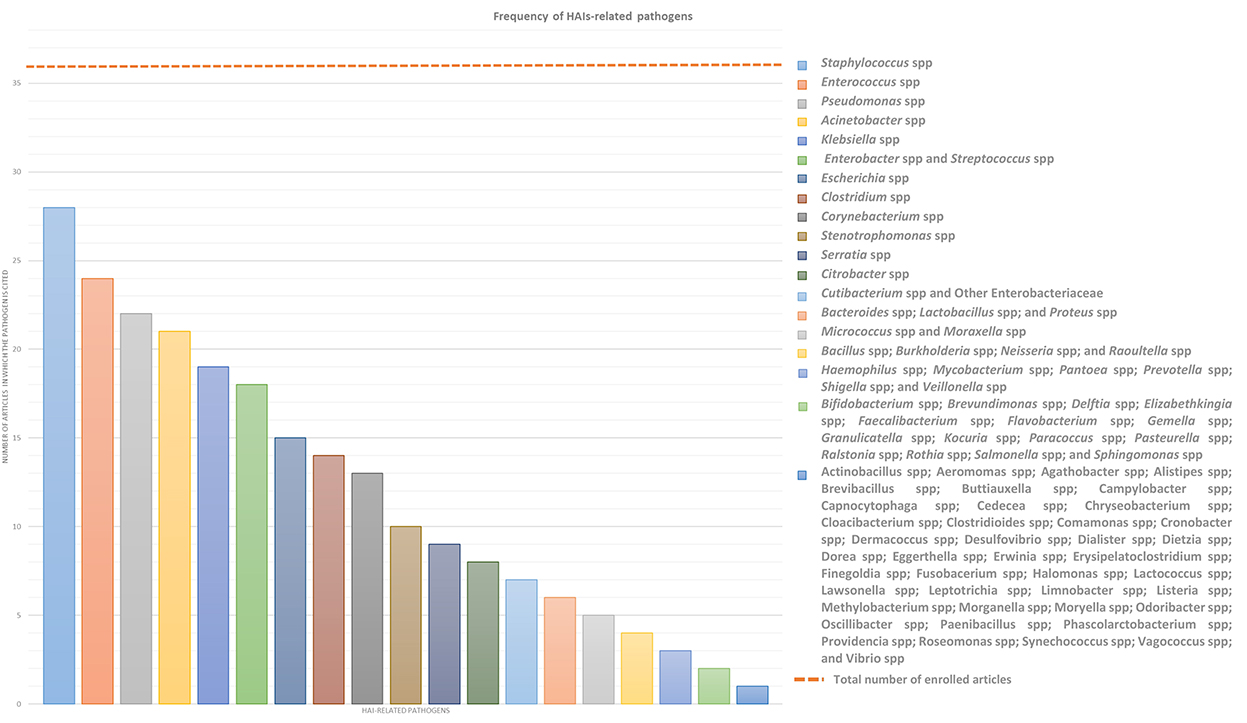
ResultsThis systemic review analyses in detail different studies, which deal with the association between microbiota and HAIs focusing on different types of microbiota, such as that of HCWs, patients, or HE, in order to define alarming factors for HAIs spreading and to identify strategies for HAI control or prevention. Over the years, new technologies such as next-generation sequencing (NGS) technologies have emerged, allowing a deeper and more precise understanding of microbiome in different contexts, providing specific knowledge toward new guidelines for combating HAIs and thus promoting and improving citizens' health. In this sense, a multifaceted approach is required and the analyses of the many factors, which can influence HAIs onset, could be a good starting point. In this review, we will focus mainly on the localization, transmission, and prevention of “ESKAPE” bacteria (Enterococcus spp, Staphylococcus aureus, Klebsiella spp, Acinetobacter spp, Pseudomonas aeruginosa, and Enterobacteriaceae) and Clostridium difficile, which are the most common pathogens causing HAIs, despite sometimes we will present a wider microbiota landscape (Figure 2). In order to provide the reader with a better understanding, we grouped the selected studies on the basis of the relationship of HAIs with seven categories: (a) HCWs microbiota and HAIs; (b) patients microbiota and HAIs; (c) HE microbiota and HAIs; (d) medical equipment microbiota and HAIs; (e) environmental factors, ecosystem, and HAIs; (f) study of transmission/cleaning and HAIs; and (g) resistome and HAIs. A summary of the results of the studies analyzed in this review is shown in Supplementary Table 1.
Figure 2. Frequency of HAIs-related pathogens. In the graph are represented the number of article out of the 36 enrolled which treated each specific pathogen to better highlight which of them result most prevalent. ESKAPE bacteria, namely Enterococcus spp, Staphylococcus spp, Klebsiella spp, Acinetobacter spp, Pseudomonas spp, and Enterobacteriaceae such as Enterobacter spp and Escherichia spp, in addition to Streptococcus spp and Clostridium spp resulted the most infective pathogens which should be controlled to prevent HAIs.
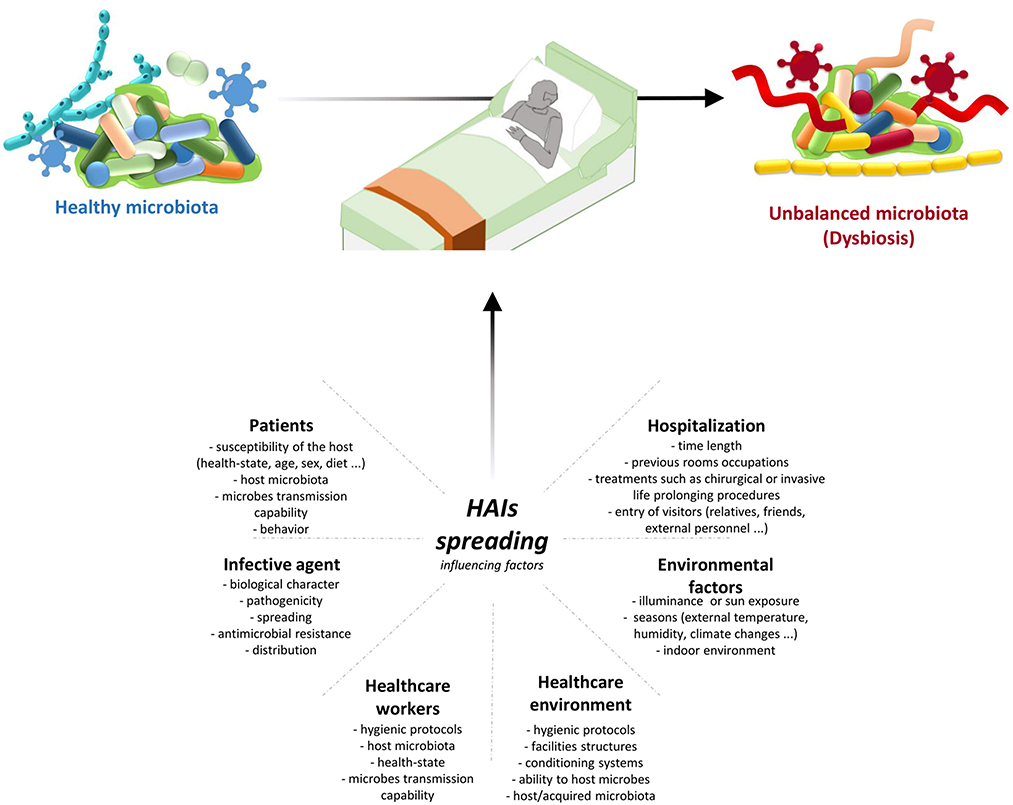
Healthcare workers' microbiota and HAIsTransmission of infection during healthcare assistance requires three elements: the source of infecting microorganisms, a susceptible host, and a means of transmission from the microorganism to the host. Infection can be endogenous when the source is represented by pathogens present within the body, but more frequently exogenous. In this case, the infection is transmitted from the outside through medical equipment or devices, the environment, healthcare personnel, or contaminated drugs (Figure 3).
Figure 3. HAIs spreading influencing factors. HAIs are mainly due to the microbiota transition from an healthy state to dysbiosis. This alterations are caused by different factors: hospitalization conditions and reason for admission; both external and internal environmental factors; HE hygienic condition and HE ability to host/acquire microbes; ability to transmit microbes by the HCWs, their healthy condition, and their propensity to follow hygienic procedures; infective agent itself; and patients healthy state and their behaviour. Therefore it is important a multifaceted approach to manage all these factors and thus HAIs spreading. HAIs, healthcare-associated infections; HCWs, healthcare-workers; HE, healthcare-environment.
There are many shreds of evidence that HCWs are one of the main risk factors involved in the large-scale dissemination of HAI-related bacteria; therefore, several studies have analyzed their implications in this context. Sereira et al. carried out the “Healthcare-associated Infections Microbiome Project,” a surveillance program of 6-month targeting, among others, HCWs, collecting 216 samples from their hands, mobile phones, and protective clothing. Through their culture-dependent and culture-independent analyses, despite the high abundance of total bacteria in the protective clothing, they observed a similar distribution of the ESKAPE bacteria investigated on the different sources identifying these sites as possible hot spots for HAI-related bacteria transmission (50). As we have previously pointed out, in addition to ESKAPE bacteria, Clostridium difficile is another important HAI-related bacteria. Shoaei et al. specifically have performed phenotypic characterization coupled with molecular typing of Clostridium difficile isolates in burned patients with diarrhea, as well as their environmental context. In particular, from the point of view of HCWs-related Clostridium difficile analyses, they collected 29 swabs from HCWs dominant hands which showed positive results for Clostridium difficile colonization in 8 samples, one of which resulted colonized by a toxigenic Clostridium difficile strain (51). A similar result was highlighted by Segal et al. They identified in an anaesthesiologist the source of contamination of post-operative infections of seven ICU patients, detecting in both patients and the anaesthesiologist the same bacteria. This result was achieved using 16S rRNA amplicon metagenomics sequencing rather than the most common cultural methods. Moreover, they observed also a correlation between the time of surgery and the severity of infection, suggesting that the number of contacts between the patient and any contaminated member of the medical team may increase the possibility for the patient to acquire that particular pathogen (52).
Since HAIs are considered as those infections acquired in any healthcare facilities, which provide healthcare or diagnostic service to individuals, and not only those acquired in hospitals, all the employers of these facilities should be considered, in this context, as HCWs. On this base, Pérez-Fernández et al. performed a descriptive observational study on 19 physiotherapy and rehabilitation centers in order to discover potential microbiological risk factors for HAIs onset. They performed sampling from the hands of physiotherapists without previously informing them to prevent influencing their behavior (hand washing in particular). The majority of the detected microorganisms were gram-positive bacteria, in accordance with the usual microbiota of the human body, suggesting the necessity of reinforcing hand washing or even combining hand washing with the use of gloves to reduce the transmission of these bacteria among different patients (53).
Cruz-López et al., in addition to studying the role of HCWs as a source of external human contamination for HAIs in-patient, have gone over identifying also the huge contribution that can be attributed to the patients' relatives. They performed sampling from 35 nurses and 8 patients' relatives. In particular, stool samples or rectal swabs and swabs of different anatomical sites as well as hands swabs were collected from the HCWs only once during the first seven days of the study, and from the patients' relatives at admission, on day 3 and then every 5 days until hospital discharge. They observed that, among the different microorganisms, coagulase-negative staphylococci represented the most frequent species recovered both in HCWs and in patients' relatives. Staphylococcus aureus and Raoultella ornithinolytica were recovered primarily from nurses. However, they identified a wider spectrum of microorganisms that could be present in both HCWs and patients' relatives, identifying them as possible asymptomatic carriers and pathogens reservoirs that can facilitate the dissemination of the pathogens in the hospital setting and that, hence, should undergo strict regulation to prevent HAIs dissemination (54).
Considering this evidence, HCWs and patients' relatives/caregivers must be considered one of the main sources of pathogen spreading in different types of healthcare facilities. More than half of HAIs are preventable, especially those associated with certain behaviors, through the planning of dedicated programs to prevent and control the transmission of infections. However, it is necessary to plan and implement control programs at different levels (national, regional, local), to ensure the implementation of those measures that have proved effective in minimizing the risk of infectious complications. Although HAIs are commonly attributable to patient variables and the quality of care provided, a dedicated organizational setup has been shown to help prevent them. Therefore, ensuring correct hygiene practices of all people involved in the patient's assistance, and the use of sterile gloves and clothing should be a fundamental strategy to ensure a higher safety level for patients, especially for the immunocompromised ones.
Patients' microbiota and HAIsHuman microbiota has a central role in many biological functions therefore its variations may represent important risk factors for HAIs onset and development. In this paragraph, we are taking into account different studies that considered the patient microbiota in order to define its correlation with HAIs onset from a general point of view or focusing on either specific pathologies or pathogens. McDonald et al. worked to confirm an earlier assumption according to which critical illness would be associated with loss of health-promoting commensal microbes with a simultaneous overgrowth of pathogenic bacteria (dysbiosis), thus increasing susceptibility to HAIs, sepsis, and multi-organ failure. They collected fecal, skin, and oral samples from 115 mixed ICU patients twice: within 48 h of ICU admission and on day 10 or at ICU discharge. First of all, they observed a greater similarity among fecal and oral samples at admission, compared to those obtained at discharge, suggesting that the length of stay in an ICU is connected with endogenous microbial community disruption. Their results confirmed the correlation between critical illness and the rapid establishment of a state of dysbiosis due to the depletion of health-promoting organisms (such as Faecalibacterium which seems to have an anti-inflammatory role), and the overgrowth of known pathogens, such as Enterobacter and Staphylococcus (55). Sereira et al. in their “Healthcare-associated Infections Microbiome Project,” collected 198 patients' samples through rectal, nasal, and hand swabbing. A high abundance of HAI-related pathogens were detected on all types of samples, however, the highest amount of bacteria and the greatest differences in alpha and beta-diversity was associated with the rectum samples. Moreover, during their studies, they concluded that 50% of the patients did not present any HAIs during hospitalization, 43.9% had an HAI during the hospitalization, and 6.1% was colonized by HAI-related bacteria, highlighting that a longer hospitalization seems to result in an increased HAIs incidence and, thereby, in an increased HAI-related pathogens detection, especially for bacteria like Klebsiella pneumoniae, Enterobacteriaceae, Staphylococcus spp, and Acinetobacter baumannii (50). Always through samples collected from different patients' body sites, Cruz-López et al. examined the colonization process and the possible ways of transmission of HAI-related pathogens, since patient colonization has been suggested as a risk factor in HAI development. They collected stool samples or rectal swabs and swabs from different anatomical sites in 11 in-hospital patients, at admission, on day 3, and every 5 days until the patient left the unit. Of these patients, 8 developed 1-3 HAIs for a total of 12 diagnosed HAIs. Since the main causative agents were identified in Acinetobacter baumanii and Klebsiella pneumoniae, the majority of HAIs (50%) were ventilator-associated pneumonia (VAP). Moreover, this study confirms the previous one, according to which the risk for HAIs-related pathogens acquisition increases with the time of hospitalization since on the 1st day of hospitalization only 50% of causative agents were recovered from patients' swabs (54).
Zakharkina et al. performed a study focused on the dynamics of the respiratory microbiome during mechanical ventilation in the ICU and its association with VAP. They collected a total of 111 samples of tracheal aspirates from 35 patients which have been divided into 4 groups: 11 patients with VAP (group 1), 9 patients without VAP but with colonized airways (group 2), 9 patients without VAP and without colonized airways (group 3), and 6 patients who developed pneumonia within 48 h after intubation (group 4). From a microbiological point of view, pathogens like Acinetobacter, Pseudomonas, and Staphylococcus were identified in patients with confirmed VAP and the duration of mechanical ventilation resulted to be associated with a decrease in microbial diversity in 83% of patients. More in detail, differences in alpha diversity were detected between group 1 and group 3 but not between groups 1 and 2. However, in group 1 patients showed a more profound dysbiosis than in group 2. Moreover, despite 27 patients receiving treatment with antibiotics at some point during their hospitalization, in this case, an association between antibiotic therapy and microbiological variations was not observed (56). Another study addressing microbial variation in mechanical ventilated ICU patients is that of Lamarche et al.; they conducted an observational study collecting samples from 34 mechanically ventilated ICU patients and from 25 healthy adults. In particular, for critically ill patients, they carried out the sampling during the 1st week of hospitalization, collecting 29 endotracheal aspirates, 26 gastric aspirates, and 10 feces specimens; whereas, for healthy adults they collected 7 bronchoalveolar lavages samples, 7 nasopharyngeal swabs, 7 oropharyngeal swabs, and 21 feces specimens. As described above, microbial dysbiosis occurred in critically ill patients, moreover, in this case, less pronounced differences in biogeographical composition, resulting in a lack of specificity between anatomical sites, were observed. Comparing ICU patients and healthy adults' operational taxonomic units (OTUs), significant differences in their abundance were shown with a strong decrease in the amount of the “health-promoting” microorganisms, in particular Faecalibacterium and Neisseria. Also, this study reiterated that in ICU patients, besides the depletion of different OTUs, there is an increase of one or few pathogenic OTUs (such as Enterococcus, Pseudomonas, and Staphylococcus genera), suggesting the microbial collapse in ICU patients toward a few dominant taxa which are usually isolated in HAIs and whose number is proportional to illness severity and mortality (22). More recently, Lu et al. focused their attention on patients with severe pneumonia, analyzing their skin microbiota composition and diversity in comparison with that of a healthy control group. They enrolled 30 mechanical ventilated ICU patients and 30 healthy staff members and collected from both groups skin surface samples and then, only from the patients, blood, endotracheal aspirates, and bronchoalveolar lavage fluid samples. From skin surface samples 14292 OTUs were identified, allowing identification of 590 genera. Staphylococcus, Acinetobacter, Corynebacterium, Stenotrophomonas, Enterococcus, Brevibacillus, and Halomonas were most abundant in the patient group, while in the healthy control group Bacteroides, Phenylobacterium, Prevotella, and Streptococcus were prevailing. However, as previously observed, patients showed also a decrease in diversity both within each sample (alpha diversity) and between samples (beta diversity). Finally, they showed an interaction between skin bacteria and respiratory microorganisms characterizing also in the other samples the same HAI-related pathogens, thereby suggesting the importance of skin microbiota along with pulmonary and gut microbiotas in the pathogenesis of severe pneumonia in ICU patients (57).
Another observational study is that performed by Mu et al. on three groups of patients (34 septic patients, 33 non-septic ICU patients, and 10 healthy adults) and 312 fecal samples. Despite the focus of their study on the gut microbiota, also in this case a significant decrease in microbiota abundance and diversity, flanked by an increase in AMR pathogens, was highlighted. Moreover, they found an association between opportunistic pathogens intestinal colonization and secondary infection development, observing a secondary infection in 23 septic patients out of 34, 14 of which resulted to be caused by Klebsiella pneumoniae, thus suggesting the central role of this pathogen in HAIs. Actually, Klebsiella pneumoniae was not the only opportunistic pathogen showing a higher abundance in both septic and non-septic ICU patient than in healthy adults; indeed, also Enterococcus strains were detected. In this study, the amount of other health-promoting bacteria, such as Faecalibacterium, was significantly lower in both septic and non-septic ICU patient than in healthy control (58).
Considering the focus on gut microbiota, in their study Lu et al. explored early intestinal colonization in very low birth weight infants (VLBWI) and how it is influenced by dominant bacteria and other factors. They collected a total of 300 anal swabs from 81 VLBWI at different times after birth until the 21st day of hospitalization. Their results showed that 188 samples out of 300 had dominant bacteria, the top five were both gram-negative bacteria (Klebsiella pneumoniae, Escherichia coli, and Serratia marcescens) and gram-positive bacteria (Enterococcus faecalis and Enterococcus faecium). However, the gram-negative bacteria resulted to be the main colonizers in VLBWI with a colonization rate that increased over time. In particular, HAIs due to both Klebsiella pneumoniae and Serratia marcescens proved to be significantly associated with intestinal colonization rather than those caused by Escherichia coli or Enterobacter cloacae. Finally, among different non-infectious factors considered in this, including gender, mode of delivery, gestational age, birth weight, feeding mode, and mechanical ventilation, only the latter was shown to be a factor affecting bacterial colonization in VLBWI, which was probably influenced also by the use of antibiotics to treat these patients (59). Also, Maamar et al. faced gut microbiota colonization but they mainly focused on a broad-spectrum cefotazime-resistant (CTX-R) Enterobacteriaceae to determine their prevalence in patients and their colonization rate during hospitalization. They enrolled 63 patients collecting different rectal swabs at admission and on a weekly basis until pathogen positive detection or hospital discharge. Firstly, at admission, 13 samples resulted to be positive for CTX-R Enterobacteriaceae indicating a prevalence of 20.63%. The following sampling was realized for only 35 patients, 15 of them acquired the pathogens during hospitalization, resulting in a CTX-R Enterobacteriaceae acquisition rate of 42.85%. In particular, CTX-R Klebsiella pneumoniae, Escherichia coli, and Enterobacter cloacae were the most frequently detected microorganisms, confirming their pathogenic role. Eventually, also Maamar et al. identified antibiotic treatment as a risk factor for pathogens acquisition (60). Since the gut microbiota of an individual can shape the local environmental surfaces, Freedberg et al. collected 304 samples from ICU patients at the time of ICU admission, 80 of which were defined as eligible to be compared with ICU rooms' microbiota. In addition to these evaluations, Enterococcaceae resulted to be overrepresented in all samples and vancomycin-resistant Enterococcus (VRE) was identified specifically in 28% of the eligible patients (61).
Ke et al. turned their attention to another important HAIs-related pathogen, Clostridium difficile. They recruited 243 participants which have been divided into four groups: 112 patients with Clostridium difficile infection (CDI), 40 asymptomatic carriers, 44 non-CDI patients with diarrhea, and 47 control patients. These authors analyzed not only gut microbial composition but also a broad panel of innate and adaptative immunological markers, suggesting that all these data taken together may allow to better distinguish patients with CDI from other groups of patients. This new association may be a new marker-derived signature to detect CDI and design early and more effective therapeutic interventions. In addition, they compared the overall microbial community structure of the four groups of patients identifying CDI ones as those with the lower alpha diversity and the higher beta diversity. Consistently with previous studies, these findings suggested a depletion of some taxa, and a significantly less stable microbiome profile characterizing CDI patients. Despite this, several driven taxa, like Klebsiella, Streptococcus, Desulfovibrio, and Veillonella, were identified as the main players in driving changes in microbial correlation networks between CDI patients and other groups and many other genera showed specific variations (62). Considering the role of Clostridium difficile, Shoaei et al. evaluated the dominant bacteria structure in burned patients with and without CDI. They collected fecal samples from 23 CDI patients, 46 burned patients without CDI, and 46 healthy control adults for a total of 189 samples, and 51 skin surface samples from burned patients. Fifty-one fecal samples showed Clostridium difficile positive results with culture methods, of which 23 had toxigenic character whereas, for the second group of samples, 14 showed positivity to Clostridium difficile culture but only two of them produced results showing colonization by toxigenic Clostridium difficile strains. More generally, they demonstrated that the gut microbiota of CDI group was characterized by an overgrowth of facultative anaerobic bacteria such as Enterococcus spp and Escherichia coli and a reduction of beneficial bacteria such as Bacteroidetes compared to other groups. Moreover, they identified that the increase in Akkermansia muciniphila and the decrease in Faecalibacterium prausnitzii may be considered predictive microbial markers for developing nosocomial diarrhea, defining a poor CDI prognosis in burned patients (51).
Ogura et al. enrolled 29 patients to characterize Staphylococcus spp on skin healed from a pressure injury. The patients were divided into two groups since 7 of them suffered from recurrent pressure injury (RPI) within 6 weeks after healing and the other 22 did not. The results showed a significantly higher abundance of Staphylococcus spp in RPI-healed sites than in non-RPI-healed sites suggesting its implication in RPI. From a genomic point of view, they demonstrated the dominance of Staphylococcus caprae and Staphylococcus aureus over Staphylococcus epidermidis, whose presence showed extremely low results in all skin sites. Moreover, despite Staphylococcus aureus seeming to appear in an earlier RPI onset, it was detected alone in only two of the seven RPI patients in comparison to Staphylococcus caprae, which was observed alone four times (63).
Given all these studies and their similarities, it is clear how patient microbial diversity may be considered as a biomarker of prognostic value for HAIs and a starting point to define targeted therapies to correct dysbiosis and health-promoting bacteria depletion, restoring a healthy microbiome and thus improving patient outcome.
Healthcare environment microbiota and HAIsSafety and hygiene of HE significantly contribute to the onset of HAIs, indeed different studies identified microbial contamination of the HE as an important source of pathogens transmission resulting in HAIs spreading. The monitoring of HE surfaces may be conducted through either the most common culture-dependent methods or culture-independent ones, which, in general, result to be faster, more effective and sensitive, and able to detect also uncultivable bacteria with the only fault being unable to distinguish viable from dead bacteria, leading to an overestimation of the contamination. Comar et al. performed one study of HE contamination using NGS technologies in comparison with conventional microbiological and molecular PCR methods, in order to define more precisely the environmental microbial composition. They collected HE samples 7 h after cleaning by contact plates for microbiological analyses and sterile swabs both for molecular ones and for NGS analyses. After sampling, 216 contact plates and 108 sterile swabs were harvested to perform microbiological, molecular, and NGS analyses, respectively. In microbiological analyses, Staphylococcus showed a microbial prevalence of 81% of the total collected samples, Enterococcus spp of 13%, Candida spp of 7.9%, Acinetobacter spp of 7.4%, Clostridium difficile of 4.2%, Pseudomonas aeruginosa of 0.9% and Klebsiella spp of 0.5%, whereas Aspergillus was never detected. Molecular analyses allowed the identification of the searched pathogens in more samples compared to the previous method. In particular, among the others, Staphylococcus was detected in 99% of the samples, Enterococcus spp in ~80%, Klebsiella pneumonia, and Enterobacter in 78%, often in association with Escherichia coli which was identified in 49% of the samples, Acinetobacter baumannii in 24%, Pseudomonas aeruginosa in 76%, and Clostridium difficile in 19%. NGS analyses allowed obtaining the following level of microbial prevalence for the most frequent pathogens: 94.5% for Cutibacterium spp, 92.6% for Staphylococcus spp, 82.4% for Streptococcus spp, 75% for Corynebacterium spp and Pseudomonas spp, 70.4% for Paracoccus spp, 65.7% for Acinetobacter spp, and 59.3% for Rothia spp. Considering all the results achieved, NGS appeared to be the only technique able to identify both searched and non-searched bacteria, with a high degree of sensitivity compared to the other two techniques, since NGS is a powerful tool for monitoring contaminating bacteria even at low concentrations (13). Another study that exploits NGS potential, rather than cultural methods, is that of Ribeiro et al., where deep-DNA-sequencing analyses were used to explore and compare the bacterial communities structures of different ICUs and neonatal intensive care units (NICUs). For this purpose, 158 samples were collected resulting in identification of 2051 OTUs for NICU and 1586 for ICU, resulting in higher diversity in the microbial composition of NICU compared to ICU, probably due to the higher transit of visitors in the former. At the genus level, sequences of 138 and 160 genera were included for ICU and NICU, respectively, among which 11 specific genera were identified as biomarkers for NICU and 6 for ICU. The HAI-related genera, which were considered biomarkers for the NICU environment by Ribeiro et al., were several facultative or obligate anaerobes, most of which, despite normal hosts of healthy adults, may be pathogenic for neonates. Instead, the main HAI-related pathogens in ICU were Pseudomonas. Collectively, these results enable to differentiate ICU and NICU environments, suggesting the central role of HCW and patients in environmental contamination since the majority of the detected pathogens are common in human microbiota (64).
Moreover, Li et al. conducted monitoring of the microbial community of ICUs. They collected 214 samples from different sites of two ICUs within a 1-year period and, then, they compared the microbial composition detected with public databases to figure out the sources of ICUs contaminations. They identified the main sources of ICUs contamination in building-related bacteria and, to a lesser extent, in human skin-related bacteria. Anyway, in addition to Proteobacteria and Firmicutes, which represent the main phyla of these two ICUs, this study showed a huge HAI-related bacteria composition characterized by Acinetobacter, Staphylococcus, Enterococcus, and Klebsiella strains (15). Again in the ICUs context, Costa et al. analyzed biofilm and ESKAPE bacteria contaminations of high-touched surfaces. Fifty-seven surfaces were selected and the samples were analyzed with four different methodologies (culture, molecular analyses, NGS, and microscopy). ICUs surfaces resulted to be contaminated by many pathogens which were identified mostly through molecular analyses rather than cultural ones, indeed from the culture-negative samples, 76.7% were shown to have live bacteria suggesting the presence of a high number of non-culturable bacteria such as those found in biofilm. Moreover, biofilms were detected in all the analyzed samples through microscopy techniques. Eventually, NGS analyses revealed a large microbial diversity with more than 830 OTUs and 170 genera, among which ESKAPE bacteria were detected in 51.8% of the NGS samples. In particular, among these HAI-related bacteria, Acinetobacter baumanii was detected in six culture-positive and five culture-negative samples, Staphylococcus aureus in three culture-positive and one culture-negative, Enterobacter spp in two culture-negative, and Pseudomonas aeruginosa in one culture-negative sample (65).
Sereira et al. during their “Healthcare-associated Infections Microbiome Project” targeted also HE in order to identify contamination hotspots, searching for specific bacteria in 666 high-touched surfaces samples. Collectively they showed that the microbial community in HE was mainly composed of Proteobacteria and Firmicutes phyla, where Enterobacteriaceae, Pseudomonas, Acinetobacter baumanii, and Escherichia coli belonged to the first phylum and Staphylococcus to the second one. Concerning hotspot sites, HCW resting rooms resulted as the most contaminated, with a high amount of both total bacteria and HAI-related bacteria. Moreover, higher diversity was shown in the unit's bathrooms as well as in bed equipment and equipment shared between hospital units (50).
Differently from Ribeiro et al. who concluded that ICUs and NICUs environment are characterized by different microbial compositions, Sereira et al. affirmed that these differences disappear over time due to the microbial community dynamicity, especially when a larger sampling size is adopted for the analyses. However, in accordance with Ribeiro et al., and Sereira et al. suggested that microbial communities which colonized HE can be influenced by patients, HCW, and the severity of illness of inpatients (50, 64). Another study, which identified in HE microbiota a possible transmission route of HAI-related pathogens, is that of Cruz-López et al. which collected environmental samples from surfaces near the patient's bed at admission, at day 3, and every 5 days until the patient's discharge. Coagulase-negative staphylococci were the most detected species also in environmental samples; however, other HAI-related bacteria were identified, such as Acinetobacter baumanii, Klebsiella pneumoniae, Enterobacter cloacae, and Enterococcus spp. HAI causative agents were recovered both before and after infection development suggesting a mutual exchange of bacteria between patients and the environment (54).
Kelly et al. studied how HE contamination may be related to the environmental position of patients and wastewater sites. They considered 51 hospital rooms at the time of patients' admission with an eligible HAI-related pathogen and then they performed a longitudinal sampling at different times in three different sites at variable distances from the patient's bed (near to the patient, intermediate distance, and far from the patient but in the proximity of wastewater sites) resulting in 408 samples. They related the probability of HAI-pathogens detection to the distance from the patient and wastewater site evidencing that the detection of gram-negative HAI-related pathogens (such as Acinetobacter spp or Pseudomonas spp) increased toward the wastewater site, while the opposite occurred for the detection of gram-positive HAI-related pathogens (such as Clostridium difficile) which increased closer to the patient. The relation between pathogens and the distance from the patient may be helpful to evinced possible hotspots of bacterial contamination (66).
Gudakova et al. analyzed microbial contamination specifically on touch surfaces of waiting rooms in pediatric outpatient facilities, to evaluate any differences between sick-child waiting rooms and well-child waiting rooms and possible hotspot sites of contamination. They collected samples from 3 pediatric offices in one or two sampling days. Taken together, their results revealed no significant differences between the two types of waiting rooms, both characterized by a high variation in microbial burden on samples collected from the same surface type. However, they highlighted that the sites with the highest microbial contamination were seats, children's seats, and children's books. Seats hosted the highest levels of Staphylococci, whereas children's books showed the highest level of both Staphylococci and gram-negative enteric bacteria. Moreover, they noted that the level of seat contamination was higher in sick-child waiting rooms in contrast to the level of children's books contamination, the results of which were higher in well-child waiting rooms. A probable explanation of these results may be connected with the different behavior of the children in the waiting rooms which is influenced by their health state (67).
A particular consideration is that also ambulances can be categorized within HE. In this context, Sheahan et al. developed a rapid, portable, inexpensive, and easy-to-use approach to metagenomics analyses to characterize ambulances microbiota. Their system allowed them to identify, on the samples collected from different ambulances at different times, six different phyla (Spirochaetes, Fusobacteria, Bacteroidetes, Actinobacteria, Firmicutes, and Proteobacteria) for a total of 68 genera, some of which contain HAI-related pathogens, such as Clostridium spp or Staphylococcus spp. In addition, other identified genera are: Campylobacter, which is a bacteria responsible for some gastroenteritis; Shigella which is associated with shigellosis disease; and Listeria, which may lead to fatal bacterial illness. Finally, by analyzing different surface samples from three different ambulances they were able to detect probable contamination hotspots, which should require fine monitoring and cleaning procedures. Overall, their approach provided a functional and rapid platform for microbial detection and monitoring in ambulances for specific pathogens, evidencing their higher prevalence on finger monitors which enter in direct contact with patients, followed by door handles which experience direct contact with the HCW, and by soft kits which are in contact with the environment (68).
Other healthcare facilities analyzed in order to discover environmental contaminations were physiotherapy and rehabilitation centers. Pérez-Fernández et al. collected four environmental samples from each of the 19 healthcare facilities under study, in particular, three samples were taken from the treatment table (head, intermediate, and caudal section) whereas the fourth sample was of the ambient air. They observed a high value of coagulase-negative staphylococci and gram-negative non-Enterobacteriaceae bacteria but lower level of Staphylococcus aureus on samples collected from tables of treatment without any relevant differences among the different tables' sections. On the contrary, Staphylococcus epidermidis, Micrococcus spp, and Bacillus spp were the only microorganisms identified in air samples. Their results suggested greater involvement of environmental surfaces rather than the ambient air in pathogen transmission since the former was shown to host opportunistic pathogens (53).
In addition to HCW and patient microbiota analyses, Shoaei et al. performed characterization of environment microbiota in rooms of burned patients after Clostridium difficile diagnosis. Of 21 bed sheets collected samples, three resulted colonized by non-toxigenic Clostridium difficile strains, therefore also in this case a correlation between environmental contamination and HAIs, such as CDI, was highlighted (51). Considering environmental contamination and VRE colonization, Freedberg et al. tried to define if there might be worse ICU rooms. Twenty-four ICU rooms were sampled at five different time points. Pseufomonaceae characterized the microbial community detected on environmental surfaces. Moreover, comparative studies to assess microbial variation across neighboring ICU rooms were performed. The rooms' microbiota slowly diverged from baseline and it appeared similar to that of neighboring rooms; however, the speed of this divergence seemed to be associated with the patients' turnover. Moreover, analyzing VRE-colonization, the authors confirmed environment-patient interactions, indeed when they showed a different VRE status in a time of 3/9 days both become VRE-positive (61).
Taken together all these studies allowed defining the central role of HE microbiota in the transmission of different HAI-related pathogens, most of which are not common environmental bacteria but rather are human-related bacteria released in the environment by the individuals who spend time in that environment.
Medical equipment microbiota and HAIsAnother important cause of HAIs has been recognized in the contamination of medical devices by pathogenic microorganisms in healthcare settings. Therefore, to reduce the burden of HAIs, accurate studies to characterize the microbiota of medical devices and to identify the main sources that lead to their contamination may be other important interventions to enhance the effectiveness of infection prevention and control practices. Therefore, different scholars performed studies to this end. Among them, Shoaei et al. were the only ones that, analyzing 19 samples from medical devices in hospital rooms of burned patients affected by Clostridium difficile, and did not find any positive contamination from Clostridium difficile (51). Opposite results were obtained by Pérez-Fernández et al. in their observational study on 19 physiotherapy and rehabilitation centers, in which the level of contamination on instruments and equipment used for patient therapies administration was investigated. They detected a greater presence of Enterobacteriaceae as well as Staphylococcus epidermidis in different devices. In addition to these bacteria, Pérez-Fernández et al. identified other important pathogens, such as Staphylococcus aureus, Acinetobacter spp, and Escherichia coli on the sponge electrode. In this study, sponge electrodes represented the instrumental samples with higher and more varied contamination, up to more than 20 different bacterial species, probably as the consequence of inadequate cleaning (53).
In addition to previous studies, Cruz-López et al. examined the colonization process and the possible transmission routes of HAI causative agents through the sampling of medical devices, such as mechanical ventilation tubes, central venous catheters, and urinary catheters. They collected samples from medical devices near to patients at different times, on day 1 of admission, day 3, and every 5 days until the patient's discharge. The same HAI pathogens identified in patients were also identified on medical devices and in particular mechanical ventilation tubes were the most colonized medical devices in those patients that developed VAP between day 1 and day 3 (54).
In their study, Mahjoub et al. worked analyzing the instrumentations of ophthalmology clinics to identify potential sources of pathogenic spread. The collection of the 33 samples was performed at 6 am before any patients or staff members entered the clinics and after the cleaning of the night before. More than half samples yielded bacterial growth, without significant differences among the clinics. Different pathogens were detected, first of all, Staphylococcus epidermidis, associated with post-intraocular surgical infection; followed by Staphylococcus capitis, implicated in surface infection such as purulent conjunctivitis; Micrococcus luteus, able to form biofilms implicated in prosthetic valve endocarditis; Corynebacterium species, causing granulomatous mastitis, and, moreover, Cutibacterium acnes, which is well-established as a cause of post-operative chronic endophthalmitis. Therefore, these findings defined medical devices as possible vectors for HAIs spreading indicating a need for increased disinfection of these instrumentations (69). Eventually, Swanson et al. performed a little different study with the aim to identify the main sources that lead to medical device contamination in addition to the characterization of the contamination itself. They used SourceTracker, a DNA sequence-based analytical tool, to identify the sources of contamination of nebulizer devices using the samples' microbiome as a biomarker. They performed source identification to look for four potential sources of microbial contamination: human gut microbiota, human oral microbiota, human skin microbiota, and hospital indoor environment microbiota. The latter was identified as the primary source of microbial contamination in nebulizers, contributing to ~41.3% of microbiomes with a variation ranging from 20.2% to 64.8%. On the contrary, the microbiota from human sources accounted only for ~10% of nebulizer microbiomes, with a higher prevalence referable to the human skin microbiota, followed, by human oral microbiota and human gut microbiota. However, their classification lacking some microbial sources since ~50% of the compounds were not classified as belonging to one of the 4 groups (70).
Based on all these studies, medical devices can represent a possible way for pathogen transmission and HAIs to spread mainly due to wrong cleaning procedures, therefore infection control practices should be developed and implemented to mitigate microbial contamination of medical devices whatever the source.
Environmental factors, ecosystem, and HAIsAt present, different factors can influence HAIs. From an environmental point of view, it is possible to go beyond the HE, analyzing different environmental factors which characterize our ecosystems, such as humidity, temperature, illuminance, season, and climate changes. The following studies focused on one or more of these factors, contributing to identifying their roles in spreading HAIs, in order to develop control procedures to manage and limit the risk to human health. One of the first studies was that of Ramos et al., which characterized the indoor environmental variations in which microbial samples were taken for the “Hospital Microbiome Project.” This project was designed to investigate microbial community and environmental factors inside 10 patients' rooms and two nearby nurse stations for a period of 1 year in a newly established hospital. Both surface-bound and airborne microbes were influenced by different environmental factors (temperature, relative humidity, and humidity ratio) in their growth or survival responses. Moreover, these Authors observed variation due to light conditions, in particular, because a high degree of sunlight illumination may inhibit bacterial growth or have bactericidal powers. They also observed further correlations with the entrance of the new occupancy and activity explained in the rooms, which may represent the main cause of contamination from human-related microbial communities (71). As well as the previous study, also Freedberg et al. highlighted, in their conclusions, that the microbial community in a healthcare setting may be altered by multiple environmental factors, such as seasonal shifts, solar exposure, and temperature (61). Another study focused on temporal variation is that of Schwab et al. which evaluated the implications of seasonal variations specifically on nosocomial bloodstream infections (BSIs). They performed a retrospective cohort study based on 2 databases (one for HAIs monitoring and one with aggregated monthly climate data) collecting information on about 1196 ICUs located in 779 hospitals and in 728 different postal codes in Germany. Collectively they analyzed more than 6.5 million ICU patients and more than 19000 BSIs in a 15-year period. Through their studies, Schwab et al. were able to determine that the incidence of BSIs was correlated with temperature and vapor pressure, and inversely with relative humidity. Related to temperature the incidence of BSI was 17% higher in months with temperature ≥20°C compared to months with temperature < 5°C. In particular, a strong correlation was observed when the mean monthly temperature of the month prior to the BSI occurrence was considered rather than the temperature of the month of occurrence. More in detail, the gram-negative bacteria were those with the most prominent effect despite the majority of bacteria increased with rising temperatures. Enterococci showed no seasonality while Staphylococcus pneumoniae reached a peak in wintertime. These conclusions agreed with previous studies which claimed that gram-negative BSI was most frequently in warmer months; gram-positive BSIs were inconsistent except for Staphylococcus pneumoniae BSIs which resulted most frequently in months with the lowest temperatures (72). A similar retrospective observational study, but on another type of HAIs, was that performed by Aghdassi et al., which included more than 2 million procedures resulting in ~32,000 surgical site infections (SSIs) from 1455 surgical departments. They matched the date of the procedures with the meteorological conditions for the month in which the procedure was performed. In accordance with the previous study also SSIs resulted most frequently in the months with temperature ≥20°C rather than in those with temperature < 5°C with a higher correlation for those SSIs due to gram-negative bacteria. This was particularly prominent for Acinetobacter spp and Enterobacter spp for which was shown that a rise of only 1°C led to an increase in SSIs incidence of 6% and 4%, respectively. Among gram-positive bacteria, Staphylococcus aureus showed a stronger association with warmer temperatures. However, despite one could think that a stronger correlation should be related to human skin bacteria (such as the latter), a higher correlation between temperature and pathogens was observed for those microorganisms abundant in the human gut (such as Acinetobacter spp, Enterobacter spp, Pseudomonas aeruginosa, Enterococcus spp, and Escherichia coli) thereby emphasizing the importance of human gut microbiome also in HAIs pathogenesis (73). More recently, Li et al. demonstrated a significant difference in the microbial composition in healthcare settings on a seasonal time scale. However, despite some HAI-related bacteria such as Acinetobacter, Pseudomonas, Enterococcus, Staphylococcus, and Escherichia existing throughout the year, they observed their increase in some periods of the year, for instance, Acinetobacter was highly abundant in June and December, whereas Pseudomonas in March, April, and May (15).
In addition, Sereira et al. showed also a specific correlation between months and bacteria amount. In particular, they noted a higher median amount of HAI-related pathogens in May and September, in some sampling sites, due to an increase in Escherichia coli and an outbreak of Acinetobacter baumannii, respectively (50). Wu et al. characterized bacterial dynamics among the seasons collecting 10 hospital ambient air particulate matter (PM2.5) samples in summer and 9 in winter. Differently from Proteobacteria, which remain consistent through the entire sampling period, they showed a decrease of 12% in Actinobacteria phylum from summer to winter, and an increase of Firmicutes phyla which passed from 22 to 40%. More generally, the microbiota results detected were less diverse in winter by one order of magnitude overall (74).
All these studies, taken together, indicate that meteorological factors impact microbiological composition and thus may influence the occurrence of different HAIs. Therefore, based on these considerations should be developed proper protocols to control HAI-related pathogens adjusted by months.
Studies of transmission/cleaning and HAIsScientific evidence shows that the application of appropriate cleaning procedures together with campaigns to raise awareness for hand hygiene may lead to reduce microbial contamination and HAIs spreading. Indeed, different scholars, such as Pérez-Fernández et al., concluded that the accumulation and proliferation of HAI-related pathogens might be due to the absence of adequate cleaning and maintenance procedures. In particular, they stated the importance of disinfection not only for HCW, but also for the entire HE including all instruments, equipment, and anything else that has come into contact with the patient (53).
We started considering three articles that tested bacterial transmission alone or in association with cleaning procedures. Del Campo et al. enrolled 30 healthy volunteers (20 women and 10 men) to perform a four-sequential steps protocol of finger-to-finger contact in the same person artificially infected with a precise bacterial inoculum. After the experimental procedure, the volunteers were grouped into three categories, based on their propensity to finger-to-finger bacteria transmission: women were classified in the medium category, whereas the men were divided into the poor or high categories. Analyzing specifically five different HAIs-related bacteria, they defined that gram-positive bacteria such as Enterococcus faecium and Staphylococcus aureus were characterized by a higher transmission efficiency in comparison to gram-negative bacteria. In particular, despite Escherichia coli results showing it to be a ubiquitous bacteria, it was characterized by a low transmission efficiency. Moreover, they performed a second experiment to test the inter-individual transmission chain exploring the finger-to-finger bacterial transmission with all possible combinations of individuals belonging to the three classes; from this test, they detected a reproducible transmission pattern whose efficiency was strictly dependent on the position of the poor transmitter, who cut off the transmission chain (75).
Weber et al. simulated the transmission of ESKAPE pathogens and Clostridium difficile under varying contact scenarios. They performed experiments for both direct (skin-to-skin) and indirect (skin-to-formite-to-skin) transmission by inoculating synthetic skin surrogates with a background skin microbiota or with both background skin microbiota and pathogens, simulating the transmission both before and after cleaning procedures. They observed
留言 (0)