
記住我









We conducted a prospective, single-centre, assessor-blinded, randomized, controlled superiority trial comparing non-operative treatment (n1 = 50) vs volar plating (n2 = 50) of unstable DRF in patients ≥ 65 years with regards to complications and functional outcome. The detailed study protocol has been published with open access [11]. The study was conducted from November 2019 to March 2022.
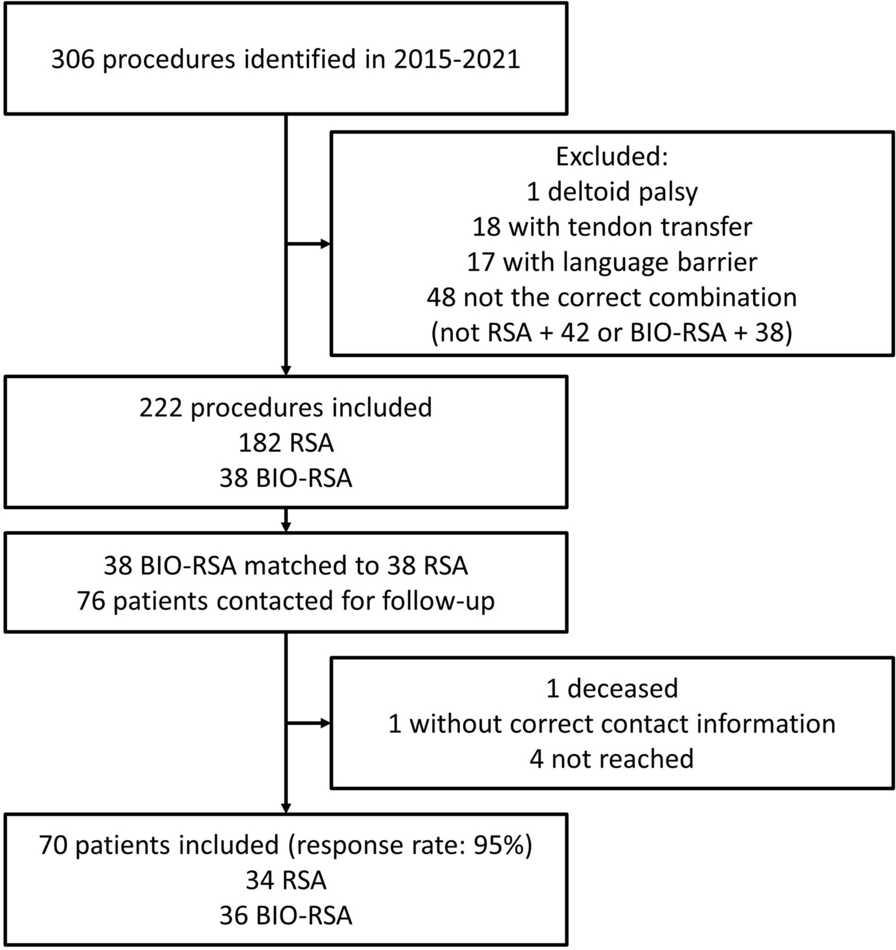
Interventions and randomizationAll patients with DRF diagnosed at our emergency department (ED) were screened for eligibility. Exclusion criteria were age < 65 years, high energy fracture, open fracture, concomitant injuries, previous fracture on the same arm, and inability to give written consent (Fig. 1).
Fig. 1
After diagnosing the DRF on standardized wrist radiographs (anterior–posterior and lateral projections) in the ED, the physician on call had two attempts to achieve an acceptable closed reduction under local analgesia with a 20 mg/ml lidocaine haematoma block. The radiological NCG criteria were assessed on new radiographs. According to the sample size calculation, 50 participants were allocated to each group; hence, 100 identical A5 envelopes were sealed, each containing a folded note whereupon either “operative” or “non-operative” were written. The concealment strategy was tested and light could not shine through the envelopes. Concealment of allocation was thus effective.
ORIF with volar plate fixation utilized Acu-Loc®, Acumed or Variax®, Stryker, depending on the surgeon’s preference. A standard Henry approach to the distal radius and pronator quadratus repair, if possible, was performed in the operative group. The vast majority of patients were operated under regional anaesthesia, and the remaining patients were operated under general anaesthesia.
After surgery, the wrist was immobilized in a dorsal plaster cast for 2 weeks, followed by a further 3 weeks of immobilization with a removable orthosis. A single hand therapeutic instruction took place.
Non-operative treatment consisted of a dorsal plaster cast immobilization for 5 weeks. Only discomfort, neurologic deficits or signs of infection warranted removal and replacement with another dorsal plaster cast. A single hand therapeutic instruction took place in this group after removal of the cast. No radiological evaluation was performed before 5 weeks after the injury.
OutcomesThe primary outcome was the complication rate after 12 months. Complications were prospectively recorded at day 0 (baseline), 2 weeks, 5 weeks, 6 months and 12 months after injury. The patient answered standardized questions from the investigators at the given timepoints.
Complications were defined as the presence of:
Sensory disturbance, including carpal tunnel syndrome and chronic regional pain syndrome
Flexor tendon rupture and irritation
Extensor tendon rupture and irritation
Hardware failure, e.g. osteosynthesis loosening
Infection: superficial (treated with antibiotics only) or deep (requiring surgical intervention)
Reoperation with hardware replacement
Reoperation with hardware removal (partial or total), which is not routinely performed in our country
Vascular compromise (capillary refill ≥ 2 s).
Secondary outcomes were obtained at the same timepoints as the primary outcomes.
Patient-reported outcome measures included the Danish version of the Quick Disabilities of the Arm, Shoulder and Hand (Quick-DASH), which was used to assess the level of functionality prior to injury and after 2 weeks, 5 weeks, 6 months and 12 months. The minimal clinically relevant difference was defined as a 16- to 20-point difference in Quick-DASH [12,13,14]. The pain experienced during activity within the preceding 14 days before the injury and at 2 weeks, 5 weeks, 6 and 12 months of follow-up was recorded using the 0–10 Numeric Rating Scale (NRS). A validated Danish version of the Patient-Rated Wrist/Hand Evaluation (PRWHE) was also applied [15].
Range of motion (ROM) was measured by a registered nurse using a goniometer. To ensure the observer was blinded, the patient was instructed not to talk about the treatment. Furthermore, all wrists were covered by a glove concealing potential scars.
The grip strengths of both left and right hand were estimated as the mean score of three repetitions of each hand, alternating hands between attempts, after 6 months and 12 months using a calibrated dynamometer (EH101 CAMRY, by the Camry scale). Quality of life was assessed with European Quality of Life 5 Dimensions 3 Levels (EQ-5D-3L).
Baseline demographics were reported as age, gender, side of DRF, dominant hand, working status, ASA class 1–6 (American Society of Anaesthesiologists Classification), smoking, alcohol consumption and diabetes.
Statistical methodsThe primary outcome, complication rate, was compared using Fisher’s exact test of the accumulated complication rate after 12 months. In order to prevent double counting, in patients with multiple complications, only one complication was accounted for in this calculation (bold numbers in Table 2).
All secondary outcome measures were analysed for all obtained data using mixed-effects analysis with Sidak’s multiple comparisons test. All available data were used without imputations for missing values.
According to our sample size calculation, 50 patients per treatment arm provide 80% statistical power at a 5% alpha level assuming a difference of 20% in complication rate between operatively and conservatively treated patients.
Statistical analyses were performed with Prism 9 for macOS.
The present trial was approved by the Danish Scientific Ethical Committee (ID: 1-10-72-420-17) and registered at Clinicaltrials.gov (ID: NCT03716661) [7].
留言 (0)