
記住我








After obtaining approval from the local ethics committee (blinded for review), a retrospective query of the institutional electronic database of a single academic tertiary revision arthroplasty and orthopedic oncology department was performed. The study was conducted in accordance with the World Medical Association’s Declaration of Helsinki.
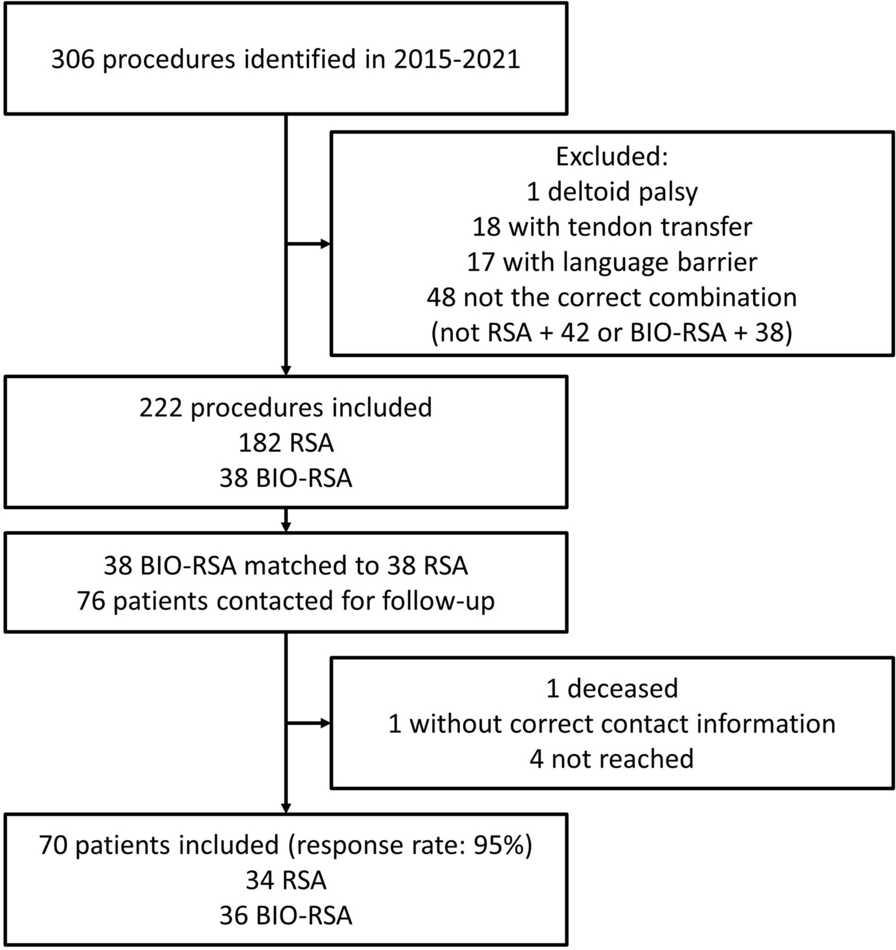
We retrieved all 212 cases of chronic knee PJI—diagnosed based on the 2011 Musculoskeletal Infection Society (MSIS) criteria—that underwent the first stage of an intended two-stage exchange between February 6, 2012 and December 12, 2020. We excluded four patients from our analysis who underwent amputation following first-stage surgery and six patients who died after the first stage (Fig. 1). Treatment success and failure were defined as recommended by the MSIS [24]. However, as the TTR was our independent variable, a completed second stage was a precondition for further analysis. Seven patients had a documented transition to another hospital and four patients were lost to follow-up, resulting in 191 cases. Also, 22 cases requiring at least one spacer exchange between the stages were excluded, as this event likely delays the TTR and is considered a risk factor for subsequent treatment failure. Three patients had PJI in both knees (six cases) and were therefore excluded from the analysis, as these cases are not independent. Finally, 163 patients who completed the second stage were included in the analysis.
Fig. 1
Flowchart of included and excluded cases of knee PJI
The electronic patient file was analyzed for patient characteristics, microbiology data and details on the initial surgery as well as potential revision surgeries. The patient’s age, Charlson Comorbidity Index (CCI) [25] and body mass index (BMI) were calculated. The CCI was chosen as a surrogate for host status because it can be well assessed retrospectively from medical records and significantly correlates with the risk of PJI [26, 27].
The diagnosis of infection was made based on the 2011 MSIS criteria [28], relying on culture results, fistula or visible foreign material, as well as synovial leukocyte count and serum C-reactive protein (CRP). In each revision surgery, a minimum of three to five tissue cultures were taken and incubated for a minimum of 7–14 days. All patients underwent a minimum of 6 weeks of combined intravenous and oral tailored antibiotics depending on the microbiological findings. We did not use suppressive antibiotics for planned two-stage revisions to achieve infection control.
A two-stage revision using antibiotic-impregnated polymethylmethacrylate (PMMA) spacers with intramedullary rods was the approach of choice for chronic knee PJI in all patients.
All spacers were handmade using intramedullary titanium rods (diameter: 6 mm) that were wrapped in PMMA to bridge the knee joint and any bone defect present. In our standard protocol, we used a commercially available bone cement (Copal G + C, Heraeus Medical) containing 1 g of clindamycin and 1 g of gentamicin. For every 40-g batch, an additional 2 g of vancomycin was incorporated in the presence of gram-positive organisms or unknown organisms. In instances involving resistant gram-negative microorganisms, we added 2–4 g of meropenem. For fungal infections, 600 mg of voriconazole or amphotericin B was added. For all patients, we recommended that they should not bear weight on the operated leg or, at most, apply light sole contact. Patients who were unable to follow the mobilization with crutches were provided with a wheelchair. We must acknowledge that, in our clinical experience, many patients do not adhere to these instructions, often resulting in larger bone defects due to excessive loading. All patients received a rigid knee brace for additional stabilization.
After completing the minimum of 6 weeks of systemic antibiotics, all patients were seen in the outpatient clinic and were scheduled for reimplantation if the knee joint exhibited no irritation and the laboratory infection parameters (serum CRP and leukocyte counts) were low. Knee joint aspiration was not performed at this stage. All second-stage reimplantation surgeries were performed using a single-design implant system (modular tumor and revision system, MUTARS, Implantcast GmbH, Buxtehude, Germany).
Description of outcomes: infection control, aseptic revisions, overall survivalInfection control was based on the consensus criteria from Diaz-Ledema, which require healed wounds, no further revision surgery for infection and no PJI-related mortality [29]. Reinfection-free survival was defined as the time from reimplantation (second stage) to the date of the first reinfection of the knee. Patients without reinfection were censored at their last follow-up. Death without prior reinfection was regarded as censored.
Aseptic revisions included all subsequent surgical procedures on the same knee joint that were not performed due to a reinfection. Aseptic-revision-free survival was defined as the time from second-stage revision to the date of aseptic revision. Patients without aseptic revision were censored at their last follow-up or death. Previous reinfections were not considered here.
Overall survival was defined as the time between second-stage revision and death or last follow-up.
Description of functional outcomesThe functional outcomes were assessed at the last available follow-up at our institution. The Oxford Knee Score (OKS) is a patient-reported outcome (PRO) with 12 questions on activities of daily living. It is considered a highly specific PRO to assess function and pain after TKA [30]. The OKS provides a single summed score which reflects the severity of problems that the respondent has with their knee, ranging from 0 (the worst possible) to 48 (the best outcome). Patients were asked to fill in the German version of the questionnaire on a regular basis during the waiting time for their regular follow-up appointment. These appointments are offered to patients 6 weeks after the second stage if partial weight-bearing has been indicated or after 3 months otherwise. Thereafter, at least annual appointments with a clinical and radiological check-up were scheduled in our outpatient department. In addition, the range of motion of the knee is documented with the neutral-zero method in the electronic patient chart.
Statistical analysisStatistical analyses were performed using R statistical software (version 4.2.1, R Foundation for Statistical Computing, Vienna, Austria) and GraphPad Prism (version 9.4.0 for macOS; GraphPad Software, San Diego, CA, USA). All p values and confidence limits were two-sided and intended to be exploratory, not confirmatory. Therefore, no adjustment for multiplicity was made. Exploratory two-sided p values ≤ 0.05 were considered statistically noticeable.
In descriptive analysis, continuous variables are reported as median (25% quantile–75% quantile, IQR). Absolute and relative frequencies are given for categorical variables. TTR groups were compared using Mann–Whitney U tests for continuous data and Fisher’s exact tests for categorical variables.
The optimal cutoff point for the TTR regarding the outcome ‘reinfection’ was identified using the maximally selected log-rank statistic as proposed by Hothorn and Lausen [31] and implemented in the R maxstat package [32].
Time-to-event outcomes were analyzed using log-rank tests and Cox proportional hazard regression models. Event-free rates (at 2 and 5 years) were reported as Kaplan–Meier estimates and pointwise 95% confidence intervals (CI) using log-log transformation. Univariable Cox regressions included either the TTR group or TTR (in days) as the only independent variable. In order to adjust for potential confounding factors, CCI and CRP (mg/dl) were included as additional covariates in the Cox regression. Results are reported as hazard ratios (HR) and corresponding 95% confidence intervals (CI). Median follow-up was estimated using the reverse Kaplan–Meier method.
留言 (0)