
記住我


KEY POINTS
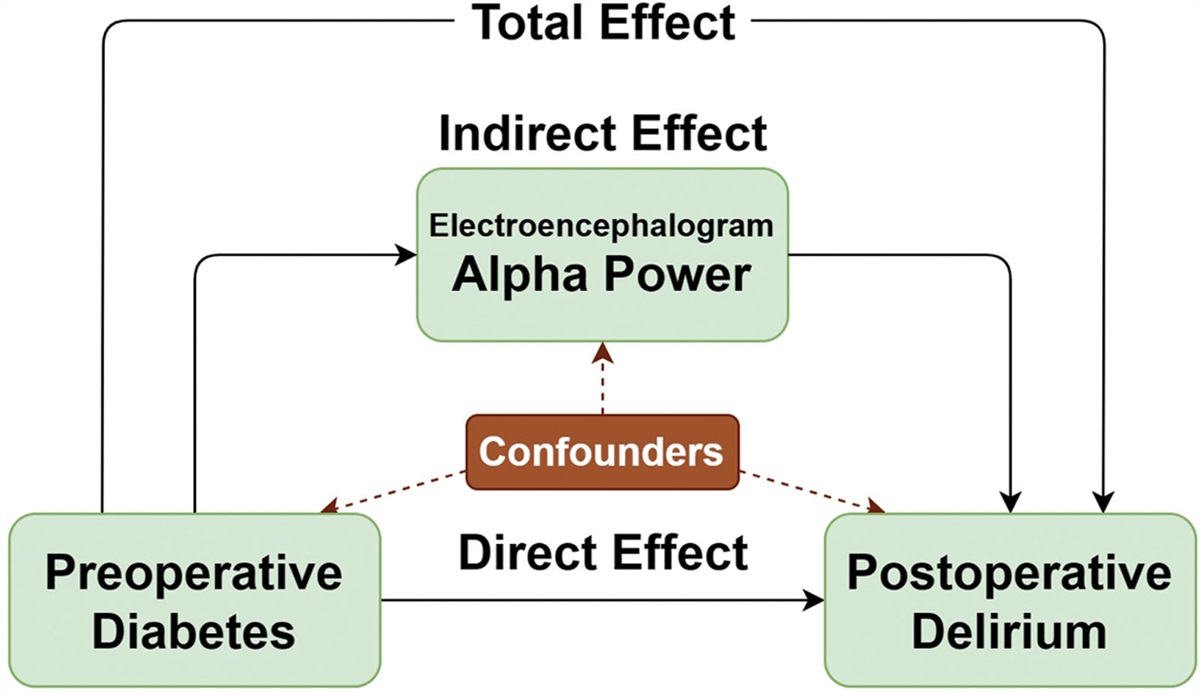
Question: Does the rate of maternal fever differ between women utilizing epidural versus continuous spinal labor analgesia? Findings: We found no evidence for a difference between the rate of maternal fever associated with epidural versus continuous spinal labor analgesia. Meaning: Our observation that the rate of maternal fever associated with neuraxial labor analgesia did not significantly differ between women receiving epidural versus continuous spinal analgesia suggests that a dose-dependent effect of bupivacaine or fentanyl is unlikely to mediate the association between maternal hyperthermia and neuraxial labor analgesia.See Article, page 1151
Neuraxial labor analgesia is associated with elevations in maternal temperature.1 This phenomenon is well described2 and lies in stark contrast to the hypothermia associated with neuraxial blockade for cesarean delivery3 or nonobstetric surgery.4 The mechanism responsible for the association between neuraxial labor analgesia and maternal hyperthermia is unknown, but is unlikely to be a result of infection.5,6 Epidural analgesia may alter maternal thermoregulatory pathways resulting in decreased ability to dissipate excess heat, either directly as a result of sympathetic blockade7,8 or indirectly through decreases in heat-dissipating activities such as hyperventilation9 that are common in the absence of effective labor analgesia. Inflammation may mediate epidural-related maternal fever,10,11 although the source of inflammation that drives the febrile response has not been identified. One hypothesis is that epidurally administered local anesthetics are systemically absorbed and trigger an inflammatory response during labor that results in maternal fever.1,12
Continuous spinal analgesia is an alternative to epidural labor analgesia.13 Continuous spinal analgesia is commonly utilized after accidental dural puncture with an epidural needle during attempted epidural catheter placement and is occasionally chosen for patients with significant comorbidities, such as cardiac disease or morbid obesity.14 Continuous spinal analgesia is titrated to achieve a similar degree of neuraxial blockade as epidural analgesia, but requires significantly less local anesthetic. This creates the conditions for a natural experiment on the effects of bupivacaine on maternal fever: if systemic effects of local anesthetics cause maternal fever, the drastically lower neuraxial and systemic bupivacaine levels associated with continuous spinal analgesia should result in a decreased rate of maternal fever. In contrast, if thermoregulatory effects of the neuraxial block are responsible for the association between maternal temperature elevation and epidural analgesia, we would predict a similar rate of fever in association with epidural and spinal labor analgesia.
Our single-center study was designed to test the hypothesis that continuous spinal labor analgesia is associated with a lower rate of maternal fever than epidural labor analgesia. Our retrospective study design was predicated on comparing an infrequently used technique, continuous spinal analgesia, with the commonly used technique of epidural labor analgesia to gain additional insights into the mechanism underlying the observation that maternal fever is associated with epidural labor analgesia; it was not designed to motivate changes in labor analgesia practice. Our predefined primary outcome was the rate of maternal fever, which we defined as a temperature ≥38 °C.
METHODSThe University of Chicago institutional review board approved this study and waived the requirement for informed consent. We used an institutional obstetric anesthesia quality database to identify patients who received continuous spinal labor analgesia between June 2012 and March 2020. We used a reverse chronologic search strategy beginning with patients who delivered in March of 2020. We excluded patients with no temperature measurements between the start of anesthetic care and delivery, patients with more than 1 type of neuraxial catheter (eg, a patient with an epidural catheter that was replaced with an intrathecal catheter), patients admitted with an intrauterine fetal demise, and patients who were febrile before the start of anesthesia care. Each patient receiving continuous spinal analgesia was matched to the 2 patients with the nearest anesthesia start time and the same nulliparous status receiving epidural analgesia who met inclusion criteria.
From the electronic medical record, we collected data on gestational age, body mass index (BMI) on delivery admission, group B Streptococcus (GBS) status, induction versus spontaneous labor, mode of delivery, number of cervical examinations in labor, diagnosis of chorioamnionitis, intrapartum administration of magnesium or antibiotics for chorioamnionitis or GBS, use of prostaglandins for induction of labor, admission to delivery and rupture of membranes (ROM) to delivery times, analgesic duration, and local anesthetic dose excluding patient-controlled boluses. The basal local anesthetic dose was calculated based on the rate and time for which the solution was running, as recorded in the anesthetic record. For patients receiving programmed intermittent epidural boluses, this represents an approximation of their total dose, as the timing of intermittent boluses was not captured in the medical record. Patient-controlled boluses were not captured on the anesthetic record and thus are not reported.
During the study time period, continuous spinal labor analgesia was typically initiated with 1.25 mg of bupivacaine and 4 to 15 µg of fentanyl, and maintained with a continuous infusion of 0.0625% bupivacaine with 2 µg/mL fentanyl at 2 mL/h. Patient-controlled boluses of 1 mL of the maintenance solution every 30 minutes were permitted by some but not all attending anesthesiologists. The infusion rate could be increased by 1 to 2 mL/h for patients with inadequate analgesia.
Combined spinal epidural procedures, dural puncture epidural procedures, and epidural procedures without dural puncture were all utilized during the study time period. Between the start of the study period (2012) and November of 2015, labor epidural analgesia was maintained with a continuous infusion of 0.0625% bupivacaine with 2 µg/mL of fentanyl with patient-controlled boluses of 5 mL of the maintenance solution allowed every 10 minutes, and an hourly maximum of 30 mL. In November of 2015, our institution transitioned to programmed intermittent bolus administration, and analgesia was maintained with 10-mL boluses of 0.0625% bupivacaine with 2 µg/mL of fentanyl every 60 minutes with patient-controlled boluses of 5 mL allowed every 10 minutes and an hourly maximum of 30 mL. Additional details regarding initiation of labor analgesia are described in the Supplemental Digital Content 1, https://links.lww.com/AA/D818.
Our protocol on labor and delivery calls for measurement of maternal temperature every 4 hours for patients in labor and every 2 hours after ROM. Maternal temperature during the study time period was typically measured with noncontact infrared thermometers, although oral thermometers were also available and occasionally used. We did not attempt to measure compliance with institutional protocols as part of this retrospective study. The temperature of labor rooms was not measured and patients had the ability to increase or decrease their individual room temperature according to their preferences.
Statistical AnalysisStatistical analysis was performed using JMP Pro (SAS Software). The primary outcome was intrapartum maternal fever, defined as any temperature of ≥38 °C before delivery. We hypothesized that the rate of maternal fever would be lower in women receiving spinal analgesia compared to those receiving epidural analgesia. The rate of maternal fever between women with epidural and spinal labor analgesia was compared using Fisher exact test and is reported as the percentage of women developing a fever within each group as well as the difference between these 2 groups. Continuous variables (BMI, gestational age, number of vaginal exams, admission-delivery, ROM-delivery, and anesthesia start-delivery times) were tested for normality using the Shapiro-Wilk test. Categorical data (nulliparity, GBS status, mode of delivery, diagnoses of preeclampsia or chorioamnionitis, intrapartum administration of magnesium, antibiotics, or prostaglandins) were compared using the Fisher exact test. Continuous data that did not conform to a normal distribution (BMI, gestational age in weeks, number of vaginal exams, admission-delivery, ROM-delivery, and anesthesia start-delivery times) were compared using the Kruskal-Wallis test. A multivariable logistic regression model was constructed to test the association between maternal fever and continuous spinal versus epidural labor analgesia. The model was adjusted for mode of delivery and anesthetic duration as potential confounders, and is presented with odds ratios and 95% confidence intervals (CIs). A P value of <.05 was considered significantly different.
We originally estimated that we would identify 150 women with continuous spinal labor analgesia and planned to match them to 300 control women with epidural labor analgesia. Based on an anticipated rate of fever of 5% in women with continuous spinal analgesia and 15% in women with labor epidural analgesia, this would have given us >90% power to detect a difference between these groups with a type I error rate of 5%. These estimates were based on a fever rate in women with continuous spinal analgesia at the upper end of that reported for women without neuraxial analgesia and an approximate midpoint of the reported incidence15–18 of fever for women with epidural analgesia.
However, we identified only 81 women with continuous spinal analgesia meeting our study inclusion criteria during the study time frame and extending the time frame would be impractical because our anesthetic records were first included in the electronic medical record in 2012. Therefore, we elected to continue with the study using the available records as a convenience sample. We made this decision before analyzing data on any women with epidural labor analgesia.
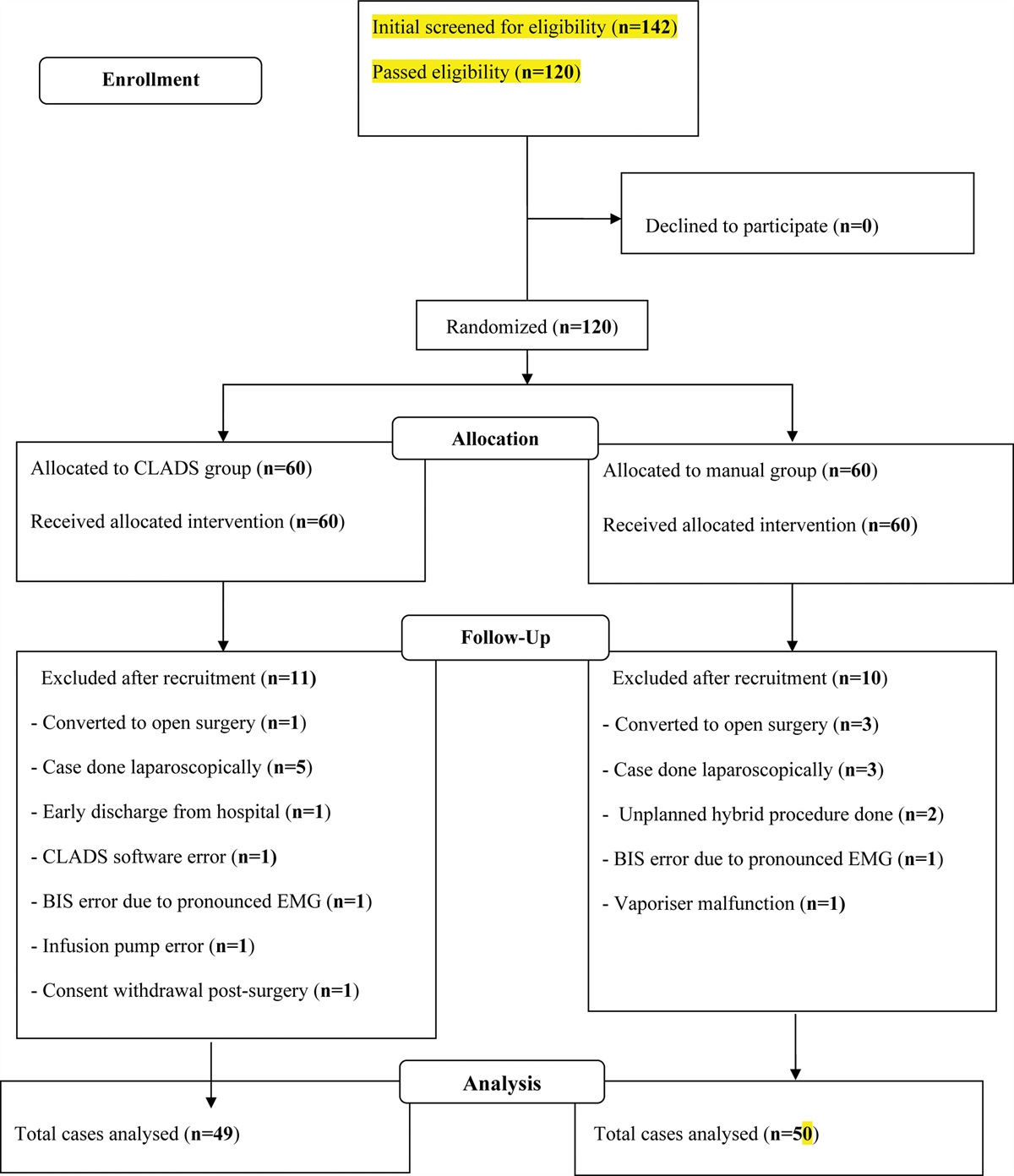
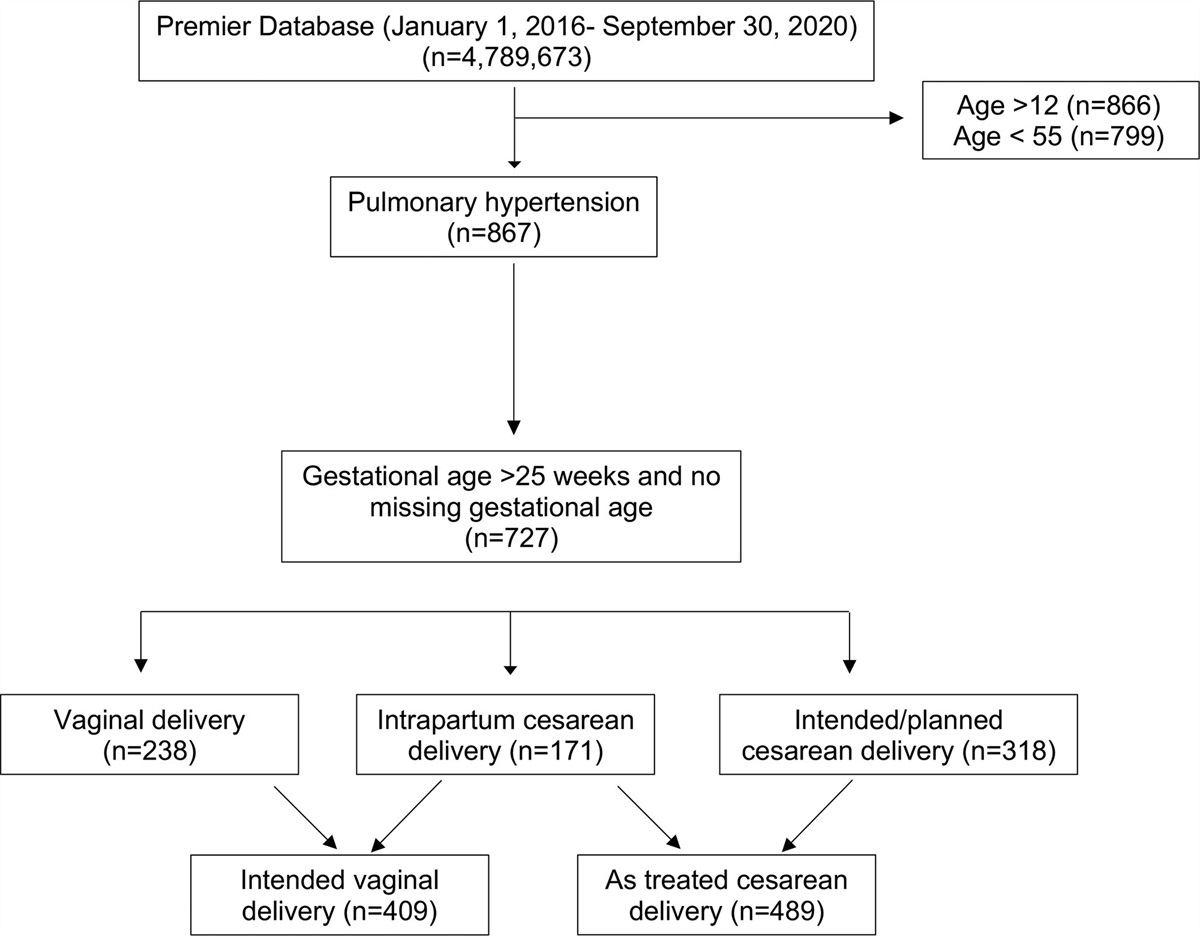
RESULTSOur obstetric quality database included 11,955 labor analgesic records during the study time period. After excluding patients without a temperature recorded after initiation of labor analgesia, those with an intrauterine fetal demise, and with multiple catheter types (eg, an epidural catheter that was replaced with a spinal catheter), we included 81 women with continuous spinal analgesia and 162 women matched for nulliparity in our study cohort (Figure).
 Figure.:
Figure.: Study flow diagram. *One patient with an intrauterine fetal demise also had a temperature ≥38 °C before intrathecal catheter placement and is included in the counts for both exclusion criteria.
Demographic characteristics are described in Table 1. Women receiving continuous spinal analgesia had a slightly higher BMI than those receiving epidural analgesia. Labor descriptions and outcomes are described in Table 2 and did not differ significantly between groups. The duration of labor analgesia did not significantly differ between groups, but bupivacaine utilization (exclusive of patient-controlled boluses) was significantly higher in women receiving epidural labor analgesia (Table 3).
Table 1. - Patient Demographics Spinal analgesia (n = 81) Epidural analgesia (n = 162) P value Nulliparous 35 (43%) 70 (43%) N/A Body mass index (kg/m2) 33 (28.25–52.5) 32 (27–36) .04 Gestational age (completed weeks) 39 (37.5–40) 39 (38–40) .12Data are presented as n (%) or median (interquartile range). Comparisons between groups were performed using the Kruskal-Wallis test.
Abbreviation: N/A, not applicable.
Data are presented as n (%) or median (interquartile range). Comparisons between groups were performed using the Fisher exact or Kruskal-Wallis test.
Abbreviations: C/S, cesarean delivery; GBS, group B Streptococcus; NSVD, normal spontaneous vaginal delivery; OVD, operative vaginal delivery (forceps or vacuum assisted).
aTwo patients who received epidural analgesia did not have the time of membrane rupture recorded.
Data are presented as median (interquartile range). Comparisons were performed using Kruskal-Wallis test. Bupivacaine consumption does not include patient-controlled boluses.
Eight of 81 (9.9%; 95% CI, 5.1–18.3) women with continuous spinal analgesia developed an intrapartum fever compared to 18 of 162 (11.1%; 95% CI, 7.1–16.9) women with epidural analgesia (P = .83). The mean difference between the proportion of women with fever in the spinal relative to the epidural analgesia group was −1.2% (95% CI, −9.0 to 7.5; a negative value indicates a decreased proportion of febrile women in the spinal analgesia group). In logistic regression analysis, the rate of maternal fever was not associated with route of labor analgesia after adjusting for a potential influence of mode of delivery or anesthesia start-delivery time as potential confounders (Supplemental Digital Content 1, Table 1, https://links.lww.com/AA/D818).
DISCUSSIONThere was no difference in the rate of maternal fever between women with continuous spinal compared to epidural labor analgesia in our study cohort. While the incidence of maternal fever has not previously been compared between women with continuous spinal and epidural labor analgesia, the incidence of maternal fever in our study is similar to the 14.1% rate reported in an observational study of spinal analgesia provided with 23-gauge intrathecal catheters,19 and to fever rates in patients with epidural catheters.20 Our study is unique in that we were able to directly compare the rate of maternal fever between women receiving spinal and epidural labor analgesia.
Our findings have implications for the association between maternal hyperthermia and neuraxial labor analgesia. There was a difference in bupivacaine consumption between women with continuous spinal versus epidural labor analgesia (despite our inability to capture patient-controlled boluses), but no difference in the rate of maternal fever. Our results are therefore not consistent with models in which a dose-dependent inflammatory effect of bupivacaine is responsible for maternal fever. While in vitro leukocyte studies investigating the effects of bupivacaine on inflammatory mediators have demonstrated altered cytokine profiles (specifically decreased levels of intracellular interleukin-1 receptor antagonist) with bupivacaine treatment, the concentration of bupivacaine used was 3 to 8 times higher than plasma bupivacaine concentrations in women receiving labor epidural infusions of 0.25% bupivacaine21 and thus markedly higher than would be achieved in vivo using modern low-dose infusion regimens.
While the route of administration and dose of bupivacaine differ between epidural and spinal labor analgesia, they are titrated to produce similar levels of neuraxial blockade. Our results thus support models in which effects of the central neuraxial blockade itself, such as alterations in thermoregulatory pathways7,8,22 link maternal fever and neuraxial analgesia. Potential thermoregulatory pathways impacted by effective neuraxial analgesia include a decrease in heat-dissipating behavioral activity (such as hyperventilation9) as well as direct effects of sympathetic blockade on sweating, vasodilation, and heat distribution.7,8 Our study does not distinguish between these possible mechanisms, nor does it rule out an effect of the catheter itself or a concentration-independent direct effect of bupivacaine on maternal fever.
Neuraxial labor analgesia is provided using a combination of local anesthetic and opioids. While we did not quantitate fentanyl consumption in this study, women receiving continuous spinal labor analgesia received a reduced dosage of neuraxial fentanyl relative to women receiving epidural labor analgesia. Opioids have been postulated to have an antipyretic effect,23 although this has never been demonstrated in the context of intrapartum hyperthermia. Neither the use of epidural opioids for labor analgesia nor use of parenteral opioids before initiating neuraxial labor analgesia influences the rate of maternal fever.24–26 As such, we believe that it is unlikely that differences in opioid consumption between groups in our study influenced the rate of maternal fever.
Our study must be interpreted in light of its limitations. Our sample size was smaller than we originally planned, and our study was thus underpowered based on our originally hypothesized rate of maternal fever of 5% for women with continuous spinal analgesia and 15% for women with epidural analgesia. Given that it was logistically not possible to retrospectively extend our sample size and that prospectively extending our study to achieve the planned sample size would require an additional 6 to 7 years of data, we elected to proceed with our analysis using the available data as a convenience sample. Furthermore, we relied on standard nursing documentation of maternal temperature, and we were unable to standardize either the times or site at which maternal temperature was measured. Our epidural analgesia group included women with epidural catheters placed without dural puncture as well as combined spinal epidural and dural puncture epidural techniques. Our study was not designed to investigate any potential differences in maternal fever that may be associated with variations in epidural technique. However, previous studies have not found differences in maternal temperature associated with a combined spinal epidural compared to epidural technique27 and maternal hyperthermia has consistently been reported regardless of variations in epidural technique.2 Our labor epidural protocol changed during the study period from a continuous infusion to programmed intermittent boluses. While previous studies have not found differences in the overall rate of maternal fever between intermittent boluses and continuous epidural labor analgesia,28 we cannot rule out an effect of this protocol change on the incidence of fever in our epidural analgesia group. While women were not randomized to continuous spinal versus epidural analgesia, most intrathecal labor catheters at our institution are placed after inadvertent dural puncture during attempted epidural catheter placement. Many obstetric and demographic variables may influence the rate of maternal fever; as our study was retrospective and included only a small number of febrile women, we were unable to rigorously control for all potential confounders. Given that continuous spinal labor analgesia is uncommon and that a randomized trial of continuous spinal analgesia using macrocatheters is not feasible because of the side effects associated with spinal macrocatheters (most notably post dural puncture headache14), our study provides valuable information despite these limitations.
A meta-analysis including more than 600,000 subjects from 41 studies has firmly established that epidural labor analgesia is associated with intrapartum hyperthermia.2 The mechanism underlying this association remains elusive. Identifying this mechanism will be essential to efforts to identify women at risk for epidural-related maternal fever, potentially modify risk factors to prevent its occurrence, and distinguish epidural-related maternal fever from fever related to infection. Our results, while subject to the limitations discussed earlier, demonstrate that maternal fever occurs in association with continuous spinal labor analgesia and that mechanisms linking neuraxial labor analgesia and maternal hyperthermia should apply equally to epidural and spinal labor analgesia.
DISCLOSURESName: F. Arran Seiler, MD.
Contribution: This author helped perform data extraction, analyze and interpret study results, and write the manuscript.
Name: Barbara M. Scavone, MD.
Contribution: This author helped design the study, interpret study results, and write the manuscript.
Name: Sajid Shahul, MD.
Contribution: This author helped analyze and interpret study results.
Name: David E. Arnolds, MD, PhD.
Contribution: This author helped design the study, perform data extraction, analyze and interpret study results, and write the manuscript.
This manuscript was handled by: Jill M. Mhyre, MD.
REFERENCES 1. Sultan P, David AL, Fernando R, Ackland GL. Inflammation and epidural-related maternal fever: proposed mechanisms. Anesth Analg. 2016;122:1546–1553. 2. Morton S, Kua J, Mullington CJ. Epidural analgesia, intrapartum hyperthermia, and neonatal brain injury: a systematic review and meta-analysis. Br J Anaesth. 2021;126:500–515. 3. du Toit L, van Dyk D, Hofmeyr R, Lombard CJ, Dyer RA. Core temperature monitoring in obstetric spinal anesthesia using an ingestible telemetric sensor. Anesth Analg. 2018;126:190–195. 4. Sessler DI. Perioperative thermoregulation and heat balance. Lancet. 2016;387:2655–2664. 5. Sharma SK, Rogers BB, Alexander JM, McIntire DD, Leveno KJ. A randomized trial of the effects of antibiotic prophylaxis on epidural-related fever in labor. Anesth Analg. 2014;118:604–610. 6. Riley LE, Celi AC, Onderdonk AB, et al. Association of epidural-related fever and noninfectious inflammation in term labor. Obstet Gynecol. 2011;117:588–595. 7. Mullington CJ, Low DA, Strutton PH, Malhotra S. Body temperature, cutaneous heat loss and skin blood flow during epidural anaesthesia for emergency caesarean section. Anaesthesia. 2018;73:1500–1506. 8. Glosten B, Savage M, Rooke GA, Brengelmann GL. Epidural anesthesia and the thermoregulatory responses to hyperthermia–preliminary observations in volunteer subjects. Acta Anaesthesiol Scand. 1998;42:442–446. 9. Hägerdal M, Morgan CW, Sumner AE, Gutsche BB. Minute ventilation and oxygen consumption during labor with epidural analgesia. Anesthesiology. 1983;59:425–427. 10. Segal S. Labor epidural analgesia and maternal fever. Anesth Analg. 2010;111:1467–1475. 11. Goetzl L, Zighelboim I, Badell M, et al. Maternal corticosteroids to prevent intrauterine exposure to hyperthermia and inflammation: a randomized, double-blind, placebo-controlled trial. Am J Obstet Gynecol. 2006;195:1031–1037. 12. Del Arroyo AG, Sanchez J, Patel S, ; EPIFEVER Investigators. Role of leucocyte caspase-1 activity in epidural-related maternal fever: a single-centre, observational, mechanistic cohort study. Br J Anaesth. 2019;122:92–102. 13. Veličković I, Pujic B, Baysinger CW, Baysinger CL. Continuous spinal anesthesia for obstetric anesthesia and analgesia. Front Med (Lausanne). 2017;4:133. 14. Cohn J, Moaveni D, Sznol J, Ranasinghe J. Complications of 761 short-term intrathecal macrocatheters in obstetric patients: a retrospective review of cases over a 12-year period. Int J Obstet Anesth. 2016;25:30–36. 15. Philip J, Alexander JM, Sharma SK, Leveno KJ, McIntire DD, Wiley J. Epidural analgesia during labor and maternal fever. Anesthesiology. 1999;90:1271–1275. 16. Yancey MK, Zhang J, Schwarz J, Dietrich CS III, Klebanoff M. Labor epidural analgesia and intrapartum maternal hyperthermia. Obstet Gynecol. 2001;98:763–770. 17. Goetzl L, Cohen A, Frigoletto F Jr, Lang JM, Lieberman E. Maternal epidural analgesia and rates of maternal antibiotic treatment in a low-risk nulliparous population. J Perinatol. 2003;23:457–461. 18. Lange EMS, Segal S, Pancaro C, et al. Association between intrapartum magnesium administration and the incidence of maternal fever: a retrospective cross-sectional study. Anesthesiology. 2017;127:942–952. 19. Tao W, Grant EN, Craig MG, McIntire DD, Leveno KJ. Continuous spinal analgesia for labor and delivery: an observational study with a 23-gauge spinal catheter. Anesth Analg. 2015;121:1290–1294. 20. Sharpe EE, Arendt KW. Epidural labor analgesia and maternal fever. Clin Obstet Gynecol. 2017;60:365–374. 21. Irestedt L, Ekblom A, Olofsson C, Dahlström AC, Emanuelsson BM. Pharmacokinetics and clinical effect during continuous epidural infusion with ropivacaine 2.5 mg/ml or bupivacaine 2.5 mg/ml for labour pain relief. Acta Anaesthesiol Scand. 1998;42:890–896. 22. Evron S, Ezri T, Protianov M, et al. The effects of remifentanil or acetaminophen with epidural ropivacaine on body temperature during labor. J Anesth. 2008;22:105–111. 23. Negishi C, Lenhardt R, Ozaki M, et al. Opioids inhibit febrile responses in humans, whereas epidural analgesia does not: an explanation for hyperthermia during epidural analgesia. Anesthesiology. 2001;94:218–222. 24. Gross JB, Cohen AP, Lang JM, Frigoletto FD, Lieberman ES. Differences in systemic opioid use do not explain increased fever incidence in parturients receiving epidural analgesia. Anesthesiology. 2002;97:157–161. 25. Douma MR, Stienstra R, Middeldorp JM, Arbous MS, Dahan A. Differences in maternal temperature during labour with remifentanil patient-controlled analgesia or epidural analgesia: a randomised controlled trial. Int J Obstet Anesth. 2015;24:313–322. 26. Camann WR, Hortvet LA, Hughes N, Bader AM, Datta S. Maternal temperature regulation during extradural analgesia for labour. Br J Anaesth. 1991;67:565–568. 27. Wong CA, Scavone BM, Peaceman AM, et al. The risk of cesarean delivery with neuraxial analgesia given early versus late in labor. N Engl J Med. 2005;352:655–665. 28. Mantha VR, Vallejo MC, Ramesh V, Phelps AL, Ramanathan S. The incidence of maternal fever during labor is less with intermittent than with continuous epidural analgesia: a randomized controlled trial. Int J Obstet Anesth. 2008;17:123–129.
留言 (0)