

記住我
The vertebral arteries (VAs) originate from the subclavian artery, and the two VAs converge to form the BA at the lower margin of the junction of the medulla oblongata and the pons. The diameters of both VAs are generally asymmetrical. Vertebral artery dominance (VAD) is an extremely common variation of VAs. Although without a standard definition, VAD refers to the obvious asymmetry of the vertebral artery diameters on both sides (1). In most conditions, if a VA union occurs, the non-dominant VA is likely to obtain sufficient blood supply from the dominant one. Thus, traditionally VADs have traditionally been regarded as a normal congenital vascular variant of VAs. In recent years, evidence has been raised that VAD is an independent risk factor for posterior circulation ischemic stroke (1–4).
The posterior inferior cerebellar artery (PICA) is a principal branch of the VA and has no alternative collateral circulation (5). One less common variation of VA is that a hypoplastic VA does not unite with the contralateral VA but ends into the PICA. This type of variation is termed a vertebral artery terminated in PICA (PICA-VA) (6–8). It was also referred to as “basilarization” one of the ICVA by Caplan (9).
Although the existence of PICA-VA is known, relatively little information has been revealed from clinical studies regarding its prevalence and relationship to vertebrobasilar stroke. One previous duplex sonography and magnetic resonance angiography (MRA) based study that included 80 patients and 80 controls suggested that the prevalence of PICA-VA was much higher (18.7 vs. 6.3%) in patients with a history of vertebrobasilar stroke or transient ischemic attack (TIA) than that in the matched normal controls (7). More recently, MRA screening for evidence of stroke before cervical spine surgery demonstrated that PICA-VA was more frequent in patients aged older than 50 years than those younger than 39 years (13.3 vs. 1.6%) (10).
The detection of PICA-VA relies on the development of cerebrovascular imaging modalities, samples, and subject heterogeneity. Digital subtraction angiography (DSA) is supposed to be a more precise technique to identify PICA-VA. Osborn et al. found that about 0.1% of patients had the variation by DSA (11). However, numerous patients did not receive invasive DSA, and this might have led to an underestimation of the prevalence of PICA-VA. Non-invasive methods like magnetic resonance angiography (MRA) have been used to evaluate the cerebral artery. In a small cohort, ~1 in ten patients (11.7%, 15/128) had PICA-VA (6).
In the present study, we aimed to investigate the prevalence of PICA-VA in a multicenter hospital-based cross-sectional study with a larger sample size and explore the relationship between PICA-VA and vertebrobasilar stroke.
Methods PopulationA retrospective review of a prospectively complied multicenter hospital-based computerized database was performed (12). The study was approved by the local institutional ethics committee. Informed consent was signed by the patient or an authorized person.
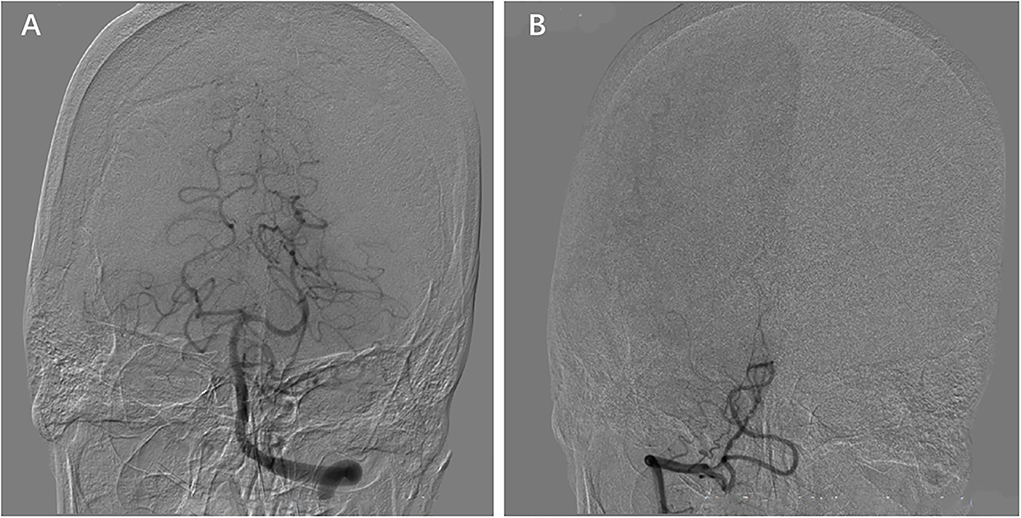
Experimental designFrom 1 August 2015 to 31 May 2017, patients from Jinling Hospital, The Second Affiliated Hospital of Guangzhou Medical University, The First Affiliated Hospital of Soochow University, and Wuxi People's Hospital were screened. The patient who met the following criteria was included in the present study: (1) More than 18 years old. (2) Stroke was defined by brain magnetic resonance imaging (MRI), and acute neurological deficits evaluated by neurologists were required; (3) Cerebral MRI including T1, T2, and DWI images and MRA were performed within 1 week of stroke onset; (4) Intracranial VA and PICA were clearly visible; (5) Cervical carotid artery and vertebral artery were detected by ultrasound, CTA, MRA, or DSA. PICA-VA was confirmed by the DSA; and (6) Clinical information was available. The patient who had one of the following criteria was excluded from the analysis: (1) Occlusion of vertebral artery or basilar artery; patients were also included in the analysis when occluded vessels were recanalized. (2) Unique vertebral artery. (3) Hemorrhagic stroke. The hemorrhagic transformation within an ischemic infarction was also included in the analysis. (4) Spinal infarction. (5) Infarction distributed both in the anterior and posterior circulation areas. PICA-VA was defined as VA not communicating with the basilar artery but ending into the ipsilateral PICA according to MRA and verified by DSA (Figure 1).
Figure 1. Posterior inferior cerebellar artery (PICA) termination of the vertebral artery (PICA-VA). The VA on one side does not join the contralateral VA (B), instead terminating as the posterior inferior cerebellar artery (A).
Digital subtraction angiography imaging analysisDigital Subtraction Angiography was performed with femoral catheterization by using the Seldinger technique with a biplane DSA unit with rotational capabilities (Axiom Artis dTA; Siemens Healthcare). Typically, 6–9 ml of non-ionic contrast medium (iopromide, 300 mg of iodine per milliliter, Ultravist 300; Bayer Schering) was used per acquisition, usually consisting of one anteroposterior, one lateral, and one or two oblique views. With the catheter in each of the three major arteries (both internal carotid arteries and one or more vertebral arteries), standard anteroposterior, lateral, and oblique DSA images were obtained.
Data collectionTrained interviewers conducted face-to-face interviews at the hospital to collect data at baseline. On admission, demographic information (including age and gender), risk factors for stroke [including body mass index (BMI), current smoking, hypertension, diabetes, previous stroke or transient ischemic attack (TIA) or intracranial hemorrhage (ICH), previous coronary artery disease (CHD), and atrial fibrillation], and laboratory examinations [including total cholesterol, TG, HDL cholesterol, LDL cholesterol, Glomerular Filtration Rate (GFR)], and current medications (including antihypertensive agents, lipid-lowering agents, antiplatelet agents, and anticoagulant agents) on admission were acquired. Current drinking was defined as heavy intake (≥14 drinks/week in women or 21 drinks/week in men) or episodic heavy intake (≥5 drinks/episode at least once per month) (13). Diabetes was defined as A1C ≥6.5%, FBG levels ≥7.0 mmol/L, blood glucose ≥11.1 mmol/L at 2 h by oral glucose tolerance test (OGTT), blood glucose ≥11.1 mmol/L at random glucose test, any use of glucose-lowing drugs, or any self-reported history of diabetes (14). Hypertension was defined as systolic pressure ≥140 mmHg or diastolic pressure ≥90 mmHg, any use of antihypertensive drugs, or a self-reported history of hypertension (15).
Statistical analysisStatistical analysis was performed using SPSS for Windows, version 22.0 (SPSS Inc., Chicago, IL). All parametric results are expressed as mean ± SD or percentage (for discrete variables). The Chi-square test was used for the comparison of categorical variables, and all the baseline variables were included in the logistic regression multivariable model. Two-sided p < 0.05 was considered significant. To adjust for confounding factors with p < 0.10, multivariable logistic regression analysis was used to assess any independent factors of vertebrobasilar stroke.
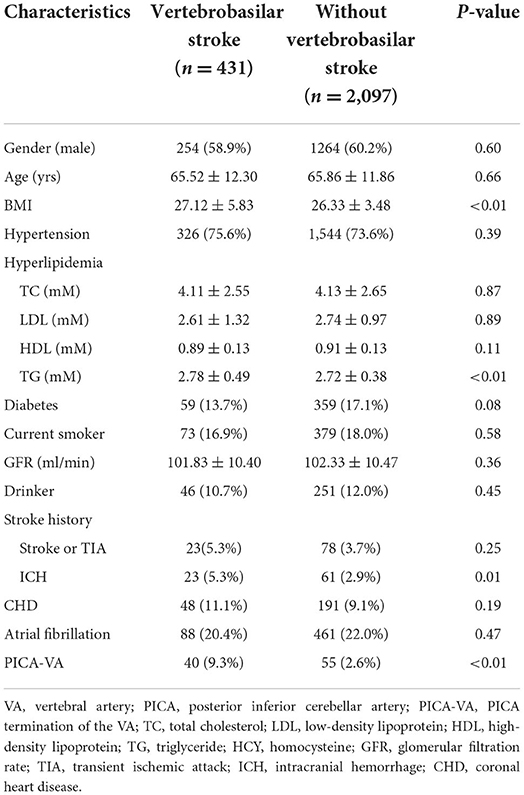
Results Incidence of PICA-VA in vertebrobasilar strokeFrom 1 August 2015 to 31 May 2017, a total of 2,528 patients were enrolled in the present study. The patient demographics are presented in Table 1. In 431 of the 2,528 patients, infarcts were identified in the territory of the posterior circulation, including the brain stem, cerebellum, occipital cortex, temporal cortex, and thalamus. Ninety-five (3.76%, 95/2,528) patients had the variation of PICA-VA, 51 of which (53.7%, 51/95) were located on the right side. Patients with PICA-VA presented a higher incidence of vertebrobasilar stroke (42.1, vs. 16.1%, p < 0.01) and a higher incidence of contralateral intracranial VA stenosis (33.7 vs. 17.5%, p < 0.01). Patients with PICA-VA demonstrated a different pattern of infarction distribution relative to those without PICA-CA. Infarction of patients with PICA-VA was most frequently located in the cerebellum (45.0%), followed by the pontine (30.0%) and medulla (10.0%). For patients without PICA-VA, the top 3 locations were pontine (44.2%), cerebellum (33.5%), and midbrain (11.0%).
Table 1. Characteristics of stroke patients with or without PICA-VA.
PICA-VA increased risk of vertebrobasilar strokeAs shown in Table 2, compared with those without vertebrobasilar stroke, patients with vertebrobasilar stroke presented a higher incidence of PICA-VA (9.3 vs. 2.6%, p < 0.01) as well as higher body mass index (BMI, 27.12 ± 5.83 vs. 26.33 ± 3.48, p < 0.01), higher level of triglyceride (2.78 ± 0.49 mmol/L vs. 2.72 ± 0.38 mmol/L, p < 0.01), and higher rate of intracranial hemorrhage history (5.3 vs. 2.9%, p = 0.01).
Table 2. Characteristics of stroke patients with or without posterior circulation stroke.
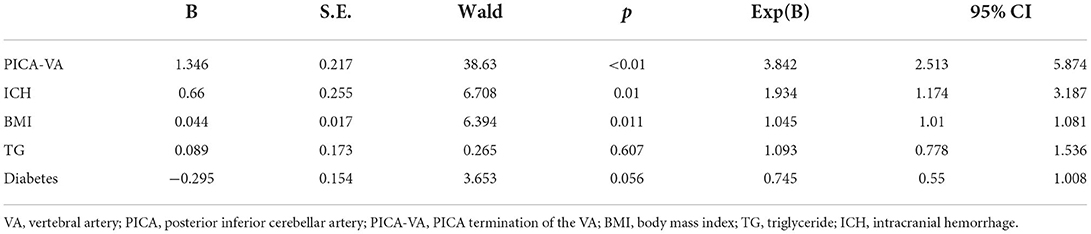
PICA-VA was independently correlated with vertebrobasilar strokeIn multivariate analysis for vertebrobasilar stroke as summarized in Table 3, PICA-VA was independently associated with a higher rate of vertebrobasilar stroke with an adjusted OR of 3.842 (95% CI = 2.513–5.874, p < 0.01). In addition, intracranial hemorrhage history (ORadjust = 1.934, 95% CI = 1.174–3.187, p = 0.01) and higher BMI (ORadjust = 1.045, 95% CI = 1.01–1.081, p = 0.011) remained significant risk factor.
Table 3. Multivariate logistic regression of risk factors of vertebrobasilar stroke.
DiscussionThe present study was a multicenter hospital-based cross-sectional study. Our data showed that 3.76% of acute stroke patients had a PICA-VA variant. PICA-VA was associated with the elevated incidence of vertebrobasilar stroke. The strength of the present study was that we demonstrated the prevalence of PICA-VA and identified its clinical significance in a relatively large sample.
The vertebrobasilar system supplies the brainstem, cerebellum, and part of the cortex. Variations were relatively common in the vertebrobasilar systems for 8–20.2% of hypoplastic VAs were observed (16). As for the intracranial part of VAs, the two intracranial VAs were usually asymmetrical and one might be 2–3 times the size of the remaining one (17). In some cases, the distal segment of intracranial VA from the origin of PICA to BA was absent and intracranial VA seemed to end in PICA in the angiogram (18), which was defined as PICA-VA (19). The prevalence of PICA-VA in different studies remained controversial. In the early time, DSA was used to determine the presence of PICA-VA. Osborn et al. found that only 0.07% of patients had this variation, and Greenberg et al. showed that 2% of the normal population had PICA-VA (20). Given the potential risk of DSA, many patients did not receive the DSA, which might have underdetermined the prevalence of PICA-VA. Liu et al. showed that 6.3% of PICA-VA in the normal population and 19% in patients with stroke, were higher than that of our study (7). In the present study, 3.76% of all patients with acute stroke and 9.28% of patients with vertebrobasilar stroke had a variation of PICA-VA. The differences may be due to the number of samples and the method used to detect the PICA-VA. Liu et al. only recruited 80 patients, while we included 2,528 patients. Moreover, Liu et al. used MRA to detect PICA-VA only. This may overestimate the prevalence because it was difficult to distinguish some asymptomatic isolated V4 occlusion from the PICA-VA by MRA. We screened the PICA-VA by MRA and then confirmed it with DSA. Our finding was partly consistent with a systematic review, which showed that 7.7% of vertebrobasilar stroke patients had PICA-VA (21).
The posterior inferior cerebellar artery had been recognized as the normal variation of intracranial VA (20). However, we found that PICA-VA was an independent risk factor for vertebrobasilar stroke. For patients with vertebrobasilar stroke, the variation was increased by about 2-fold times when compared to that without vertebrobasilar stroke (9.28 vs. 3.76%). This was the first study to demonstrate the clinical significance of PICA-VA. Moreover, we also showed there was the distribution of infarcts was different between patients with and without PICA-VA. Pontine infarction was the most abundant in patients without PICA-VA. For patients with PICA-VA, most of the infarcts occurred in the cerebellum, followed by the pontine. For the PICA-VA, the embolism would only occlude the PICA when the embolism goes through the ipsilateral VA. This might cause extra infarction in the cerebellum. For the general patients with vertebrobasilar stroke, pontine infarction was the dominant (14, 22).
The underlying mechanism of PICA-VA-induced vertebrobasilar stroke was still unknown. In the previous study, patients with PICA-VA were more prone to develop atherosclerosis than those without PICA-VA (23). VA diameter of the PICA-VA was significantly smaller, which was thought of as VA hypoplasia (6). The reason might be that there was higher asymmetry and resistance index, and lower mean flow and end-diastolic velocity in PICA-VA (7). Reduction in vertebral flow volume has been recognized as a predisposing factor for vertebrobasilar stroke (3). The high risk of atherosclerosis might increase the prevalence of stroke onset.
There were some limitations of the present study. First, the study was hospital based. The subjects in the present study had an acute stroke within 1 week. Normal people or other patients with non-acute strokes were not included. This may lead to some bias. Second, the vertebrobasilar stroke was performed based on the DWI image. The patients with DWI negative stroke and TIA were identified as patients with non-infarction. This may underestimate the prevalence of stroke. Diagnosis of TIA relied on the quality and quantity of information available and the time of assessment (24). However, the symptoms in the posterior circulation like isolated vertigo were normal in other patients with non-stroke (25). New infarction in the brainstem was hard to diagnose based on CT or other image modalities. In this way, we used MRI for the diagnosis of vertebrobasilar stroke.
ConclusionIn conclusion, our data showed that 3.76% of acute stroke patients had a PICA-VA variant, which was associated with a risk of vertebrobasilar stroke.
Data availability statementThe original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statementThe studies involving human participants were reviewed and approved by Ethics Committee of the Second Affiliated Hospital of Guangzhou Medical University. The patients/participants provided their written informed consent to participate in this study.
Author contributionsYJ: conceptualization. RH and KY: data collection. HC and ZD: investigation. JZ and YJ: formal analysis and writing. All authors contributed to the article and approved the submitted version.
FundingThis study was financially supported by the National Science Foundation of China (81471181 and 81870933), the Opening Lab Program of Guangzhou Medical University (0506308), Guangdong Basic and Applied Basic Research Foundation (2021A1515011351), Guangzhou Science and Technology Project (202102010127 to YJ), National Natural Science Foundation of China (Grant No. 82171282), Suzhou Mingsheng Science Technology Project (Grant No. 2020101), Scientific Research Project of Jiangsu Provincial Health and Wellness Committee (Grant No. M2020064), and Health Youth Backbone Project of Suzhou City (Qngg2021003 to JZ).
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References1. Sun Y, Shi YM, Xu P. The clinical research progress of vertebral artery dominance and posterior circulation ischemic stroke. Cerebrovasc Dis. (2022) 51:553–6. doi: 10.1159/000521616
PubMed Abstract | CrossRef Full Text | Google Scholar
2. Zhu W, Wang YF, Dong XF, Feng HX, Zhao HQ, Liu CF. Study on the correlation of vertebral artery dominance, basilar artery curvature and posterior circulation infarction. Acta Neurol. (2016) 116:287–93. doi: 10.1007/s13760-015-0570-5
PubMed Abstract | CrossRef Full Text | Google Scholar
3. Katsanos AH, Kosmidou M, Kyritsis AP, Giannopoulos S. Is vertebral artery hypoplasia a predisposing factor for posterior circulation cerebral ischemic events? A comprehensive review. Euro Neurol. (2013) 70:78–83. doi: 10.1159/000351786
PubMed Abstract | CrossRef Full Text | Google Scholar
4. Hu XY, Li ZX, Liu HQ, Zhang M, Wei ML, Fang S, et al. Relationship between vertebral artery hypoplasia and posterior circulation stroke in Chinese patients. Neuroradiology. (2013) 55:291–5. doi: 10.1007/s00234-012-1112-y
PubMed Abstract | CrossRef Full Text | Google Scholar
5. Nicolau C, Gilabert R, Chamorro A, Vazquez F, Bargallo N, Bru C. Doppler sonography of the intertransverse segment of the vertebral artery. J Ultrasound Med. (2000) 19:47–53. doi: 10.7863/jum.2000.19.1.47
PubMed Abstract | CrossRef Full Text | Google Scholar
6. Saito K, Kimura K, Nagatsuka K, Nagano K, Minematsu K, Ueno S, et al. Vertebral artery occlusion in duplex color-coded ultrasonography. Stroke. (2004) 35:1068–72. doi: 10.1161/01.STR.0000125857.63427.59
PubMed Abstract | CrossRef Full Text | Google Scholar
7. Liu IW, Ho BL, Chen CF, Han K, Lin CJ, Sheng WY, et al. Vertebral artery terminating in posterior inferior cerebellar artery: a normal variation with clinical significance. PLoS ONE. (2017) 12:e0175264. doi: 10.1371/journal.pone.0175264
PubMed Abstract | CrossRef Full Text | Google Scholar
8. Siclari F, Burger IM, Fasel JH, Gailloud P. Developmental anatomy of the distal vertebral artery in relationship to variants of the posterior and lateral spinal arterial systems. AJNR Am J Neuroradiol. (2007) 28:1185–90. doi: 10.3174/ajnr.A0498
PubMed Abstract | CrossRef Full Text | Google Scholar
9. Caplan LR. Vertebrobasilar Ischemia and Hemorrhage. 2 edition. Cambridge: Cambridge University Press (2015).
10. Aoyama T, Obara N. Vertebral artery terminating posterior inferior cerebellar artery (PICA-VA) as a potential risk factor in cervical spine surgery. World neurosurgery. (2020) 143:e535–40. doi: 10.1016/j.wneu.2020.08.003
PubMed Abstract | CrossRef Full Text | Google Scholar
11. Osborn AG. Diagnostic Cerebral Angiography. 2 edition. Philadelphia, PA: Lippincott Williams & Wilkins (1998).
12. Liu X, Xu G, Wu W, Zhang R, Yin Q, Zhu W. Subtypes and one-year survival of first-ever stroke in Chinese patients: the Nanjing stroke registry. Cerebrovasc Dis. (2006) 22:130–6. doi: 10.1159/000093241
PubMed Abstract | CrossRef Full Text | Google Scholar
13. Wu L, Li Y, Ye Z, Liu D, Dai Z, Zhu J, et al. Site and mechanism of recurrent pontine infarction: a hospital-based follow-up study. Brain Sci. (2022) 12:520. doi: 10.3390/brainsci12050520
PubMed Abstract | CrossRef Full Text | Google Scholar
14. Zhu J, Li Y, Wang Y, Zhu S, Jiang Y. Higher prevalence of diabetes in pontine infarction than in other posterior circulation strokes. J Diabetes Res. (2022) 2022:4819412. doi: 10.1155/2022/4819412
PubMed Abstract | CrossRef Full Text | Google Scholar
15. Qiu Z, Liu J, Huang R, Liu D, Dai Z, Luo M, et al. Incidence, risk, and treatment of binary restenosis after vertebral artery stenting. Catheter Cardiovasc Interv. (2020) 96:404–9. doi: 10.1002/ccd.28906
PubMed Abstract | CrossRef Full Text | Google Scholar
16. Songur A, Gonul Y, Ozen OA, Kucuker H, Uzun I, Bas O, et al. Variations in the intracranial vertebrobasilar system. Surg Radiol Anat. (2008) 30:257–64. doi: 10.1007/s00276-008-0309-6
PubMed Abstract | CrossRef Full Text | Google Scholar
17. Chuang YM, Chern CM, Liao WH, Hsu LC, Lien CF, Lirng JF, et al. Contribution of intracranial vertebral artery asymmetry to vestibular neuropathy. J Neurol Neurosurg Psychiatry. (2011) 82:823–5. doi: 10.1136/jnnp.2009.203323
PubMed Abstract | CrossRef Full Text | Google Scholar
18. Stopford JS. The arteries of the pons and medulla oblongata. J Anat Physiol. (1916) 50 (Pt. 2):131–64.
19. Isaji T, Yasuda M, Kawaguchi R, Aoyama M, Niwa A, Nakura T, et al. Posterior inferior cerebellar artery with an extradural origin from the V3 segment: higher incidence on the nondominant vertebral artery. J Neurosurg Spine. (2018) 28:154–9. doi: 10.3171/2017.5.SPINE161286
PubMed Abstract | CrossRef Full Text | Google Scholar
20. Greenberg MS, Arredondo N. Handbook of Neurosurgery. New York, NY: Thieme (2001).
23. Yu J, Zhang S, Li ML, Ma Y, Dong YR, Lou M, et al. Relationship between the geometry patterns of vertebrobasilar artery and atherosclerosis. BMC Neurol. (2018) 18:83. doi: 10.1186/s12883-018-1084-6
PubMed Abstract | CrossRef Full Text | Google Scholar
24. Wang Y, Wang Y, Zhao X, Liu L, Wang D, Wang C, et al. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack. N Engl J Med. (2013) 369:11–9. doi: 10.1056/NEJMoa1215340
留言 (0)