Design and Sample
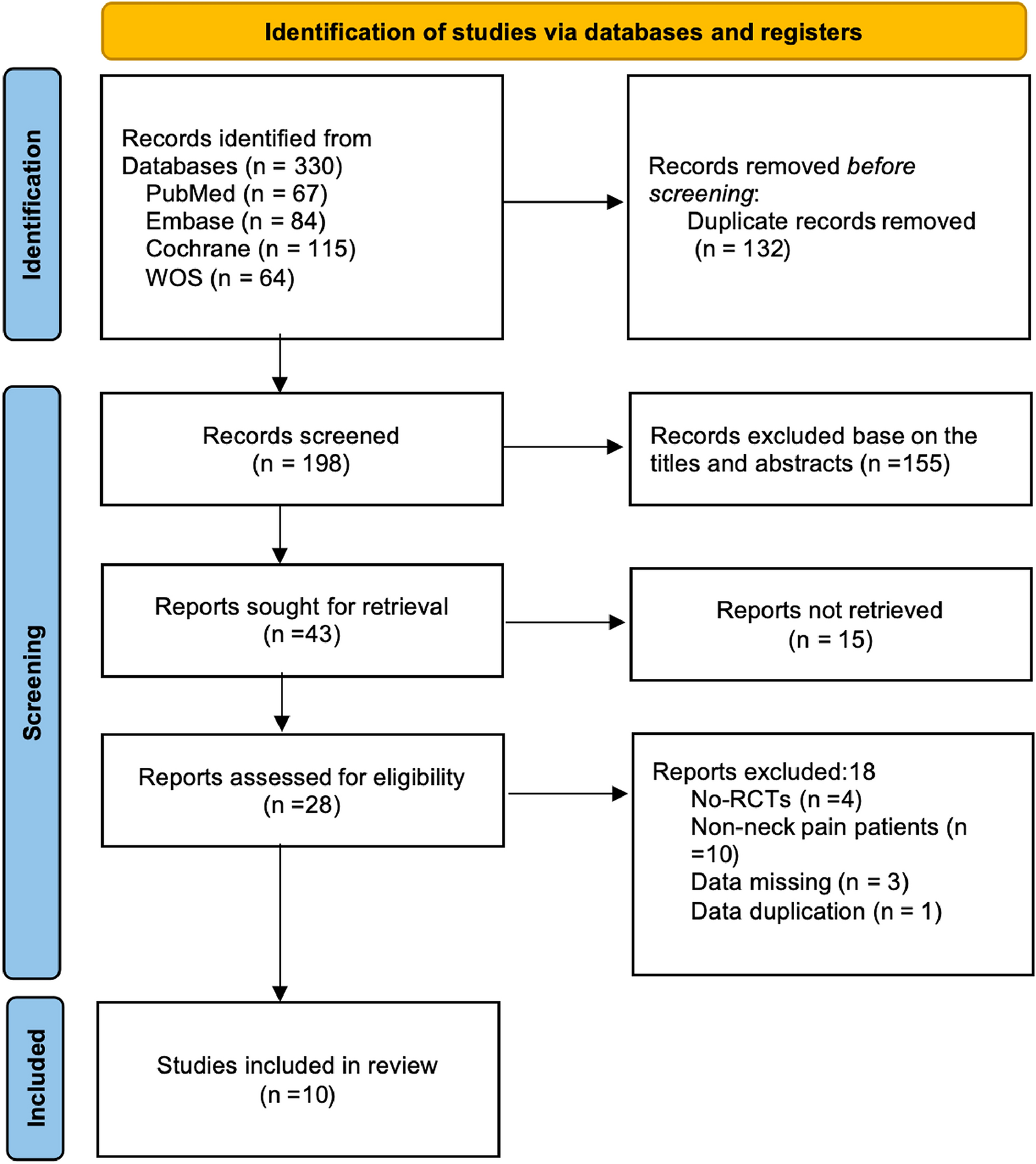
This retrospective study was conducted on 644 consecutive patients with chronic non-cancer pain who were referred by family doctors or specialists to the PWC for a medical pain consultation during a 24-month period (January 2016–December 2017). The study population was divided into two age groups: older population (≥ 65 years of age, n = 126) and younger population (< 65 years of age, n = 518). For this study, the older population (≥ 65) included individuals aged 65 and over and the younger population (< 65) included individuals 64 years old and up to but not more than 6 months. All patients filled out the standard PWC intake form which included a consent form (acceptance of the patient to use his or her data anonymously in aggregate format for research purposes) witnessed by administrative staff. This study was approved by the Research Ethics Board of University of Toronto (protocol number 36903).
Data Collection
Data were collected using standardized intake questionnaires completed by the patients at the time of their original consultation, as well as through retrospective chart review. These data included demographics (age, sex, place of birth, education, marital status, employment status) and pain characteristics (site, primary pain complaint, pain ratings on the Brief Pain Inventory, duration of pain). “Place or country of birth” was used as identifier and patients were classified as Canadian born (CB) and foreign born (FB).
Diagnosis was extracted from chart review by experienced PWC clinicians (through the detailed original consultation, review of records sent at time of referral, as well as additional reports and findings of investigations collected during follow-up appointments). Pain mechanisms were obtained from a detailed list of biomedical disorders established during data compilation, i.e. neuropathic pain (NP) disorders (including brain and spinal cord conditions, radiculopathies, neuropathies, etc.), nociceptive pain (NC) disorders (including osteoarthritis, soft tissue injuries, nociceptive visceral pains, etc.) and mixed conditions (neuropathic and nociceptive pain disorders).
Furthermore, the study population was divided into three diagnostic groups as follows: Group I patients have a significant biomedical condition(s) considered responsible for pain symptoms and disability while psychological influences are considered absent or minor. Group II patients have a combination of biomedical condition(s) and psychological/psychosocial factors affecting pain perception and disability. Group III patients lack findings consistent with biomedical conditions, present with high levels of emotional distress, disability and pain severity, and psychological/psychosocial factors are considered prominent in their presentation. The aforementioned categorization is based on our established clinical practice as follows: all patients are seen in our centre referred by their primary care physicians or specialists and are evaluated extensively by two pain team members, who obtain an explicit history regarding their pain problems, as well as detailed medical, surgical, psychiatric, and psychosocial history; review past and current medications and treatments received to date; as well as all imaging, medical reports and surgical consultations forwarded with the referral. The history is followed by detailed neuro-musculoskeletal examination, and if needed additional investigations. A group III diagnosis is not a diagnosis of exclusion, i.e. made solely on the basis of lack of detectable biomedical pathology (with current means available), but is based on clinical expert judgement that takes in account all sources of information (history, physical findings, behavioural observations, review of records, and laboratory/medical/surgical reports and findings). The aforementioned diagnostic classification has been explicitly described [12] and extensively used in previous publications from our group [12, 14,15,16,17,18]. A very small number of patients in both age groups in the present study were not given a diagnostic categorization because of lack of final diagnosis (e.g. investigations were not completed and/or the patient failed to show for follow-up).
In regard to opioid use, based on daily total morphine equivalent dosage (MED), the patients were classified as low opioid users (LOU) ≤ 90 mg/ day of morphine and high opioid users (HOU) ≥ 90 mg/day of morphine. The cut-off point of 90 mg/day between the two opioid user groups was defined by the 2017 Canadian guidelines for safe and effective use of opioids for chronic non-cancer pain [19]. Mean dose and range were calculated only for preparations taken regularly that could be converted to morphine equivalents. Additionally, current cannabis use was recorded at entry point.
Statistical Analysis
Statistical analysis was performed using SPSS (Statistical Package for the Social Sciences, version 16.0). Pearson’s chi-square test or goodness-of-fit test or chi-square test for independence was used to analyse contingency of demographic variables, pain characteristics, opioid users and diagnosis data between the elderly and younger population. Student’s t test was used to analyse pain ratings and opioid consumption between the elderly and younger subjects and binomial proportions were used for comparing individual variables between both the groups. At a 95% confidence interval, statistical significance was shown by using two-sided p value of less than 0.05. When the denominator is different as a result of missing data, the exact number will be indicated in brackets.









留言 (0)