
記住我










Background We sought to determine the prognostic value of transthoracic echocardiography (TTE)-derived right ventricular dysfunction (RVD) in haemodynamically stable and intermediate-risk patients with acute pulmonary embolism (PE), evaluate continuous RVD parameters, and assess the literature quality.
Methods We searched MEDLINE, Embase and the Cochrane Central Register of Controlled Trials for studies assessing TTE-derived RVD in haemodynamically stable PE that reported in-hospital adverse events within 30 days. We determined pooled odds ratios (ORs) using a random-effects model, created funnel plots, evaluated the Newcastle–Ottawa scale and performed Grading of Recommendations, Assessment, Development and Evaluation.
Results Based on 55 studies (17 090 patients, 37.8% RVD), RVD was associated with combined adverse events (AEs) (OR 3.29, 95% confidence interval (CI) 2.59–4.18), mortality (OR 2.00, CI 1.66–2.40) and PE-related mortality (OR 4.01, CI 2.79–5.78). In intermediate-risk patients, RVD was associated with AEs (OR 1.99, CI 1.17–3.37) and PE-related mortality (OR 6.16, CI 1.33–28.40), but not mortality (OR 1.63, CI 0.76–3.48). Continuous RVD parameters provide a greater spectrum of risk compared to categorical RVD. We identified publication bias, poor methodological quality in 34/55 studies and overall low certainty of evidence.
Conclusions RVD is frequent in PE and associated with adverse outcomes. However, data quality and publication bias are limitations of existing evidence.
AbstractRight ventricular dysfunction on echocardiogram is a frequent finding in pulmonary embolism and associated with adverse events. Publication bias and methodological limitations of existing studies highlight the need for well-designed prospective studies. https://bit.ly/3SNd4bE
IntroductionAcute pulmonary embolism (PE) is a leading cause of cardiovascular death, with a recent trend to increasing age- and sex-adjusted mortality [1, 2]. Once the diagnosis of PE is made, the 2019 European Society of Cardiology (ESC) guidelines recommend risk stratification based on haemodynamic stability, clinical prediction scores, cardiac biomarkers and imaging of the right ventricle (RV) using echocardiography or computed tomography [3]. High-risk patients are defined by the presence of haemodynamic instability, whereas intermediate-risk patients are haemodynamically stable but have a simplified PE severity index (SPESI) of >0 and/or evidence of RV dysfunction (RVD) and/or positive cardiac biomarkers.
Prior meta-analyses of haemodynamically stable patients have demonstrated that RVD on transthoracic echocardiography (TTE) is associated with an increased odds of short-term mortality in haemodynamically stable patients [4–6]. However, the presence of RVD has not been shown to alter the management of haemodynamically stable patients with PE [7]. The most recent meta-analysis published in 2014 included 3283 patients from 12 studies that were all published before 31 December 2011 [4]. This meta-analysis only used a single electronic database with two keywords and only evaluated in-hospital and 30-day all-cause mortality despite there being other clinically relevant outcomes. Additionally, some of the included studies had patients treated with upfront thrombolytic therapy, which differs from the contemporary guideline-based standard of practice for haemodynamically stable patients [4]. Although prior meta-analyses have been instrumental in advancing our knowledge of PE risk stratification, in the absence of an up-to-date and comprehensive meta-analysis, several knowledge gaps remain. No prior meta-analysis of haemodynamically stable patients has assessed the prognostic value of RVD on the more commonly used study end-point that includes a composite of adverse events and the prognostic value of RVD on PE-related mortality has not been performed since 2004 [8]. Two recent meta-analyses have shown a prognostic association of RVD in low-risk patients [9, 10], but since the introduction of these ESC risk categories, no meta-analysis has assessed the prognostic role of RVD in intermediate-risk patients. Additionally, TTE-defined RVD has historically been based on the presence of a composite definition including RV dilation, RV hypokinesis, tricuspid annulus plane systolic excursion (TAPSE), flattened/bowed septum, tricuspid regurgitation and/or elevated right atrial pressure. However, an increasing number of studies have evaluated quantitative continuous measures of RVD, which previous meta-analyses did not assess.
Therefore, the aims of this systematic review and meta-analysis were to: 1) estimate the association between TTE-derived RVD and adverse clinical outcomes (combined adverse events, all-cause mortality and PE-related mortality) in haemodynamically stable patients, 2) determine the association between TTE-derived RVD and adverse clinical outcomes in ESC-defined intermediate-risk patients, and 3) evaluate the association between quantitative continuous TTE variables of RVD on clinical outcomes, and 4) assess the quality of evidence contributing to the recommendation to consider TTE-derived RVD for risk stratifying haemodynamically stable PE.
MethodsThe protocol for this systematic review was pre-specified and was registered on the PROSPERO international prospective register of systematic reviews (CRD42020186110) on 5 July 2020 and is reported according to the PRISMA 2020 statement (table S1) [11].
Information sourcesWe searched MEDLINE (1950–20 October 2021), Embase (1980–21 October 2021) and the Cochrane Central Register of Controlled Trials (inception–October 2021) on 21 October 2021, as well as online grey literature with the assistance of a medical research librarian (supplementary methods). We focused on medical subject headings and keywords related to “pulmonary embolism” and “echocardiography”. Articles in the search were limited to the English language involving human subjects. Bibliographies of all included studies were reviewed for any other relevant articles. We did not contact authors for studies with insufficient data for extraction (i.e. studies reporting TTE-derived RVD but without association to outcomes).
Eligibility criteriaArticles were eligible for inclusion if they included adult patients (≥18 years old) with PE confirmed by computed tomography pulmonary angiography or ventilation/perfusion imaging, included haemodynamically stable patients (defined as systolic blood pressure >90 mmHg or low-risk or intermediate-risk by ESC criteria [3]), had TTE performed to identify a minimum of one sign of RVD and reported short-term (in-hospital or ≤30 days) outcomes including all-cause mortality, PE-related mortality, thrombolysis or mechanical thrombectomy, initiation of extracorporeal mechanical oxygenation, cardiac arrest, cardiopulmonary resuscitation or the initiation of catecholamines due to obstructive/cardiogenic shock.
Studies were excluded if they assessed paediatric populations, did not confirm the diagnosis of PE, only included haemodynamically unstable patients (high-risk/massive PE), performed upfront thrombolysis or catheter-directed therapies, did not assess RV function using TTE or if only long-term outcomes (>30 days) were reported. Reviews, editorials, case reports and case series were also excluded.
Selection processThe search results were uploaded into an online systematic review management platform (www.covidence.org). Articles were screened for inclusion based on title and abstract independently by two reviewers and discrepancies were resolved by consensus. For any articles meeting the screening criteria, full texts were reviewed independently by two reviewers and any discrepancies were resolved by consensus. If multiple articles with the same patient cohort met inclusion criteria, the single study containing the largest number of patients or that reported the most inclusive data evaluating the prognostic value of RVD was selected.
Data extractionData from each included article was manually extracted independently by two reviewers and any discrepancies were resolved by consensus. Data were entered into an electronic spreadsheet for analysis. This included manuscript details such as author, country, publication year and journal, as well as data on study design, patient demographics, PE diagnostic method, RVD definition, time from PE diagnosis to TTE, all outcome data and duration of follow-up.
We recorded the definition of RVD, including whether a single TTE measurement or a composite of TTE measurements was used. Individual pre-defined continuous measures of RVD were also recorded including TAPSE, right ventricular to left ventricular diameter ratio (RV/LV), tricuspid regurgitation peak gradient, pulmonary artery systolic pressure (PASP), estimated right atrial pressure, right ventricular fractional area change, peak lateral tricuspid annulus systolic velocity, right ventricular strain, pulmonary artery acceleration time, pulse wave Doppler velocity time integral (VTI) and stroke volume. All outcomes were recorded, including all-cause mortality, PE-related mortality, haemodynamic instability (systolic blood pressure <90 mmHg, hypoperfusion/shock or the use of catecholamines to maintain perfusion), cardiopulmonary resuscitation, mechanical ventilation, emergency fibrinolysis, embolectomy or the initiation of extracorporeal membrane oxygenation. Recurrent venous thromboembolism and major bleeding were only included when contained within a study's combined adverse events.
Risk of bias assessmentThe methodologic quality of included studies was assessed independently by two reviewers using the Newcastle–Ottawa Scale (NOS) with discrepancies resolved by consensus and studies were classified as poor, fair or good based on conversion to Agency for Healthcare Research and Quality (AHRQ) standards [12].
SynthesisWe used odds ratios (ORs) as the common measure of association. Wherever possible, unadjusted and adjusted ORs were recorded and, when not reported, primary data was used to manually calculate the unadjusted OR. Pooled estimates, expressed as the most adjusted ORs (with 95% confidence interval (CI)), were generated using DerSimonian and Laird random effects models and visualised using forest plots. In studies with no events in patients without RVD, a Yates correction factor was used [13]. Inter-rater agreement was assessed using percentage agreement and the kappa statistic. Between-study heterogeneity was examined and quantified using Cochran's Q test and I2 statistics [14]. Stratification and meta-regression were conducted on the following variables: prospective versus retrospective, whether the primary aim of study was to evaluate TTE-derived RVD, time from diagnosis to TTE, timing of publication in relation to the 2014 ESC guidelines and study quality. We assessed for publication bias by generating funnel plots. Additionally, we performed a grading of recommendations assessment, development and evaluation (GRADE) analysis to assess the certainty of evidence for each outcome [15].
The meta-analysis was performed using the “metan’ command within Stata 15 (Stata Statistical Software: release 15. College Station, TX: StataCorp LLC.). Level of significance was set at α=0.05.
ResultsArticle selectionA total of 6402 citations were identified as of 21 October 2021, and 1757 duplicates were removed, depicted in the PRISMA flow diagram (figure 1). In total, 4675 titles and abstracts were screened and 4394 articles were excluded. The inter-rater study inclusion agreement for screening was 95.2% (κ=0.54; CI 0.51–0.57). A total of 251 articles underwent full-text review for eligibility. From these, 196 were excluded, leaving 55 unique studies (references for included studies in the supplementary material). The overall inter-rater study inclusion agreement for full-text review was 83.3% (κ=0.56; CI 0.44–0.68). The most common reasons for exclusion were insufficient data reported for extraction, primary treatment with thrombolysis or thrombectomy, and long-term or no outcomes reported. Seven studies meeting inclusion criteria were excluded after identifying duplicate data in another included publication.
 FIGURE 1
FIGURE 1 PRISMA diagram showing literature search and selection of right ventricular dysfunction (RVD) in pulmonary embolism (PE) articles [11]. A total of 6402 articles were identified (1757 duplicates removed). 4675 articles were screened by title and abstract with 251 articles determined for eligibility. 196 articles were excluded, leaving a total of 55 articles that were included in the systematic review. VQ: ventilation/perfusion; CT: computed tomography; RVD: right ventricular dysfunction; TTE: transthoracic echocardiography.
Results of individual studiesA summary of the study characteristics is shown in table 1 and detailed individual study information is provided in table S2. A total of 17 090 haemodynamically stable patients (52.8% were female) with a TTE were included. There were 5399 (37.8%) patients with RVD. 37 studies (67.3%) used a composite definition of RVD based on an average of 3.0±1.2 TTE criteria, while 18 studies (32.7%) used individual variables to define RVD. Components of the combined adverse events assessed in these studies included all-cause mortality (n=20), PE-related mortality (n=12), haemodynamic instability defined as systolic blood pressure <90 mmHg or initiating catecholamines for hypoperfusion/shock (n=31), cardiac arrest or cardiopulmonary resuscitation (n=21), mechanical ventilation (n=15), thrombolysis/catheter-directed therapies/initiation of extracorporeal membrane oxygenation (n=22), recurrent venous thromboembolism (n=2) and major bleeding (n=1).
TABLE 1Summary characteristics of articles included in the systematic review
Results of synthesisThe forest plots for haemodynamically stable patients (figure 2) showed that the presence of RVD was associated with a 3.3-fold higher odds of combined adverse events (OR 3.29, 95% CI 2.59–4.18; 29 studies; I2=26.5%), a fourfold higher odds of PE-related mortality (OR 4.01, CI 2.79–5.78; 17 studies; I2=6.1%) and a twofold higher odds of all-cause mortality (OR 2.00, CI 1.66–2.40; 24 studies; I2=9.6%).
 FIGURE 2
FIGURE 2 Forest plots for studies assessing right ventricular dysfunction (RVD) in pulmonary embolism (PE) for a) combined adverse events, b) all-cause mortality outcome and c) PE-related mortality outcome. Dashes (–) represent missing data. All weights are from the random-effects model. References can be found in the data supplement. CI: confidence interval; DL: DerSimonian and Laird. #: Yates correction.
The forest plots for ESC-defined intermediate-risk patients (figure 3) showed that RVD was associated with a twofold higher odds of combined adverse events (OR 1.99, CI 1.17–3.37; seven studies, I2=33.8%), and a sixfold higher odds of PE-related mortality (OR 6.16, CI 1.33–28.40; three studies, I2=51.5%), but was not associated with all-cause mortality (OR 1.63, CI 0.76–3.48; four studies, I2=33.9%).
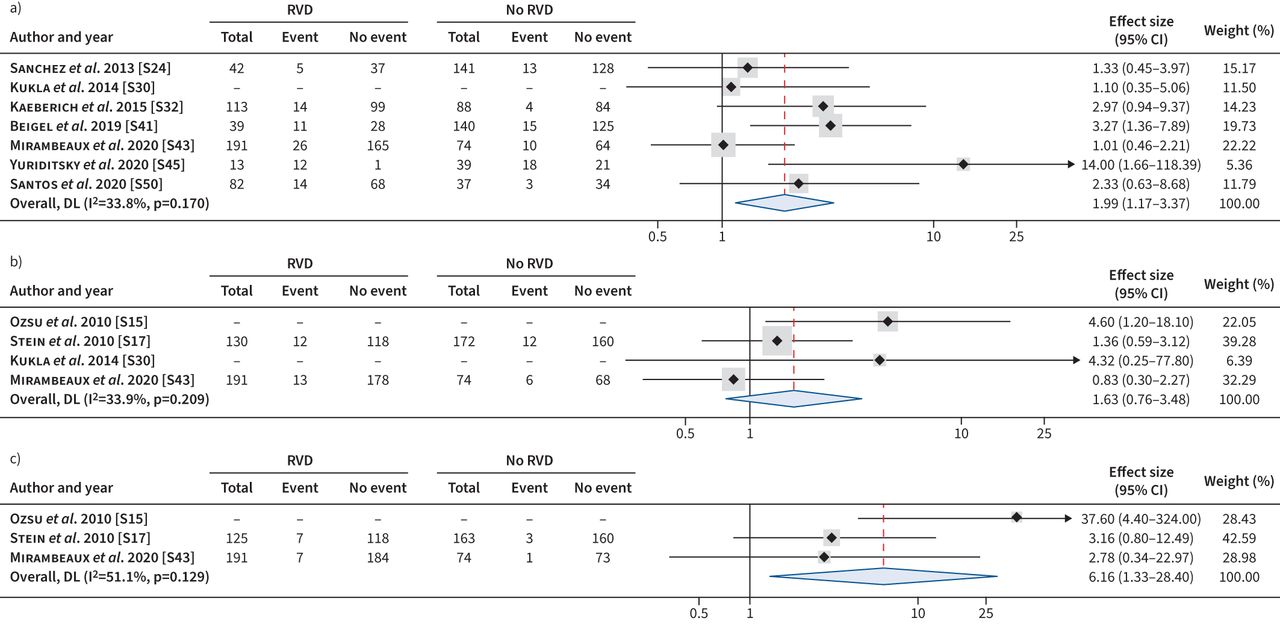 FIGURE 3
FIGURE 3 Meta-analysis of studies assessing right ventricular dysfunction (RVD) in pulmonary embolism (PE) for haemodynamically stable patients at intermediate risk of outcomes. a) Combined adverse events. b) All-cause mortality. c) PE-related mortality. Dashes (–) represent missing data. All weights are from the random-effects model. References can be found in the data supplement. CI: confidence interval; DL: DerSimonian and Laird.
Only RV/LV ratio, TAPSE and PASP had sufficient studies (≥3) to perform pooled meta-analysis of the quantitative, continuous measures of RVD for combined adverse events and all-cause mortality outcomes (figure 4). For each unit increase in RV/LV ratio, the odds of all-cause mortality increased by over 2.5-fold (OR 2.79, CI 1.92–4.04; three studies, I2=0.0%), every 1 mm decrease in TAPSE increased the odds of combined adverse events by 1.3-fold (OR 1.31, CI 1.03–1.67; three studies, I2=85.0%), and for every 10 mmHg increase in PASP the odds of a combined adverse event increased by 1.5-fold (OR 1.47, CI 1.24–1.73; three studies, I2=20.7%).
 FIGURE 4
FIGURE 4 Individual measures of right ventricular dysfunction (RVD) showing the pooled odds ratios of a) decreasing tricuspid annulus plane systolic excursion (TAPSE) per mm on combined adverse events, b) decreasing TAPSE per mm on all-cause mortality, c) increasing right ventricular to left ventricular diameter ratio (RV/LV) per 1 unit change on combined adverse events, d) increasing RV/LV per 1 unit change on all-cause mortality, e) increasing pulmonary artery systolic pressure (PASP) per 10 mmHg on combined adverse events and f) increasing PASP per 10 mmHg on all-cause mortality. All weights are from the random-effects model. References can be found in the data supplement. CI: confidence interval; DL: DerSimonian and Laird.
Subgroup meta-regression analysis (table 2) showed that using early outcomes (in-hospital or ≤14 days versus <14–30 days) were more strongly associated with all-cause mortality (p=0.011) and studies published after the 2014 ESC guidelines were more strongly associated with PE-related mortality (p=0.010). Importantly, there was no difference in the pooled effect size regardless of the timing of TTE from PE diagnosis (<24 h versus 24–72 h; p>0.05 for all outcomes). However, the presence of RVD was more common in studies where TTE was performed within 24 h compared to within 24–72 h (951/2026 versus 2579/5989, p<0.001).
TABLE 2Subgroup analysis showing the difference between study design for the studies with combined adverse events, all-cause mortality and pulmonary embolism (PE)-related mortality
Study quality and risk of bias assessmentAll studies were observational with 54 cohort designs and one case-control study. The methodologic quality of each study based on the NOS (table S3) showed that overall this body of literature suffers from poor methodologic rigour (figure S1). In the selection category, articles frequently lost points because the study cohort excluded haemodynamically stable PE without TTE resulting in selection bias and because of missing information on how included subjects were identified. In the comparability category, articles frequently lost points due to lack of adjustment for confounding variables. In the outcomes category, articles frequently lost points for missing information on outcome identification/adjudication or lacked information on the completeness of follow-up. Based on the NOS conversion to AHRQ standards, 18 articles were identified to be good quality, three were fair quality and 34 were poor quality studies. Funnel plot analysis (figure S2) showed evidence of publication bias for combined adverse events (p=0.013), all-cause mortality (p=0.021) and PE-related mortality (p=0.038). The funnel plot asymmetry observed suggests the potential for publication bias towards studies with large positive effect sizes.
Certainty of evidenceWe took a GRADE approach to assess the certainty of evidence (table S4) [15]. The results identified a risk of publication bias based on funnel plot analysis, minimal adjustment for potential cofounders and a lack of reporting the completeness of follow-up for all outcomes assessed. There was only minimal heterogeneity for each of the outcomes assessed despite the TTE criteria defining RVD and the criteria used to define adverse events being highly variable between studies. The effect sizes for combined adverse events and PE-related mortality were large, and those for all-cause mortality were moderate – all with CIs far from the line of null effect. The overall quality ratings for the prognostic value of RVD in haemodynamically stable PE for combined adverse events, all-cause mortality and PE-related mortality were all low.
DiscussionThis systematic review and meta-analysis included 17 090 patients from 55 studies and found that haemodynamically stable patients with PE who demonstrate RVD on TTE have increased odds of combined adverse events, all-cause mortality and PE-related mortality. In intermediate-risk patients, we observed a less pronounced association between RVD and combined adverse events and no significant association between RVD and all-cause mortality. However, there was a greater association between RVD and PE-related mortality, albeit with a wide CI. Finally, we observed an association between adverse events and three quantitative continuous measures of RVD including RV/LV, TAPSE and PASP, which are variables that may provide a wider spectrum of risk assessment and may be more useful to identify patients at the highest risk. Overall, in this largest and most rigorous systematic review to date, there was evidence of publication bias, poor methodologic rigour of primary studies, and the overall GRADE certainty of evidence was low.
Three prior meta-analyses have assessed the prognostic value of TTE-derived RVD in haemodynamically stable patients, all of which evaluated short-term all-cause mortality as the primary outcome. First, in 2004, ten Wolde et al. [8] identified an OR for short-term all-cause mortality of 5.1 (CI 2.8–9.2; n=5) including 746 patients (calculated from reported raw data). In 2011, Coutance et al. [5] reported a pooled OR for all-cause mortality of 2.4 (CI 1.3–4.3, I2=0%; n=8) including 1249 patients. Most recently, Cho et al. [4] identified a pooled OR of 2.29 (CI 1.61–3.26, I2=28%; n=12) for short-term in-hospital/30-day mortality including 3283 patients. There is a trend towards a reduction in association between RVD and all-cause mortality after each meta-analysis. The decrease in the magnitude of association over time may actually reflect an increased use of TTE, leading to more frequent and prolonged admissions for monitoring and inpatient management preventing or intervening early during decompensation [16] or changes in temporal anticoagulation strategies away from unfractionated heparin and warfarin towards low molecular weight heparin and direct oral anticoagulants [17]. Additionally, we found that the pooled OR for TTE-derived RVD for the outcome of PE-related mortality was 4.01 (2.79–5.78, I2=6.1%) based on 17 studies which had not been evaluated since the 2004 ten Wolde et al. [8] meta-analysis, which reported an OR of 28.9 (CI 6.8–122.4) in haemodynamically stable patients based on five studies including 746 patients (calculated from raw data). Overall, the trend over time seems to suggest a diminishing prognostic value of TTE-derived RVD in PE. In our study we found that the association between RVD and PE-related mortality was numerically greater than all-cause mortality. Becattini et al. [9] showed a similar trend in low-risk patients where the prognostic association of RVD was numerically greater for PE-related mortality compared with all-cause mortality at 3 months. This may suggest that PE-related mortality is a more robust outcome and should be used in future studies.
This meta-analysis also assessed the prognostic value of TTE-derived RVD in intermediate-risk of outcomes by ESC criteria (SPESI>0 and/or positive cardiac biomarkers and/or imaging evidence of RVD), which has not been previously assessed. Interestingly, there seems to be a numerical trend of a diminishing prognostic value of RVD with increasing risk categories. In a meta-analysis of low-risk patients, Becattini et al. [9] showed that RVD identified on TTE carried an OR for in-hospital/30-day mortality of 5.86 (CI 2.3–14.86) compared with our data showing an OR of 2.00 (CI 1.66–2.40) in haemodynamically stable patients and 1.63 (CI 0.76–3.48) in intermediate-risk patients [9]. While this trend is only hypothesis-generating due to the few studies with intermediate-risk patients that we identified, it is possible that as patients develop additional markers of risk, they may become pre-selected where categorical RVD becomes more common and less specific for adverse events.
We assessed the prognostic value of quantitative continuous TTE markers of RVD on outcomes, as these measures can provide a spectrum of risk which is clinically useful. Unfortunately, only TAPSE, RV/LV and PASP had an adequate number of studies (≥3) for pooled analysis. Continuous measures of RVD seem to provide a more clinically relevant spectrum of risk, although these should be considered hypothesis-generating given the relatively few studies and limited number of continuous markers of RVD. There are numerous other promising markers of RVD that leverage the pathophysiology of reduced cardiac output [18–20] and RV–pulmonary artery decoupling [21–24], which did not have enough studies with similar outcomes for analysis.
We performed several novel subgroup analyses that may have implications for clinical practice. We found that the timing of TTE from diagnosis (≤24 h versus ≤48–72 h) did not affect the prognostic value of RVD, suggesting that haemodynamically stable patients can undergo TTE within 72 h of diagnosis without altering its prognostic value. However, we also found that patients with early TTE (<24 h) had a greater proportion of RVD than patients with delayed TTE (<24–72 h), which may suggest that some patients recover their RV function quickly with initial anticoagulation management alone or that some selection bias exists in these studies where sicker patients who were more likely to have RVD underwent more urgent TTE in based on clinical factors. We found that RVD was more strongly associated with early events (in-hospital or ≤14 days versus <14–30 days) for all-cause mortality but not combined adverse events or PE-related events, which may suggest that RVD identifies a more comorbid population at risk of early mortality but not necessarily mortality due to cardiogenic/obstructive shock from PE. Lastly, we found that the prognostic association between RVD and PE-related mortality increased significantly following the 2014 ESC guidelines. This difference seems to be driven by using TAPSE to define RVD in 2/4 of these studies published after the 2014 guidelines, which may suggest a greater prognostic value for TAPSE compared to traditional composite measures of RVD.
Current ESC guidelines provide a class IIa recommendation to consider RV assessment by imaging methods or laboratory markers in all patients regardless of risk category [3]. However, apart from increased hospital monitoring, the presence of RVD in haemodynamically stable patients has failed to alter initial management based on the PEITHO trial of fibrinolytic therapy [7]. The presence of traditional TTE RVD definitions isubiquitous in haemodynamically stable PE (37.8% of patients in this meta-analysis). Similar to the PEITHO trial that defined RVD by the presence of RV end-diastolic diameter>30 mm or RV/LV>0.9 or hypokinesis of the RV free wall or tricuspid regurgitation velocity >2.6 m·s−1, 70% of the studies in this meta-analysis used similar composite definitions of RVD [7]. Given its high prevalence, these current definitions of RVD lack specificity to define a truly intermediate–high risk subpopulation that might benefit from upfront reperfusion strategies. Strategies to increase the positive predictive value of TTE-derived RVD are needed to identify patients at higher risk of PE-related events. It is possible that new RVD parameters such as VTI or RV–pulmonary artery decoupling [18–24] using higher thresholds to define RVD or continuous measures of RVD that provide a spectrum of risk in combination with multimodality approaches that incorporate imaging, biomarkers and clinical data may enhance PE risk stratification in the future [25, 26].
Several limitations are acknowledged related to the study designs included and the overall quality of the literature. All studies were observational and few studies performed adjusted/multivariate analysis to account for potential confounders. Multivariate/adjusted analysis was seldom reported (2/29 of studies reporting combined adverse events, 3/24 for studies reporting all-cause mortality and 2/17 studies reporting outcomes for PE-related mortality). Funnel plots showed significant bias exists towards the publication of studies where RVD had large effect sizes for all outcomes studied. However, funnel plots are intended to detect small study effects which are challenging to interpret for meta-analyses of observational studies, such as ours, where multiple sources of heterogeneity may be present, such as those arising from true clinical differences (e.g. different definitions of RVD) or bias inherent to individual studies (e.g. residual confounding and lack of blinding) [27].
ConclusionsIn haemodynamically stable patients with PE, TTE-derived RVD is associated with increased odds of short-term combined adverse events, all-cause mortality and PE-related mortality. However, the prevalence of RVD is over 37% in this population and current definitions lack specificity to meaningfully change clinical management. In intermediate-risk patients, the prognostic value of RVD is less robust with an increased odds of combined adverse events and PE-related mortality but not all-cause mortality. The finding of publication bias, frequently poor methodologic rigour in the primary studies, infrequent adjustment for confounders and an overall low GRADE certainty of evidence questions the robustness of RVD's association with outcomes from this meta-analysis and those prior. To advance the field of PE risk stratification, TTE-derived RVD indices with high predictive value for PE-related events are needed in conjunction with multimodality risk stratification to enrich future studies of reperfusion therapy in patients who are at higher risk of cardiopulmonary decompensation. Future well-designed prospective studies are needed to evaluate TTE-derived RVD variables with a high positive predictive value to identify those patients at highest risk of adverse clinical events for consideration of systemic thrombolysis or other invasive interventions.
Supplementary materialSupplementary MaterialPlease note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERR-0120-2022.SUPPLEMENT
FootnotesProvenance: Submitted article, peer reviewed.
Availability of data: Publicly available data collection, data used, and analytic code is available upon request to the corresponding author.
Conflicts of interest: J. Weatherald reports grants or contracts from Janssen, Actelion, Bayer, Canadian Institutes for Health Research and Heart & Stroke Foundation of Canada; consulting fees from Janssen and Actelion; honoraria from Janssen; payment for expert testimony from Spigings Intellectual Property Law; travel support from Janssen; and participation on a Data Safety Monitoring Board or Advisory Board for Janssen, Acceleron and Université Laval. J. Weatherald is a member of the Medical Advisory Committee of the Pulmonary Hypertension Association of Canada. He is a shareholder in a pulmonary function testing laboratory (Precision Lung Consultants and Diagnostics). All other authors have no conflicts to declare.
Received June 29, 2022.Accepted August 1, 2022.Copyright ©The authors 2022http://creativecommons.org/licenses/by-nc/4.0/This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissionsersnet.org
留言 (0)