
記住我
Trampolining is a popular form of recreation and trampolines are among the most common gifts to school age children and pre-adolescents.1 However, trampolining poses a significant risk of injury, which accounts annually for nearly 100 000 paediatric emergency visits in the USA.2 In the United Kingdom (UK), there were 11500 presentations to emergency departments (EDs) due to trampoline-related injuries in 2002.1 In Australia, almost 15 000 children (~1500 annually) were hospitalised for trampoline injuries between 2002 and 2011.3 Injury surveillance systems, which use hospital admission data as a proxy of injury severity, have concluded that trampoline-related injuries lead to more hospitalisations than injuries suffered in other sports or recreational activities.4
In light of the significant health burden from trampoline injuries, the American Academy of Pediatrics (AAP), the American Academy of Orthopedic Surgeons, and the Canadian Paediatric Society have issued policy statements advising against the recreational use of home trampolines.5 6 In response to safety concerns, industry safety standards have been developed globally to reduce potential hazards associated with the manufacture, assembly, maintenance and use of trampolines, but despite this, rates of trampoline injuries have not declined.3 7 8
Most trampoline injuries that occur within the home environment result from improper landing onto or falling off the trampoline.4 9 However, there is emerging evidence that injuries sustained at trampoline centres are more severe and the frequency of these injuries are rising dramatically.10–14 The number and popularity of trampoline centres have skyrocketed over the past decade: there are currently about 840 commercial trampoline centres in the USA and over 400 were reported in other countries in 2017.15 16 Recreational trampoline centres are characterised by a patchwork of connected trampoline surfaces that entertain large groups of jumpers in close proximity, potentially creating conditions for collisions and falls.5 9 Due to differences in the use, design, layout and build between trampolines centres and home trampolines, it has been suggested that commercial trampoline centres might be altering the nature and spectrum of associated injuries.2 9 17 Each commercial trampoline centre franchise has different safety guidelines with no consistent approach.5
We conducted a systematic literature review and meta-analysis to: (1) summarise the existing evidence on trampoline injuries by type and site of injury and treatment required (including hospital admission and surgery); and (2) present pooled results from all available observational studies that reported trampoline-related injuries sustained at trampoline centres and in the domestic setting (home or backyard trampolines).
MethodsSearch strategy and selection criteriaThis systematic review and meta-analysis followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines for reporting.18 A systematic search of the databases MEDLINE, Scopus, Google Scholar and Embase was performed up to 31 December 2021 to identify relevant articles (figure 1). Our search terms included ((trampoline) AND (wound and injuries) OR (trauma) OR (accident) OR (injury)). The reference lists of relevant articles were also searched for appropriate studies. No language or age restrictions were used in either the search or study selection. No search for unpublished literature was performed.
 Figure 1
Figure 1 Results of the literature search. PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses. Reproduced with permission from Page et al.33
We included studies that: (1) reported trampoline injuries at home and in trampoline centres; (2) reported the risk point estimate as an odds ratio (OR), or presented data that enabled an OR to be calculated; (3) reported the 95% confidence interval (95% CI), or presented data that allowed the 95% CI to be calculated; (4) used an internal comparison when calculating the risk estimate.
Data extractionData extraction was performed using a standardised form and included information on the publication year, study design, population type, country, sample size, mean age, number of adjusted variables, risk estimates or data used to calculate the risk estimates, and confidence intervals or data used to calculate 95% CIs. Study quality was assessed using the Newcastle-Ottawa Scale Quality Assessment (NOS) (online supplemental appendix 1). Adjusted ratios were extracted in preference to non-adjusted ratios; however, where adjusted ratios were not provided, unadjusted ORs and 95% CIs were calculated. Where more than one adjusted ratio was reported, we chose the ratio with the highest number of adjusted variables. Where multiple risk estimates were available in the same study, for example, due to the use of different comparator groups, they were included as separate risk estimates. Severity of an injury was determined based on the treatment required whether non-surgical treatment (non-severe) or surgical intervention was recommended (severe).
Data analysisPooled ORs and 95% CIs were calculated using a random-effects model for the risks of injuries sustained in commercial trampoline centres compared with home trampolines, by type and site, and requirement for hospital admission or surgery.19 Heterogeneity was assessed using the I² statistic: 0–25% (low), 25–75% (moderate), and >75% (high) levels of heterogeneity.20 We assessed publication bias using Egger’s regression model only if there were more than 10 studies.21 22 All analyses were performed with Comprehensive Meta-analysis (version 3.0), Biostat, Englewood, NJ, USA (2014).
ResultsA total of 154 articles were identified in the literature review, of which 11 studies (1386843 injuries) were included in this meta-analysis based on our inclusion criteria (figure 1). Table 1 presents selected characteristics of the identified studies, including authors, year of publication, study type, population sample, country, sample size, mean age in years, sex, and NOS score. Overall, children who sustained an injury at a trampoline centre were older than those whose injury occurred at home. In most studies, the proportion of injuries by sex were similar between trampoline centres and home trampolines. Four studies were conducted in the USA, two in South Korea, and one each in Canada, UK, Singapore, Australia and New Zealand. Of the four studies in the USA, three used data from the National Electronic Injury Surveillance System (NEISS) (https://www.cpsc.gov/Research--Statistics/NEISS-Injury-Data) and the most complete or recent results were used. All the studies were cross-sectional with fair quality based on the NOS assessment (table 1).
Table 1Characteristics of the studies included in the meta-analysis
Abrasion was investigated as an outcome in two studies (online supplemental appendix 2); the pooled estimate showed a reduced likelihood for abrasions at trampoline centres compared with home trampolines. The OR was 0.69 (95% CI 0.46 to 1.03, p=0.07); moderate but not significant heterogeneity was observed (I2=73.76, p=0.05). Laceration was assessed in three studies; the pooled OR showed a reduction in likelihood for this outcome in a trampoline centre (OR 0.46, 95% CI 0.35 to 0.59, p<0.001), with high heterogeneity detected (I2=78.31, p=0.01) (figure 2). Sprains occurred more often at trampoline centres than at home trampolines (OR 1.64, 95% CI 1.36 to 1.97, p<0.001; I2=54.46, p=0.09). Soft tissue injuries were no more likely at trampoline centres (OR 1.36, 95% CI 0.36 to 5.14, p=0.66; I2=95.33, p<0.001).
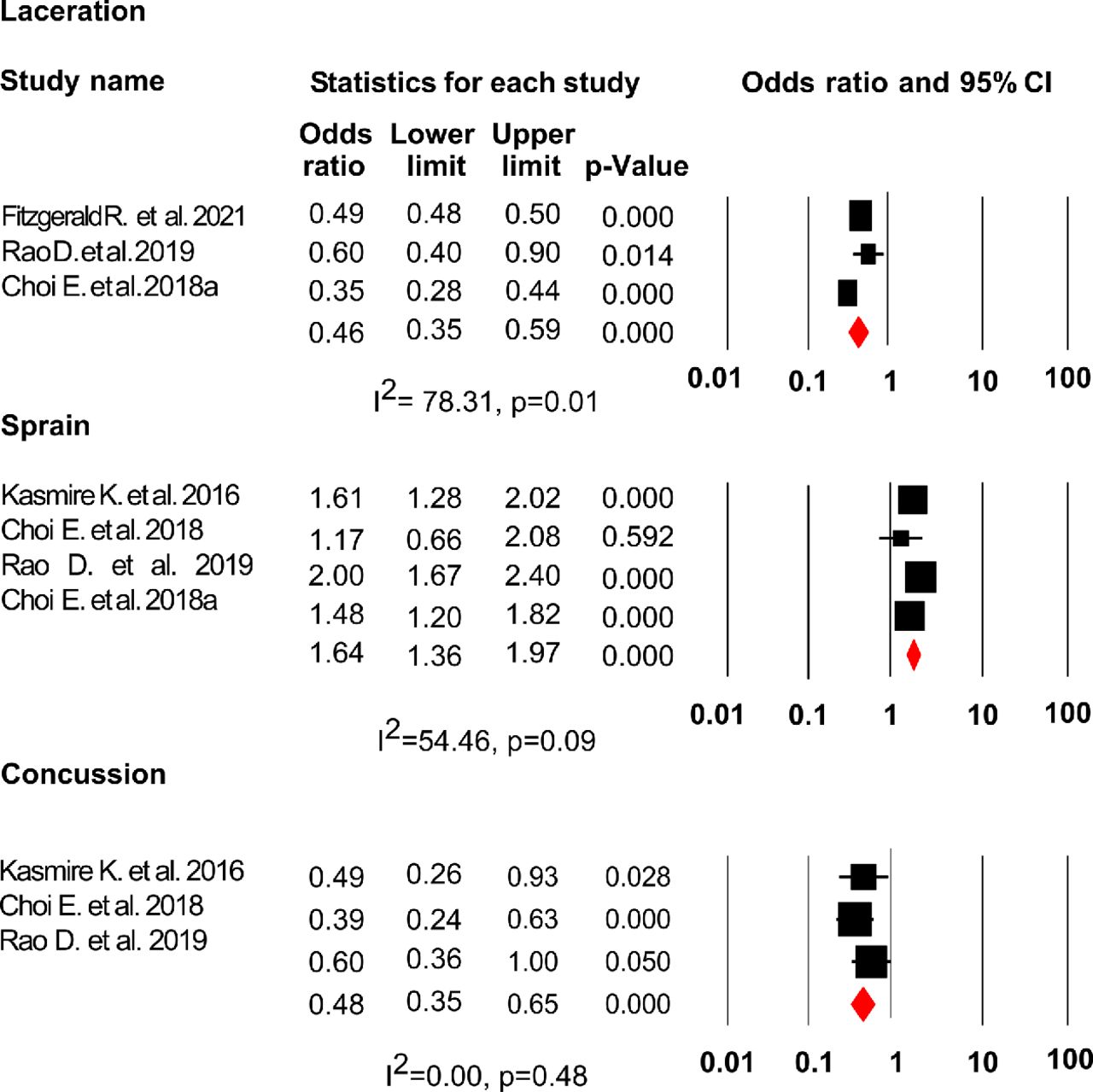 Figure 2
Figure 2 Pooled OR and 95% CIs of non-severe trampoline injury risk according to location (trampoline centre vs home trampoline (reference)).
There was no difference in the likelihood of head and facial injuries (OR 0.50, 95% CI 0.20 to 1.21, p=0.13; I2=96.76, p<0.001) or injuries to the trunk region of the body (OR 0.97, 95% CI 0.59 to 1.58, p=0.90; I2=37.11, p=0.19) between trampoline centres and home trampolines. Concussion was less likely to occur at trampoline centres than at home (OR 0.48, 95% CI 0.35 to 0.65, p<0.001; I2=0.00, p=0.48).
Three studies examined the likelihood of sustaining a dislocation on a trampoline (online supplemental appendix 3); there was no increased likelihood of dislocations occurring at trampoline centres compared with at home (OR 1.17, 95% CI 0.66 to 2.05, p=0.59); moderate but not significant heterogeneity was observed (I2=61.30, p=0.07). The risk of fractures was assessed in six studies; there was no difference in risk (OR 1.11, 95% CI 0.84 to 1.49, p=0.46; I2=87.38, p<0.001) in trampoline centres or at home. Six studies investigated lower extremity injuries and five investigated upper extremity injuries; lower extremity injury was more likely to occur in a trampoline centre (OR 2.81, 95% CI 1.99 to 3.97, p<0.001; I2=93.52, p<0.001) whereas upper extremity injury was less likely to occur at a trampoline centre (OR 0.49, 95% CI 0.25 to 0.95, p=0.03; I2=96.58, p<0.001) (figure 3). Lower extremity injuries were no more likely to occur in children and adolescents than adults (OR 1.25, 95% CI 0.74 to 2.11, p=0.41; I2=0.00, p=0.87) (online supplemental appendix 4).
 Figure 3
Figure 3 Pooled OR and 95% CIs of severe trampoline injury risk according to location (trampoline centre vs home trampoline (reference)).
Musculoskeletal and/or orthopaedic injuries were examined in two studies; the pooled OR indicated a more than two-fold increased likelihood for these injuries at trampoline centres (OR 2.45, 95% CI 1.66 to 3.61, p<0.001; I2=0.00, p=0.34). A total of four studies analysed the risk of spinal injuries but there was no difference between trampoline centres and home trampoline (OR 1.83, 95% CI 0.84 to 3.98, p=0.13; I2=87.38, p<0.001).
There was no difference in the risk of hospital admission for injuries sustained at trampoline centres compared with home trampolines (OR 1.16, 95% CI 0.56 to 2.41, p=0.69; I2=85.53, p<0.001). However, the risk of requiring surgery was significantly higher if the injury was sustained in a trampoline centre (OR 1.89, 95% CI 1.37 to 2.60, p<0.001; I2=0.00, p=0.93). Children under 6 years of age were less likely to be injured in trampoline centres than at home (OR 0.52, 95% CI 0.30 to 0.90, p=0.02; I2=58.31, p=0.09) (online supplemental appendix 5). A summary of all outcomes assessed in this meta-analysis is provided in online supplemental appendix 6.
DiscussionWe believe this is the first systematic review and meta-analysis to have assessed the level of evidence regarding the likelihood of various types of injuries sustained at commercial trampoline centres compared with trampolines at home. In principle, trampoline-related injuries sustained at trampoline centres and at home should share common characteristics, but findings from this study suggest a different pattern of injuries in these two settings. This important information has not been previously reported in the medical literature and has implications for safety policy.
Lower extremity injuries, sprains, and requirement for surgical intervention were more prevalent at trampoline centres. This may relate to structural differences in the trampoline mat used in the home and at trampoline centres.7 The higher tensile strength used in commercial trampoline centres may produce a harder bounce which amplifies the loading in bones and ligaments.7 13 23 Similar high-energy impact is observed when double bouncing on a trampoline.23 Computational biomechanical modelling based on two trampoline users shows that there is a kinetic energy transfer from the larger to the smaller mass, in particular during periods when bouncing is out of phase.24 This increases the rate of loading in the bones and joints of the person with a lower weight.24 The generation of high-energy impact is supported by the reporting of open tibial and distal femoral fractures and more dislocations when comparing trampoline centres to home trampolines.5 10 25 Age was another risk factor for injuries in trampoline centres. The greater risk of injuries observed in older children and adolescents in trampoline centres may reflect higher rates of risk-taking behaviours in pre-teens and teenagers.2 17 Children under 6 years of age were less like to be injured in trampoline centres than older children. The reason for this is unclear and may be due to body mass, age limits that restrict use of centres by younger children, advertisements targeting adolescents or greater levels of supervision.
Fewer upper extremity injuries, lacerations and concussions were noticed in trampoline centres. Older home trampolines which are elevated and do not have safety features are still used. It is not uncommon for many children of varying body mass to use home trampolines. All these factors may contribute to these injuries. Upper extremity injuries often result from falls off trampolines, falls being the most common mechanism of injury in the home setting.4 17 Given that trampoline courts are not usually elevated but built below ground level, fewer falls occur in this setting.17 The reduced risk of concussion and lacerations in trampoline centres observed in our study could be explained in part by the use of wall-to-wall gymnastics-grade protective padding to cover exposed structures and spring mechanisms in trampoline centres.7 17 26 Padding does not always mitigate injuries at commercial centres as some users have been injured when their feet were entrapped in protective padding.10 17 Moreover, current requirements for padding and mesh netting surrounds for home trampolines and those at trampoline centres have not reduced injuries.10 This highlights the need for safety improvements above and beyond the design of trampolines, for example, limiting the number of jumpers per trampoline.
Injury surveillance systems in several continents have reported a soaring number of emergency department visits and hospital admissions related to trampoline injuries over time.3 10 27 28 Trampoline injuries cost the US healthcare system $1 billion between 2002 and 2010.29 The global proliferation of commercial trampoline centres after 2011 was associated with a 12-fold increase in emergency visits due to trampoline centre injuries reported by NEISS,10 which will exert additional pressure on limited healthcare budgets. Jordan et al 5 conducted a cost analysis of injuries that occurred in a single commercial trampoline centre in the UK and presented to the Royal Surrey County Hospital emergency department from July 2014 to November 2015. The total acute healthcare cost (including ambulance callout, emergency department, inpatient and outpatient care) for 71 patients was over £80 888 (US$123 637).5 The mean cost per child was £905 (US$1383), ranging from £298 (US$455) to £4158 (US$6356) and per adult was £1274 (US$1947), ranging from £298 (US$455) to £4789 (US$7320).
An Australian study of 392 paediatric trampoline injuries compared injury costs sustained at a trampoline centre versus on home trampolines. The estimated total injury cost in 2015 was $A546 786 (US$410 438) in this cohort (average cost per child $A1395 (US$1047).26 Although only 76 injuries occurred in a trampoline centre, these injuries accounted for 22% of the total cost and required a longer hospital stay.26 Furthermore, 21% of children whose injury was sustained in the trampoline centre were hospitalised and 18% required surgery.26 The non-financial burden of trampoline injuries was also significant. At 6 month follow-up, 33% of patients experienced persistent pain and 32% had some form of physical disability.5 Therefore, prevention of trampoline-related injuries is crucial to diminish both morbidity and the economic burden to society.12
Presently, safety guidelines are not legislated for commercial trampoline centres anywhere in the world.7 13 16 26 Most trampoline centres only demand an user’s injury liability waiver before admission,25 and the current AAP policy statement on trampolines does not include trampoline centres because of the lack of data regarding the safety of these recreational venues.5 7 In response to the growing number of trampoline centres and the high injury rates, stakeholders created the International Association of Trampoline Parks (IATP) in 2012 to develop safety standards for trampoline centres.16 However, adherence to these safety standards is not mandated.16 For instance, the Australian Trampoline Park Association (ATPA), which is a subcommittee of the IATP, notes that fewer than 20% of trampoline centres in Australia are members of the IATP,30 raising concerns about the standards for manufacture, installation, operation and maintenance of trampolines required in these venues and their safety policy.
ATPA safety guidelines for trampoline centres recommend a minimum supervision ratio of one staff for every 20 users and a maximum of one jumper per trampoline.30 However, up to 73% of paediatric trampoline injuries occur despite adult supervision.31 32 Hence, a monitored setting may create a false sense of security and underestimation of risk at trampoline centres.10 Also, trampoline centres frequently request one user per mat, but given the open layout of some venues and the large number of clients this instruction is not always followed and multiple jumpers can end up either unintentionally or purposely on the same trampoline mat.5 The AAP policy discourages backflips and somersaults in the home setting due to reported deaths and spinal cord injuries.6 However, currently many commercial trampoline franchises do not have rules in place against somersaults and backflips.2 13 The mechanisms of injuries sustained at trampoline centres were not reported in most of the studies included in this meta-analysis so we were not able to infer conclusions. Elucidation of injury mechanisms is needed to inform strategies to reduce injuries at trampoline centres.
This study has a number of limitations. Given the nature of any meta-analysis, findings are constrained by the number and quality of included studies. There were few studies which included both injuries at a trampoline centre and at home. Additionally, the definition of some outcomes could not be verified as this information was not provided in primary publications, contributing to the heterogeneity of several meta-analyses. For example, neither ‘upper extremity injuries’ nor ‘surgical interventions’ were specifically defined. Further, most ORs were crude estimates which did not adjust for potential confounders such as age, gender, trampoline size or injury mechanism. No study specifically identified factors which could mitigate harm. Strengths of this study include the use of PRISMA guidelines and the broad search strategy which included multiple databases without language restrictions. Most data were obtained from large national injury databases or hospitals with sizeable catchment areas, avoiding ascertainment bias which limits the generalisability of findings. We only included studies that reported data where the ORs could be calculated.
In conclusion, our findings support the notion that children and adolescents using trampoline centres can sustain more severe trauma with requirement for surgical intervention than children using home trampolines. Considering the rapid global expansion of the commercial trampoline industry in the last decade, the increasing injury rates and the cost to health systems, the development and implementation of evidence-based safety standards and preventative strategies and public awareness campaigns are urgently required. Additionally, we recommend that future studies should attempt to adjust for potential confounding factors.
What is already known on the subjectHome trampoline injuries are well-documented and policy statements have been developed, advising against recreational use.
Trampoline centres have grown in popularity as well as the reported number of injuries occurring in those centres during the last decade.
Little is known about whether injuries sustained at commercial trampoline centres and in the home differ.
What this study addsThis systematic review and meta-analysis showed that injuries sustained at commercial trampoline centres are more severe than home trampoline injuries.
An increased risk of musculoskeletal and/or orthopaedic injuries (particularly lower extremity injuries and sprains) and the need for surgery were found at commercial trampoline centres compared to home trampolines.
The risk of upper extremity injuries, lacerations and concussions was lower at commercial trampoline centres.
Data availability statementAll data relevant to the study are included in the article or uploaded as supplementary information The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics statementsPatient consent for publicationEthics approvalNot applicable.
AcknowledgmentsAPSU activities are supported by The University of Sydney, Faculty of Medicine and Health, Discipline of Child and Adolescent Health; Kids Research at the Sydney Children’s Hospital Network (Westmead); and the Royal Australasian College of Physicians (Division of Paediatrics and Child Health).
留言 (0)