
記住我




The term megarectum describes the radiological or operative finding of a grossly enlarged rectum often with an accompanying varying length of colonic dilatation.1 Such dilatation is observed congenitally in short-segment Hirschsprung’s disease (classic Hirschsprung’s disease is associated with megacolon) and can be acquired with infection (Chagas disease) and some disorders of the endocrine or central nervous system (including spinal trauma and old age).2 However, megarectum can also be observed in the absence of an organic cause and the term ‘idiopathic’ is applied.1 Idiopathic megarectum affects both sexes roughly equally, with symptoms generally starting in early infancy or childhood.3 A high proportion of these patients fail4 or poorly tolerate5 medical and behavioural6 interventions, which do not restore rectal calibre to normal, even following several years of therapy.7 On this basis, despite the relatively high-risk nature of surgery, resection of the enlarged rectum may be undertaken, even in childhood.8
Accepting the rarity of the condition, resected rectal tissue provides an opportunity for review of histopathological findings, which also might determine whether rectal dilatation in idiopathic megarectum occurs as a consequence of a primary neuromuscular disease9–14 of the rectal wall or occurs secondary to functional changes, including behavioural or learning difficulties in which volitional stool retention may lead to chronic distension.3 15–17 To date, pathological studies have been limited to small numbers of patients (largest study: n=24) with heterogeneous clinical presentations and a dependence on a variety of techniques, some of which are now outdated (see the Discussion section for full review of previous studies). The lack of consistency in pathological abnormalities observed to date has prevented firm conclusions regarding whether observed changes are primary or secondary. One further group of patients develop megarectum in association with rare anorectal anomalies.18–20 Wide variations in prevalence are reported in this association (10%–50%), and the mechanism of visceral distension is not fully understood, possibly reflecting a concomitant primary neuromuscular disorder of the rectum or the effect of chronic distal stenosis before or after surgery, or both.21
Here we present the results of a systematic histopathological evaluation of 35 patients undergoing surgical excision of the rectum for megarectum including those considered primary ‘idiopathic’ and those secondary to corrected anorectal malformations. This evaluation is in keeping with international guidance on techniques and reporting of gastrointestinal (GI) neuromuscular pathology.22
ResultsFindings in the whole cohortHistopathological examination of rectal tissue from all 35 patients showed a range of findings (table 3 and figure 1). The most common finding was the presence of extensive fibrosis (30 of 35 patients), with the submucosa most affected (27 of 35 patients). Fibrosis was also evident in the region around the myenteric ganglia and in the muscularis propria in about half of patients with fibrosis. This fibrosis stained red with the EVG method indicating collagen and varied from fine fibrils to thick bands of collagen. The next most common finding was hypertrophy of the muscularis propria (27 of 35 patients), usually involving both muscle layers and always involving the circular muscle layer. In some cases, gross hypertrophy was evident. Where hypertrophy was present, intramuscular fibrosis was also often present.
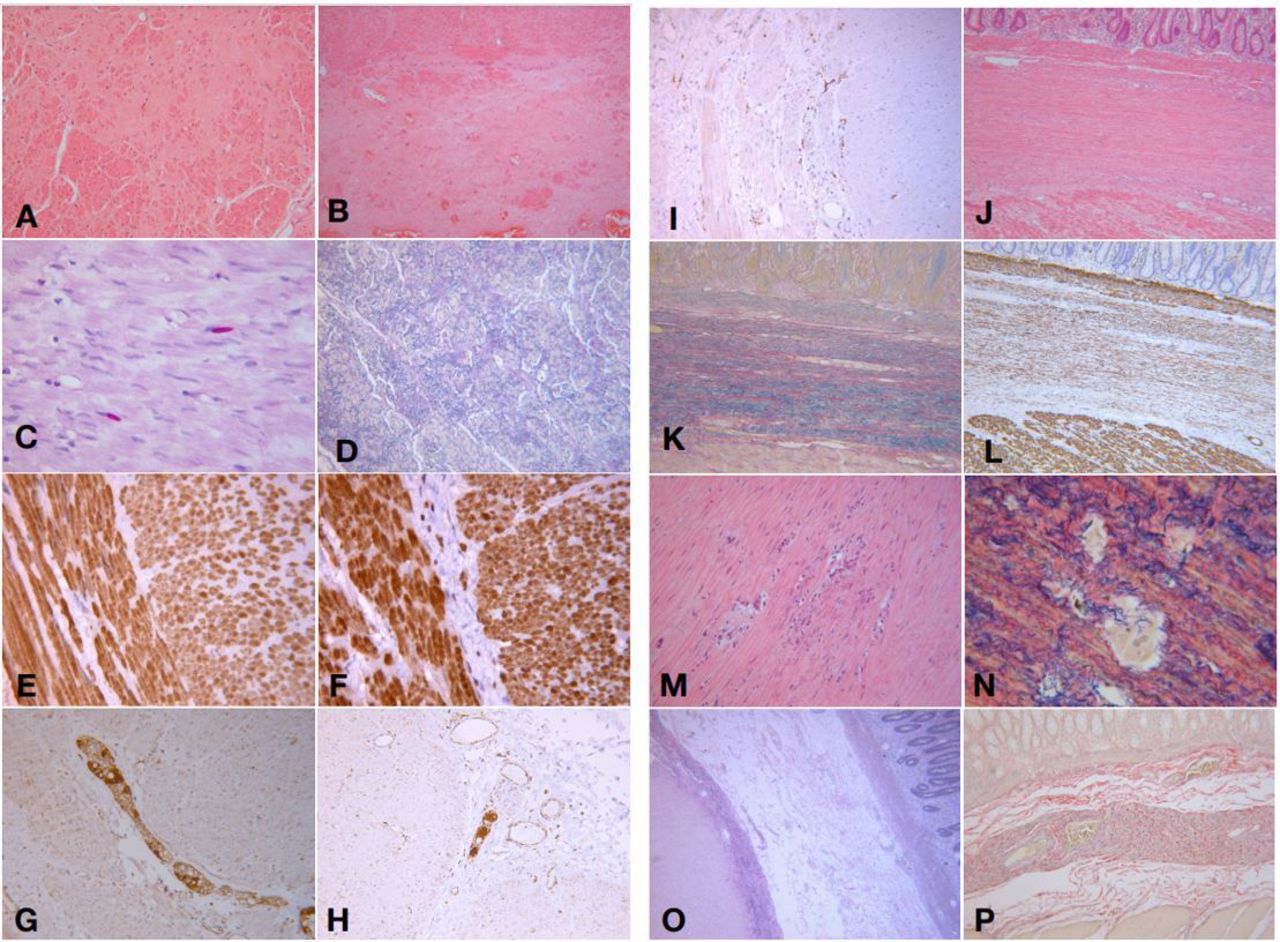 Figure 1
Figure 1 Extensive replacement of the muscularis propria by apparent ‘fibrosis’ (A,B), and in some areas leading to the appearance of a ‘lost layer’ of longitudinal smooth muscle (B) (H&E ×25). (C) Ovoid polyglucosan bodies (purple) within the smooth muscle fibres of the muscularis propria (periodic acid-Schiff stain ×40). (D) Areas of apparent ‘fibrosis’ showing extensive elastosis (stained black) (elastic van Gieson ×25). (E,F) Normal pattern of smooth muscle actin (E) and desmin (F) immunostaining in preserved areas of the smooth muscle of the muscularis propria (x40). (G,H) Normal ganglia of the myenteric (G) and submucosal (F) plexus stained with the MTOCH1 antibody, highlighting ganglion cell bodies (x25). (I) Normal pattern of CD117 immunostaining highlighting interstitial cells of Cajal (x40). (J,K,L) Submucosal smooth muscle metaplasia and fibroelastosis filling the submucosa between the muscularis mucosa and the muscularis propria: H&E section (×25) (J), elastic van Gieson (K) and desmin (L) immunostaining. (M,N) Intramuscular area of abnormal elastin fibres within the hypertrophic circular layer of the muscularis propria: H&E (×25) (M), including a multinucleate giant cell reaction. Elastic van Gieson stain (×40) showing a large multinucleate giant cell (light brown colour) and surrounding coarse elastin fibres (N). (O,P) Defined bands of elastosis within the submucosa, one deep and adjacent to the muscularis propria (O) and the other in the midpoint of the submucosa (P) (elastic van Gieson ×25).
Table 3Pathological findings on examination of full-thickness rectal tissue from all patients with megarectum
EVG staining revealed evidence of elastin deposition in over half of patients (19 of 33 patients). This elastosis was profound in several patients, where it was present in all or nearly all major layers of the rectal wall, and in others it was more focal but with a variable distribution. Elastosis was often accompanied by a degree of fibrosis, but the latter was not always prominent. In some patients the elastin was associated with a granulomatous response, including focally in the mid part of the muscularis propria in one case. In this latter situation the elastin fibres appeared fragmented and coarse only in the area of inflammation (see figure 1M,N), not elsewhere. In the control group, and in those without significant elastin deposition, elastin fibres were seen in the expected distribution in the blood vessel walls, in a fine mesh in the muscularis mucosa and the luminal most aspect of the muscularis propria. Elastin is also normally present in a fine line around the myenteric plexus and in between the muscle fascicula of the muscularis propria (figure 2).
 Figure 2
Figure 2 Normal distribution of elastin in the rectum with elastic van Gieson staining. (A) Mucosa and muscularis mucosa. (B) Submucosa/muscularis propria interface; the asterisk marks the submucosal ganglion. (C) Myenteric plexus at the interface of the circular and longitudinal muscle layers; the asterisk marks the myenteric ganglion. (D) Myenteric plexus (asterisk) and longitudinal muscularis propria junction with serosa.
Polyglucosan bodies, demonstrated on periodic acid-Schiff staining, were evident in the muscularis propria in 15 of 32 patients. Since these can be a patchy finding, multiple sections were examined, demonstrating that in 9 of those 15 patients with polyglucosan bodies these were present in more than one, and sometimes several sections.
Classically described abnormalities of nerve and muscle (enteric neuropathies and myopathies) were rare or absent. Only two patients had evidence of hypoganglionosis and none had a classic degenerative myopathy with or without vacuolation (even by a-smooth muscle actin and desmin immunostaining). In contrast, several patients had evidence of gross morphological changes in the organisation of the nerve plexus and/or muscle. Thus three patients had duplication of the myenteric plexus and three had complete duplication of the circular muscle layer. Eight patients showed smooth muscle metaplasia of the submucosa, often in association with fibrosis or elastosis or both. Reductions in numbers of interstitial cells of Cajal were noted in only 6 of 27 patients. No evidence of amyloid deposition was detected using Congo red staining.
Findings by main groupsThe above findings were common to both groups of patients studied (table 4). Thus, while there were some slight variations in the proportion of patients with each histological finding, there were no major differences, with the exception that duplications of nerve and muscle were confined to the secondary (anorectal malformation) group, perhaps reflecting a parallel developmental abnormality (in addition to evident anorectal malformation).
Table 4Main histological findings by disease group
DiscussionEven taking all causes together, megarectum is acknowledged as a rare cause of severe intractable constipation in children and adults.1 3 6 15 The category generally excludes specific causes such as Hirschsprung’s disease, where the dilatation is consequent on mechanical obstruction caused by the distal narrowed aganglionic segment.
Several case series and case reports on megarectum have described variable changes of all three main final effectors of sensorimotor function (enteric nervous system, smooth muscle and interstitial cells of Cajal).9–14 23 Several report smooth muscle hypertrophy9–11 with or without some degree of fibrosis or connective tissue abnormality.24 Some have also reported changes in neuronal staining,9 10 14 while others have found no abnormality.13 25 Overall, reported changes have been inconsistent. Further, these studies have generally included only relatively small numbers of rectal tissues from patients with defined idiopathic megarectum (most being mixed series of patients with megacolon and megarectum24) and all predate the development of international guidance on techniques and reporting of GI neuromuscular pathology.22 As part of a centralised pathological review of patients with GI neuromuscular disease, we re-evaluated all rectal tissues obtained from patients with idiopathic megarectum with techniques in keeping with this guidance.
The opportunity afforded by our large paediatric surgery practice, in addition to our specialist practice, both surgical and histopathological, in adult GI dysmotility, allowed us to use ‘primary’, that is, idiopathic megarectum, and ‘secondary’ megarectum groups and compare findings for commonalities and differences to gain some insight into the mechanistic processes. In our series we show some similarities but also some major differences in findings to those seen in the classic study of Gattuso et al.10 Our series is larger and includes both idiopathic and secondary megarectum. Hypertrophy of smooth muscle, despite the presence of dilatation, was a common feature of both series, as was fibrosis; however, our series included 85.7% of cases with fibrosis, a higher rate than Gattuso et al,9 and a great deal of elastosis, a feature not commented on in previous studies. We used an EVG preparation in our series, which is a sensitive detector of both collagen and elastin.26 Previous studies have not employed this method, which may explain the lack of previous reporting. It is very easy to confuse elastosis with fibrosis on an H&E preparation (figure 1). Similarly, we report polyglucosan bodies as a common feature of both idiopathic and secondary megarectum. The bodies are easy to miss on a section if you are unaccustomed to recognising them, and the majority of laboratories receiving specimens relating to GI dysmotility do not perform the full range of recommended stains and may well be unfamiliar with identification of inclusion bodies.27 28
The common patterns of pathology seen in both idiopathic and secondary megarectum groups suggest that hypertrophy, fibrosis, elastosis and polyglucosan body formation are common features of rectal dilatation rather than primary causal pathology. While little primary research has been performed on GI smooth muscle, inferences may be drawn from a range of other studies on smooth muscle. Using a wide range of such literature, hypertrophy, fibrosis, elastosis and indeed the formation of polyglucosan bodies seen in the patients reported here may be linked through secondary mechanisms, as depicted in a summary form in figure 3. Stress from stretching is known to cause smooth muscle hypertrophy in airway smooth muscle via inhibition of glycogen synthase kinase 3 beta (GSK3B).29 GSK3B inhibition has also been reported to play a critical role in hypertrophy of cardiac myocytes30 and in human cardiac muscle, leading to increased beta-catenin expression and subsequent protein expression increase and hypertrophy.31
 Figure 3
Figure 3 Proposed model of smooth muscle changes in the megarectum. GSK3B, glycogen synthase kinase 3 beta.
GSK3B is a key enzyme in a range of intracellular processes, not just hypertrophy. GSK3B is normally activated and is the main regulator of glycogen synthase (GS). When GSK3B is inhibited there is an increase in the activity of GS kinase.32 33 A balance of GS and glycogen branching enzyme (GBE) is key to the formation of soluble glycogen. Insoluble deposits of non-branching polyglucosan can be deposited when this balance is disrupted by either a deficiency of GBE or an increase in GS.34 35 It is conceivable that the smooth muscle hypertrophy seen in megarectum is accompanied by an increase in the activity of GS, which might overwhelm the normal balance of glycogen production and predispose to polyglucosan body formation.
When subjected to laminar shear stress vascular smooth muscle cells will deposit tropoelastin in vitro in two-dimensional settings,36 but the recent demonstration of the production of mature elastin fibres and elastogenesis-related proteins by smooth muscle cells in a three-dimensional matrix37 shows that shear stress may produce a functional change in smooth muscle cells that can create the setting for elastogenesis. We have already shown that smooth muscle cells in visceral myopathy may transform into myofibroblastic phenotypes and be associated with the production of collagen,38 and in megarectum it seems highly likely that the same process may be occurring in response to smooth muscle injury. Thus, the stretch and lateral shear produced by rectal dilatation can create conditions that result in smooth muscle hypertrophy, fibrosis, elastogenesis and polyglucosan body formation in keeping with our findings. The commonality of these features in both idiopathic and secondary megarectum provides evidence of these processes as a final common pathway in chronic rectal dilatation.
We acknowledge limitations to the study, which include the small number of overall patients and the general descriptive nature of the methodology. However we note the rarity of the condition (St Mark’s Hospital, London identified only 92 genuine cases in a 27-year period3), making our pathological series the largest published to date. Significantly, the current study adds to a literature devoid of contemporary pathology reporting for this condition. While acknowledging that the above discussion on mechanism is hypothetical, our findings mirror two important clinical observations. First, profound structural changes such as high degrees of fibrosis may account for the irreversibility of gross megarectum necessitating recourse to major surgery,8 and second that earlier stages of the disease, for example, when first recognised, justify the current clinical approach of emptying the rectum (sometimes by manual disimpaction) and thence keeping it empty3 by means such as rectal and oral laxatives, and anterograde and retrograde irrigation.
Take home messagesIn the largest case series reported to date, we have identified characteristic features of the pathology of megarectum not previously reported, including the presence of elastosis and polyglucosan bodies.
The presence of similar features in both primary and secondary megarectum cohorts is highly suggestive of a common, and secondary, cellular process that is potentially preventable and we propose a mechanism for this.
留言 (0)