
記住我


On completion of this activity, the learner will be better able to: • Identify current major areas of unmet need among patients with schizophrenia • Describe the mechanism of action by which TAAR1 agonists control schizophrenia symptoms • Evaluate clinical data on the use of TAAR1 agonists to treat schizophrenia
Among adults in the prime of their lives, schizophrenia is one of the top 25 causes of disease burden around the world.1 Unfortunately, the toolkit we have to fight this disorder remains similar to the one available in the 1950s, when the first antipsychotic was discovered. Today, all antipsychotics work via essentially the same mechanism: by antagonizing the dopamine D2 receptor. Although this mechanism is able to control the positive symptoms of schizophrenia for many patients, substantial unmet needs remain. Studies have shown that schizophrenia is an extremely heterogeneous condition in terms of symptoms,2–4 brain structure and chemistry,5–7 and the genetic and epigenetic variants that confer risk.4,8,9 It is unsurprising that a single class of medications is not effective for all patients and all symptoms.
In fact, antipsychotics fail to control symptoms for approximately one third of patients with schizophrenia.10 In addition, they frequently cause adverse effects that may result in patients abandoning treatment.11 In one trial of nearly 1500 patients with schizophrenia randomized to take various antipsychotics, nearly 75% discontinued the medication that they had been assigned within 18 months because of lack of effectiveness, intolerable adverse effects, or other reasons.12 In the context of this trial, they were offered another antipsychotic; however, in real life, many patients simply stop taking their medication.
Our inability to effectively manage schizophrenia for so many patients has consequences for them, their families, the health care system, and society. Only approximately 14% to 50% of patients with schizophrenia achieve recovery, depending on the definition used.13 Recovery depends on many factors, of which effective medication is just one.14 However, effective medication is an essential tool in controlling the symptoms of this debilitating disorder.
Because of the limitations of our current care options, the life expectancy of patients living with schizophrenia in North America is approximately 14 years shorter than that of the general population.15 One contributor to this much shorter life expectancy is the rate of suicide among patients with schizophrenia, which is 4.5 times the US population average; among patients 18 to 34 years of age, it is a stunning 10 times the population average.16 At a broader level, in 2020, the economic burden of schizophrenia in the United States was estimated to be $281.6 billion annually, reflecting both direct costs (eg, health care, supportive housing, the criminal justice system) and indirect costs (eg, nonemployment, caregiver burden, and caregiver unpaid wages).17 Clearly, new medications are urgently needed.
Recently, promising clinical data have emerged for a novel class of drugs with an entirely new mechanism for treating schizophrenia: the trace amine–associated receptor 1 (TAAR1) agonists. An additional treatment option for schizophrenia could dramatically improve the prospects of patients who cannot achieve recovery with existing antipsychotics. However, clinicians who care for patients with schizophrenia may be skeptical of potential new treatments, for good reason. Promising preclinical data have raised the field's hopes about new agents many times, only for the results of late-stage clinical trials to dash them. Examples of past disappointments are varied, including a glutamate receptor agonist,18 an α-7 nicotinic receptor agonist,19 a phosphodiesterase 10A inhibitor,20 and a glycine reuptake inhibitor.21
Given the strong performance of the TAAR1 agonist ulotaront in a recent phase 2 clinical trial,22–24 as well as the existence of ralmitaront, another TAAR1 agonist being investigated in clinical trials, there is good reason to believe that these novel agents may hold greater promise than previous approaches. Here, we review the biologic, preclinical, and clinical data available for TAAR1 agonists, so that if and when they are approved for the treatment of schizophrenia, psychiatry specialists will be ready to use them to optimize patient outcomes. We also briefly review other emerging therapies in late-stage development for the treatment of schizophrenia.
UNMET NEEDS IN SCHIZOPHRENIA: LIMITATIONS OF CURRENT ANTIPSYCHOTIC MEDICATIONSThe first antipsychotic, chlorpromazine, was introduced in 1952.25 Although antipsychotics revolutionized the treatment of schizophrenia, the limitations of this class of medications were evident as early as the 1960s.25Schizophrenia is a multifaceted disorder that consists of positive, negative, and cognitive symptoms (Fig. 1).26,27 Whereas the intensity of positive symptoms tends to come and go over a patient's life course, negative and cognitive symptoms tend to be ever present (Fig. 2).26,28 Recovery from schizophrenia necessitates control of all 3 types of symptoms. However, available antipsychotics tend to control only positive symptoms.25
 FIGURE 1: Patients with schizophrenia experience 3 core types of symptoms: positive, negative, and cognitive. However, currently available antipsychotics primarily control positive symptoms. Adapted from Correll and Schooler26 (2020) and Bowie and Harvey27 (2006).
FIGURE 1: Patients with schizophrenia experience 3 core types of symptoms: positive, negative, and cognitive. However, currently available antipsychotics primarily control positive symptoms. Adapted from Correll and Schooler26 (2020) and Bowie and Harvey27 (2006). FIGURE 2: Schematic of different types of symptoms over the life course of a typical patient with schizophrenia. Adapted from Correll and Schooler26 (2020) and Millan et al28 (2014).Positive Symptoms
FIGURE 2: Schematic of different types of symptoms over the life course of a typical patient with schizophrenia. Adapted from Correll and Schooler26 (2020) and Millan et al28 (2014).Positive Symptoms
Positive schizophrenia symptoms can be considered an excess or distortion of normal functions.26 Examples include delusions, hallucinations, and disorganized behavior. Although antipsychotics offer substantial relief from positive symptoms for many patients with schizophrenia, up to one third of individuals exhibit treatment resistance, typically defined as the persistence of symptoms despite 2 or more trials of antipsychotics of adequate dose and duration, with documented adherence.10,29
Multiple hypotheses have been proposed to explain why some individuals experience treatment resistance.10,30 One hypothesis is that these patients develop dopamine supersensitivity, caused by the upregulation of dopamine receptors, from past antipsychotic treatment. This supersensitivity would prevent the dopamine receptor blockade by which antipsychotics work. Another hypothesis is that patients with treatment-resistant schizophrenia have normal dopaminergic function, and alterations in other neurotransmitter systems—such as the glutamatergic system—are responsible for their disorder. The dopamine-focused mechanism of action of antipsychotics would not help control symptoms in these patients. Such hypotheses are not mutually exclusive; treatment resistance may be caused by different mechanisms in different patients.10,30
Currently, clozapine is the only evidence-based therapy for treatment-resistant schizophrenia that is approved by the Food and Drug Administration (FDA). Despite its well-established efficacy for managing positive symptoms in treatment-resistant schizophrenia,30 as well as improving quality of life and functioning,31 its association with cardiometabolic, hematologic, and other adverse effects limits its use.25,32 Although research suggests that clozapine can be used safely when dietary, clinical, and therapeutic monitoring is in place,33 it can be challenging for clinicians to provide such monitoring in everyday practice.34 Many healthcare providers also remain wary of using this agent because of the risk of severe adverse effects.34,35 Finally, some patients with treatment-resistant schizophrenia fail to respond to clozapine, or are unwilling to take it.30 As a result, clozapine is underused, although many patients have a favorable experience taking it.36–38 For these reasons, agents with attractive safety profiles that could be used to treat patients who do not respond to existing antipsychotics would represent a major advance for the field.
In addition to failing to control positive symptoms in patients with treatment-resistant schizophrenia, available antipsychotics fail to prevent relapse for a sizable proportion of patients. One study found that 1 in 5 patients with first-episode schizophrenia who initially responded well to antipsychotic treatment experienced breakthrough psychotic symptoms over a 2-year period, even when a long-acting injectable (LAI) antipsychotic was used to ensure adherence.39 Although the breakthrough symptoms tended to be less severe than first-episode symptoms, the patients' treatment response was poorer. Similarly, a meta-analysis of 19 LAI trials found that 1 of 5 patients relapsed over a period of roughly 9 months.40 Among patients who did not initially achieve symptom remission while taking their LAI, this figure was 1 in 3. Because every relapse makes remission harder to achieve,41 failure to prevent relapse has serious ramifications for a patient's life-long disease trajectory.
To treat patients experiencing treatment-resistant schizophrenia or breakthrough symptoms, clinicians may try increasing the dose of their antipsychotic or augmenting it with another antipsychotic.30 Unfortunately, although increasing the dose of an antipsychotic may improve its effectiveness, it also makes a patient more likely to experience a range of adverse effects, including weight gain, parkinsonism, hyperprolactinemia, and neurocognitive impairment.42 Similarly, with regard to treatment-resistant schizophrenia, there is little evidence that 2 antipsychotics are more beneficial than one antipsychotic, and adding another antipsychotic to a patient's treatment plan increases the chance they will experience adverse effects.30,41 Clearly, the limited tools available hamper clinicians' ability to manage patients' positive symptoms.
Negative SymptomsNegative schizophrenia symptoms involve a reduction in or absence of normal behaviors related to motivation, interest, and expression.26 Examples include avolition, anhedonia, asociality, blunted affect, and alogia. Negative symptoms are not typically the reason that patients with schizophrenia receive clinical care, and patients often lack insight into their negative symptoms.26 As a result, it is easy for clinicians to give patients' negative symptoms less attention than their positive symptoms. However, negative symptoms are extremely common and have an outsized impact on patients' lives.
Among patients experiencing a first psychotic episode, 90% experience at least 1 negative symptom.26 Negative symptoms severe enough to require treatment occur in up to 60% of patients with schizophrenia.26 Research shows that negative symptoms are a better predictor of quality of life and functional outcomes than are positive symptoms.43
As mentioned previously, negative symptoms do not respond well to currently available antipsychotics.26 In some cases, clinicians try to address negative symptoms by prescribing antidepressants in addition to antipsychotics. However, the evidence supporting this practice is lacking, and adding another medication makes a patient's regimen more complex—and potentially problematic.41 Therapies that address schizophrenia's negative symptoms are sorely needed.
Cognitive ImpairmentCognitive symptoms of schizophrenia include impaired attention, working memory, verbal fluency, and executive functioning.27 Like negative symptoms, cognitive symptoms are extremely common in schizophrenia, occurring in roughly 80% of patients.44 They too are a better predictor of functional outcomes than positive symptoms.45 In fact, neurocognitive ability has been found to be the best predictor of everyday life skills among patients with schizophrenia.46 Because currently available antipsychotics fail to meaningfully address the cognitive impairment present in schizophrenia, it remains difficult for patients to achieve recovery.
Adverse EffectsThe adverse effects associated with antipsychotics are well known and include weight gain, prolactin elevation, and extrapyramidal symptoms (EPS), among others. Many of these adverse effects are associated with excessive D2 receptor occupancy, so they are directly related to available antipsychotics' mechanisms of action.47 In a recent survey of 200 individuals with schizophrenia who were taking antipsychotics, the adverse effects considered most bothersome were weight gain, sexual dysfunction, and trouble concentrating (Fig. 3).11 Although 92% of patients surveyed said that antipsychotics improved their symptoms, more than one quarter (27%) reported that antipsychotics did more harm than good.
 FIGURE 3: Bothersomeness of the adverse effects of antipsychotics, as rated in a survey of 200 patients with schizophrenia.11Patient Preference and Adherence 2020;14:2043–2054. Originally published by and used with permission from Dove Medical Press Ltd.
FIGURE 3: Bothersomeness of the adverse effects of antipsychotics, as rated in a survey of 200 patients with schizophrenia.11Patient Preference and Adherence 2020;14:2043–2054. Originally published by and used with permission from Dove Medical Press Ltd.Given the prevalence of adverse effects, it is not surprising that many patients stop taking their antipsychotics (Fig. 4).41 In the survey mentioned previously, of the 56% of respondents who reported stopping their medication at some point, 65% reported doing so because of adverse effects.11 The adverse effects that most often led to treatment discontinuation were also among those most frequently rated “extremely bothersome”: feeling like a zombie, feeling drowsy/tired, and weight gain. The single biggest risk factor for relapse in schizophrenia is medication nonadherence, and with every successive relapse, remission becomes harder to achieve.41 The adverse effect profile of current antipsychotics is a major contributor to both treatment discontinuation and failure to achieve remission.
 FIGURE 4: Risks associated with the adverse events caused by antipsychotics. Adapted from Harvey and Kane41 (2021).
FIGURE 4: Risks associated with the adverse events caused by antipsychotics. Adapted from Harvey and Kane41 (2021).Even among patients who are able to take their antipsychotics consistently, concerns about serious adverse effects such as tardive dyskinesia and cardiometabolic disease remain. Indeed, cardiovascular disorder and diabetes are among the leading causes of morbidity and mortality in individuals with schizophrenia48,49 and are major drivers of the lifetime costs associated with the disorder.50
In individuals with schizophrenia, long-term treatment with antipsychotics is associated with lower overall mortality rates than no long-term treatment,14 even from cardiovascular disease.51 This may be because individuals with schizophrenia experience a higher risk of cardiovascular mortality independent of antipsychotic use,52 and antipsychotics improve their ability to manage comorbidities. Comorbidities are quite common; for example, in a study of 404 patients with first-episode psychosis, 57% had dyslipidemia, 15% had prediabetes, 13% had metabolic syndrome, 10% had high blood pressure, 3% had diabetes, and many were overweight and smoked.41 By stabilizing patients' schizophrenia symptoms with medication, clinicians can help lay the foundation for treatment of their other chronic health conditions. However, schizophrenia therapies with a more favorable cardiometabolic profile would further improve patients' health.
Currently, clinicians are limited in their ability to satisfactorily manage antipsychotics' adverse effects. One obvious response to an adverse effect is to reduce the dose of a patient's antipsychotic, especially once their symptoms have been stabilized. However, a recent meta-analysis showed that reducing the dose below the standard range recommended for acute stabilization is associated with an increased risk of relapse and medication discontinuation.53 Relative to a standard dose, a low dose (50%–99% of the standard dose) increases the risk of relapse by 44%, and a very low dose (<50% of the standard dose) increases the risk by 72%. Moreover, in this study, adverse effect outcomes—including intolerability-related discontinuations—differed little among the dose groups. Thus, dose reductions below the standard range do not seem to be a safe or effective way to respond to adverse effects.
Older adults (those 65 years and older) seem to be especially vulnerable to elevated mortality rates and cardiopulmonary arrest when taking antipsychotics.54 As the proportion of older adults in the United States and many other countries rises over time,55 the toll that antipsychotics take on cardiopulmonary health will increase at the population level. This makes the search for new, safer schizophrenia therapies urgent.
RecoveryThe criteria for functional recovery from schizophrenia typically include symptom remission, vocational function, independent living, and meaningful peer relationships for more than 2 years.41 The adverse effect profiles and limited effectiveness of current antipsychotics have contributed to the relatively low percentage of patients who achieve recovery. Long-term treatment for schizophrenia is characterized by recurrent cycles in which antipsychotics are interrupted and then reintroduced, which is not conducive to recovery.56 Patients and clinicians report that the top 2 reasons for discontinuing antipsychotics are lack of effectiveness and adverse effects.57 Even in Finland, where issues of insurance coverage and treatment access are less problematic than in the United States, participants in a national cohort study experienced a median of 6 treatment interruptions during 8 years of follow-up.56 More effective, tolerable, and safe treatment options could help increase the proportion of patients with schizophrenia who are able to achieve recovery.
THE NEW BIOLOGY OF TAAR1 AGONISTS: EMERGING AGENTS FOR THE TREATMENT OF SCHIZOPHRENIASchizophrenia is a multifaceted disorder that affects multiple interconnected brain pathways, including the dopaminergic, glutamatergic, and serotoninergic systems.58 Despite the nuanced neurobiology underlying schizophrenia, as well as the wide spectrum of symptoms, available antipsychotics work almost exclusively by antagonizing D2 receptors, which results in dopamine blockade.59 Many atypical antipsychotics also possess serotonin 5-hydroxytryptamine 2A receptor (5-HT2A) activity.59
The limited effectiveness of current antipsychotics suggests that some cases of schizophrenia are caused by dysfunction outside the D2 dopaminergic system.60 It is notable that some patients with treatment-resistant schizophrenia respond to clozapine, which is unique among typical antipsychotics for its affinity for the D4 dopamine receptor, as well as its action at serotonergic, noradrenergic, and glutamatergic receptors.61,62 Given the inability of currently available antipsychotics to control symptoms for many patients with schizophrenia, agents with entirely novel mechanisms of action are likely required, especially to control negative and cognitive symptoms.
Trace amine–associated receptor 1 agonists have emerged as a novel class of potential schizophrenia therapies. Trace amine–associated receptor 1 is a G-protein–coupled receptor expressed in various dopamine-rich regions of the brain that are associated with schizophrenia (Fig. 5.)63,64 Initial evidence suggests both intracellular and membrane localization for TAAR1.64 Preclinical data show that TAAR1 affects central nervous system function and behavior, possibly through its influence on the monoamine system, which encompasses dopamine, noradrenaline, and serotonin signaling; it also has effects on the glutamatergic system.64 Trace amine–associated receptor 1 seems to act as an internal rheostat, maintaining neurotransmission within healthy physiologic limits.65 Specifically, it is believed to function in regulating reward circuits, cognitive processes, mood states, glucose levels, and body weight,65 all of which are disrupted in schizophrenia.
 FIGURE 5: Key regions of TAAR1 expression in the brain that are associated with schizophrenia pathophysiology. Trace amine–associated receptor 1 is found in dopamine-rich regions, such as the ventral tegmental area and substantia nigra, and serotonin-rich regions, such as the dorsal raphe nucleus. Adapted from Nair et al63 (2022).
FIGURE 5: Key regions of TAAR1 expression in the brain that are associated with schizophrenia pathophysiology. Trace amine–associated receptor 1 is found in dopamine-rich regions, such as the ventral tegmental area and substantia nigra, and serotonin-rich regions, such as the dorsal raphe nucleus. Adapted from Nair et al63 (2022).The rationale for investigating TAAR1 agonists as schizophrenia therapies is supported by several lines of evidence. First, by activating TAAR1, TAAR1 agonists seem to modulate the signaling of multiple neurotransmitter systems, including the dopaminergic, serotonergic, and glutamatergic systems, that are dysregulated in schizophrenia.59,64,66 Second, genetic variants in the TAAR genes, including TAAR1, have been linked to schizophrenia.67 This suggests that targeting TAAR1 could modify the symptoms of schizophrenia. Finally, agents that do not block postsynaptic D2 receptors are unlikely to contribute to the development of important adverse effects associated with current antipsychotics, such as hyperprolactinemia and EPS.68
Although TAAR1 agonists do not directly antagonize D2 receptors, as current antipsychotics do, they do act at multiple points in the dopaminergic signaling system. Preclinical research shows that when bound by an agonist, TAAR1 forms heterodimers with D2 dopamine receptors on presynaptic and postsynaptic neurons, altering the way that these receptors function (Fig. 6).64,69,70 Dopamine efflux then occurs through the D2 receptors, reducing dopamine levels within presynaptic neurons.71 Simultaneously, dopamine transporters are internalized, decreasing dopamine uptake and the rate at which dopaminergic neurons fire.64,69,71 This action of TAAR1 agonists at the presynaptic level represents a novel approach to managing schizophrenia, given that current antipsychotics function primarily at the postsynaptic level by blocking dopamine receptors from binding dopamine released into the synaptic cleft.
 FIGURE 6: Effects of TAAR1 on the dopaminergic system. Figure reprinted from Rutigliano et al64 (2018, CC-BY 4.0).
FIGURE 6: Effects of TAAR1 on the dopaminergic system. Figure reprinted from Rutigliano et al64 (2018, CC-BY 4.0).Trace amine–associated receptor 1 agonists do more than alter dopamine release by presynaptic neurons. They also decrease postsynaptic dopamine activity via the β-arrestin-2–dependent Akt/glycogen synthase kinase-3 pathway (Fig. 6).69 This pathway governs dopamine-mediated behaviors and is implicated in schizophrenia.69 Furthermore, TAAR1 agonists reduce the firing of serotonergic neurons and increase transmission through glutamatergic neurons66—all potentially important processes for controlling schizophrenia symptoms.
Ulotaront (SEP-363856)Ulotaront is a TAAR1 agonist with serotonin 5-HT1A agonist activity, and it is the first TAAR1 agonist to enter phase 3 trials. As such, it has been granted breakthrough therapy designation by the FDA.72
PharmacologyUlotaront was discovered during a screen for agents that lacked D2 or serotonin 5-HT2A antagonist activity while demonstrating an antipsychotic-like profile in vivo.59 Specifically, researchers used SmartCube, an artificial intelligence–based phenotypic discovery platform, to identify ulotaront.59,73 In the SmartCube system, after an agent is administered to a mouse, supervised machine learning algorithms assess the animal's phenotype, including locomotion, trajectory complexity, body posture and shape, and behaviors. On the basis of this automated assessment, the agent being studied is assigned a label, such as antipsychotic or antidepressant, based on the similarity of its profile to that of known drugs. This high-throughput approach allows investigators to efficiently screen large compound libraries.
In this case, screening a compound library with the SmartCube system showed a dose-dependent relationship between ulotaront treatment and antipsychotic activity in mice (Fig. 7).59 Ulotaront also showed modest antidepressant properties. Next, receptor panel screening and functional tests showed that this agent is a TAAR1 and serotonin 5-HT1A agonist. Subsequent experiments in mice, rats, and monkeys demonstrated that orally administered ulotaront has good systemic bioavailability and high brain penetrance. Finally, follow-up experiments in mice showed that ulotaront exhibits antipsychotic- and antidepressant-like activity without inducing catalepsy, indicating low potential for causing EPS in humans. These preclinical findings set the stage for studies in humans.
 FIGURE 7: Screening a compound library in mice revealed that ulotaront exhibits dose-dependent antipsychotic properties, as well as antidepressant activity, despite lacking D2 and serotonin 5-HT2A antagonist activity. ADHD, attention-deficit/hyperactivity disorder. Adapted from Dedic et al59 (2019) with permission from American Society for Pharmacology and Experimental Therapeutics.Clinical Trial Data
FIGURE 7: Screening a compound library in mice revealed that ulotaront exhibits dose-dependent antipsychotic properties, as well as antidepressant activity, despite lacking D2 and serotonin 5-HT2A antagonist activity. ADHD, attention-deficit/hyperactivity disorder. Adapted from Dedic et al59 (2019) with permission from American Society for Pharmacology and Experimental Therapeutics.Clinical Trial Data
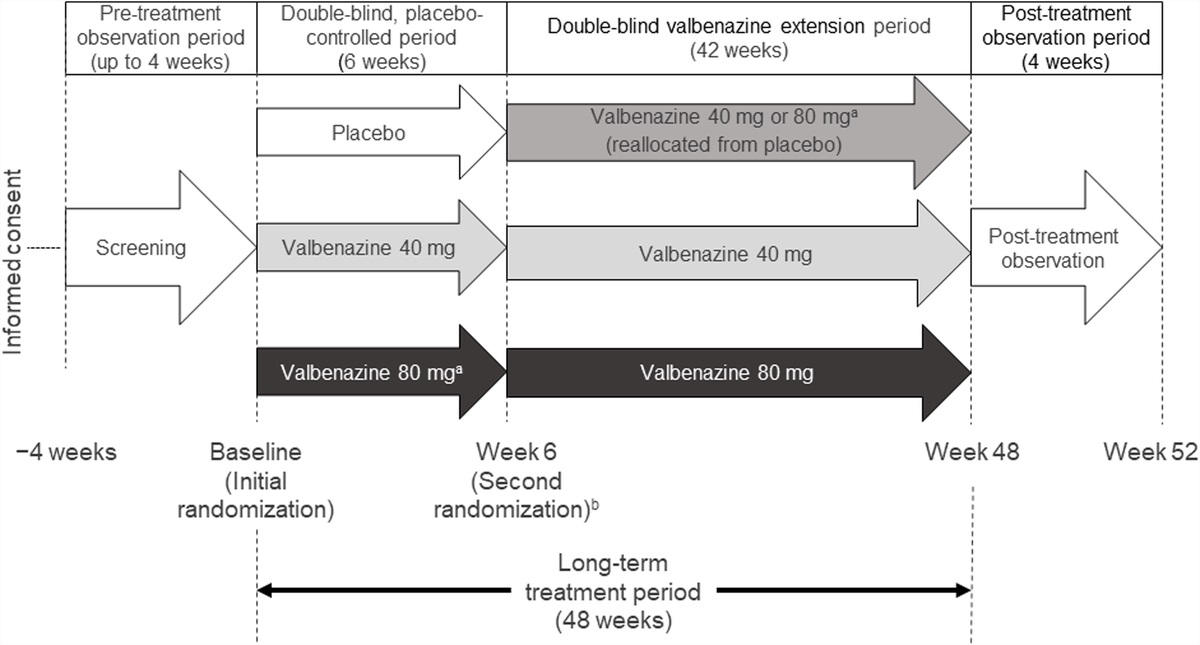
Findings from a 4-week phase 2 randomized trial comparing ulotaront to placebo in acutely ill patients with schizophrenia have been reported,22 as well as the results of a 26-week open-label extension of this trial.23 A total of 193 patients completed the 4-week trial, of whom 157 continued in the extension study.23Figure 8 shows how these studies were designed.22,23
 FIGURE 8: Study design for the 4-week phase 2 trial comparing ulotaront to placebo in acutely ill patients with schizophrenia, as well as its 26-week extension study. Adapted from Koblan et al22 (2020) and Correll et al23 (2021).
FIGURE 8: Study design for the 4-week phase 2 trial comparing ulotaront to placebo in acutely ill patients with schizophrenia, as well as its 26-week extension study. Adapted from Koblan et al22 (2020) and Correll et al23 (2021).With regard to efficacy, ulotaront was found to have a medium effect size (0.45, P = 0.001) on the Positive and Negative Syndrome Scale (PANSS), with improvement seen for both positive and negative symptoms (Table 1).22 Further improvement in symptoms was documented in the extension study, as measured by both PANSS score and Clinical Global Impressions Scale–severity, including for cognitive symptoms (Fig. 9).23,24 The extension study also confirmed the effect of ulotaront on negative symptoms: significant improvements from baseline were noted using the PANSS negative subscale, Brief Negative Symptom Scale (BNSS) total score, and uncorrelated PANSS score matrix Negative Apathy/Avolition Factor and Negative-Deficit of Expression Factor scores.23
TABLE 1 - Efficacy of Ulotaront vs Placebo* in a 4-Week, Phase 2 Randomized Trial Conducted in Acutely Ill Patients with Schizophrenia22 Efficacy Measure Least-Square Mean Change From Baseline at Week 4 Least-Square Mean Difference (95% CI) Ulotaront 50 or 75 mg Placebo Primary end point PANSS total score −17.2 ± 1.7 −9.7 ± 1.6 −7.5 (−11.9 to −3.0) Secondary end points† CGI-S score −1.0 ± 0.1 −0.5 ± 0.1 −0.05 (−0.7 to −0.2) PANSS positive subscale score −5.5 ± 0.5 −3.9 ± 0.5 −1.7 (−3.1 to −0.3) PANSS negative subscale score −3.1 ± 0.4 −1.6 ± 0.4 −1.5 (2.6 to −0.4) PANSS general psychopathology subscale score −9.0 ± 0.9 −4.7 ± 0.8 −4.3 (−6.6 to −2.0) BNSS total score −7.1 ± 1.0 −2.7 ± 0.9 −4.3 (−6.8 to −1.8) MADRS total score −3.3 ± 0.6 −1.6 ± 0.6 −1.8 (−3.2 to −0.3)Adapted from New England Journal of Medicine 2020;382(16):1497–1506. Originally published by and used with permission from the Massachusetts Medical Society.
*Mean change from baseline ± standard error.
†No inferences can be made for the secondary end points because the study did not include a plan to control for multiple comparisons.
CGI-S, Clinical Global Impressions Scale-Severity; MADRS, Montgomery-Åsberg Depression Rating Scale.
 FIGURE 9: Mean change in positive and negative schizophrenia symptoms during 4 weeks of double-blind treatment with ulotaront or placebo (left portion of plots) and 26 weeks of open-label treatment with ulotaront (right portion). A, Change in PANSS total score. B, Change in PANSS subscale scores: negative, positive, and general. DB, double blind; OL, open label; PBO, placebo; ULOT, ulotaront. Adapted from Correll et al23 (2021, CC-BY 4.0).
FIGURE 9: Mean change in positive and negative schizophrenia symptoms during 4 weeks of double-blind treatment with ulotaront or placebo (left portion of plots) and 26 weeks of open-label treatment with ulotaront (right portion). A, Change in PANSS total score. B, Change in PANSS subscale scores: negative, positive, and general. DB, double blind; OL, open label; PBO, placebo; ULOT, ulotaront. Adapted from Correll et al23 (2021, CC-BY 4.0).With regard to safety, the incidence of adverse events in the 4-week trial was roughly the same for the ulotaront and placebo groups.22 The most common adverse events associated with ulotaront were somnolence, agitation, nausea, diarrhea, and dyspepsia. In both the 4-week trial and 26-week extension study, no significant changes in metabolic laboratory parameters or prolactin levels were found in participants taking ulotaront.22,23 Whereas modest weight gain was documented in the ulotaront group in the 4-week trial, modest weight loss (-0.3 kg) was observed in the extension study. The incidence of EPS in the 4-week trial was similar between the ulotaront and placebo groups (3.3% and 3.2%, respectively),22 and it remained low (3.2%) in the extension study.23 Finally, prolactin levels decreased slightly in both the ulotaront and placebo groups in the 4-week trial, for both men and women,22 and only 4 cases of increased prolactin (an incidence of 2.6%) were documented in the extension study.23
These safety data are compelling. In a comparison of randomized controlled trials, the cumulative rate of adverse events was substantially lower for ulotaront than for available antipsychotics: 23% for ulotaront versus 42% to 60% for lurasidone, quetiapine, and olanzapine.74 To further compare the safety profiles of these agents, researchers analyzed real-world data from the US FDA Adverse Event Reporting System to identify which types of class-related adverse events are disproportionately associated with 30 atypical and typical antipsychotics. They then used clinical trial data for ulotaront and the 3 comparison atypical antipsychotics to plot the proportion of participants who experienced each type of adverse event disproportionately associated with antipsychotics. For many key adverse events associated with antipsychotics, including weight gain, diabetes, elevated fasting glucose, extrapyramidal disorder, and tardive dyskinesia, ulotaront had a superior profile (Fig. 10).74
 FIGURE 10: Comparison of adverse event frequency in clinical trials of ulotaront and 3 atypical antipsychotics. Cumulative percentage of individuals with schizophrenia who experienced an adverse event (y-axis) is shown in relation to disproportional reporting of that adverse event in postmarketing pharmacovigilance data reported via the US FDA Adverse Event Reporting System. Preferred terms were ranked by disproportionality analysis using the Empirical Bayes Geometric Mean (EBGM). The insets show the cumulative percentage of individuals with adverse events of 3-fold or greater disproportional reporting (left) and the EGBM50 for individual studies (below). Adapted from Hopkins et al74 (2021, CC-NC 4.0).
FIGURE 10: Comparison of adverse event frequency in clinical trials of ulotaront and 3 atypical antipsychotics. Cumulative percentage of individuals with schizophrenia who experienced an adverse event (y-axis) is shown in relation to disproportional reporting of that adverse event in postmarketing pharmacovigilance data reported via the US FDA Adverse Event Reporting System. Preferred terms were ranked by disproportionality analysis using the Empirical Bayes Geometric Mean (EBGM). The insets show the cumulative percentage of individuals with adverse events of 3-fold or greater disproportional reporting (left) and the EGBM50 for individual studies (below). Adapted from Hopkins et al74 (2021, CC-NC 4.0).Ulotaront is currently being investigated in the DIAMOND program, a collection of 4 clinical studies conducted in patients with schizophrenia. This program consists of a 6-week phase 3 placebo-controlled trial of ulotaront in adult patients with acute psychosis (NCT04092686),75 a 6-week phase 3 placebo-controlled trial of ulotaront in adult and adolescent patients with acute psychosis (NCT04072354),76 an open-label extension study for participants in either 6-week trial, and a 57-week phase 3 trial comparing ulotaront to quetiapine in adults with schizophrenia (NCT04115319).
留言 (0)