
記住我

Tardive dyskinesia (TD) is a persistent and often debilitating involuntary movement disorder that affects the face, mouth, trunk, limbs, and/or extremities, and can lead to serious outcomes.1–4 The vesicular monoamine transporter 2 (VMAT2) inhibitors comprise a new drug class that includes valbenazine and deutetrabenazine, which are the only promising therapies for TD at this time.5–10 The safety and efficacy of VMAT2 inhibitors for treatment of TD have been demonstrated in numerous clinical trials, and both valbenazine and deutetrabenazine were approved in the United States for this indication in 2017.11 Valbenazine has also been approved for treatment of TD in several Asian countries, including Japan, Singapore, Thailand, Indonesia, South Korea, and Malaysia.12
Tardive dyskinesia is associated with prolonged exposure to dopamine receptor-blocking agents (DRBAs), for example, antipsychotics, and is known to be associated with treatment-resistant schizophrenia and relapse.13,14 Furthermore, underlying bipolar disorder/depressive disorder is known to be a risk factor for TD.15–17 Patients with TD may vary considerably with respect to DRBA treatment regimens prescribed to manage their underlying psychiatric condition18–20; therefore, the efficacy or safety of valbenazine for TD may differ by underlying psychiatric disease. Thus, a subgroup analysis of data from the KINECT 3 trial was performed to confirm the efficacy of valbenazine in patients with schizophrenia/schizoaffective disorder or bipolar disorder/depressive disorder,21,22 and an integrated analysis of data from KINECT 2 and KINECT 3 confirmed the efficacy and tolerability of valbenazine in patients with bipolar disorder/depressive disorder.9
However, the efficacy and safety of valbenazine by underlying psychiatric disease have not yet been clarified in an Asian population, as the KINECT 223 and KINECT 35 studies were conducted in North America, and a majority of patients recruited were not of Asian ethnicity. J-KINECT, a multicenter, phase II/III, randomized, double-blind, placebo-controlled, parallel-group, fixed-dose study,24 demonstrated that valbenazine can be used effectively and safely to treat Japanese patients with TD, including those with underlying schizophrenia/schizoaffective disorder or bipolar disorder/depressive disorder.24 The present study, which is a post hoc analysis of data from J-KINECT,24 was therefore conducted to investigate whether the efficacy or safety of once-daily 40- or 80-mg oral valbenazine for the treatment of TD in Japanese patients differs according to the underlying psychiatric disease: schizophrenia/schizoaffective disorder or bipolar disorder/depressive disorder.
PATIENTS AND METHODS Study Design and Patient PopulationThe full study design and primary analysis of the J-KINECT study have been previously published.24 In brief, J-KINECT was a multicenter, phase II/III, randomized, double-blind, placebo-controlled, parallel-group, fixed-dose study, which was conducted in Japan in national hospitals and outpatient private clinics. The study consisted of a pretreatment observation period of up to 4 weeks (screening period); a double-blind, placebo-controlled period of 6 weeks; a double-blind, 42-week valbenazine extension period; and finally, a 4-week posttreatment observation period. The trial design is illustrated in Figure 1. Briefly, patients were randomly assigned (1:1:1 ratio) to receive either placebo, or 40 or 80 mg of valbenazine, and stratified according to underlying schizophrenia/schizoaffective disorder or bipolar disorder/depressive disorder. At the end of the 6-week placebo-controlled period, patients who received placebo were reallocated in a 1:1 ratio to receive either 40- or 80-mg valbenazine; patients who received valbenazine during the initial 6-week period continued at the same dose.
 FIGURE 1: Study design. aPatients allocated to the 80-mg dose initiated valbenazine at a daily dose of 40 mg for 7 days before titrating up to 80 mg. bFor the valbenazine extension period, patients who received 40- or 80-mg valbenazine during the placebo-controlled period continued at the same dose. Patients who received placebo during the placebo-controlled period were randomly reallocated to either 40- or 80-mg valbenazine for the valbenazine extension period. Reproduced from Horiguchi et al.24
FIGURE 1: Study design. aPatients allocated to the 80-mg dose initiated valbenazine at a daily dose of 40 mg for 7 days before titrating up to 80 mg. bFor the valbenazine extension period, patients who received 40- or 80-mg valbenazine during the placebo-controlled period continued at the same dose. Patients who received placebo during the placebo-controlled period were randomly reallocated to either 40- or 80-mg valbenazine for the valbenazine extension period. Reproduced from Horiguchi et al.24J-KINECT recruited men and women, aged 20 to 85 years, with a diagnosis of schizophrenia, schizoaffective disorder, bipolar disorder, or major depressive disorder, who had also been diagnosed with moderate to severe TD.24 Patients with comorbidities such as other movement disorders or those at high risk of suicidal or self-injurious behavior were excluded. Before initiating the screening period, all patients provided written informed consent to participate after procedures, and possible adverse events were explained to them.
The present study was a post hoc analysis of data from J-KINECT, aiming to assess whether the patients' underlying psychiatric disease influenced the efficacy or safety of valbenazine for treatment of TD. However, the partial efficacy findings and safety findings presented here were a prespecified analysis in J-KINECT and were not part of the post hoc analysis.
The original protocol was approved by the relevant institutional review boards for each study center, and the post hoc analysis was reviewed and approved by the Institutional Review Board of Mitsubishi Tanabe Pharma Corporation. The J-KINECT study was registered at ClinicalTrials.gov under the identifier NCT03176771.
Outcome MeasuresThe efficacy endpoints for the post hoc analysis were as follows: change from baseline in Abnormal Involuntary Movement Scale (AIMS) total score (items 1–7: central assessment based on video recordings) at weeks 2, 4, 6, 16, 32, 48, and 52 after treatment with valbenazine, and Clinical Global Impression of Change–Tardive Dyskinesia (CGI-TD) scores at weeks 6, 48, and 52 after administration of valbenazine.
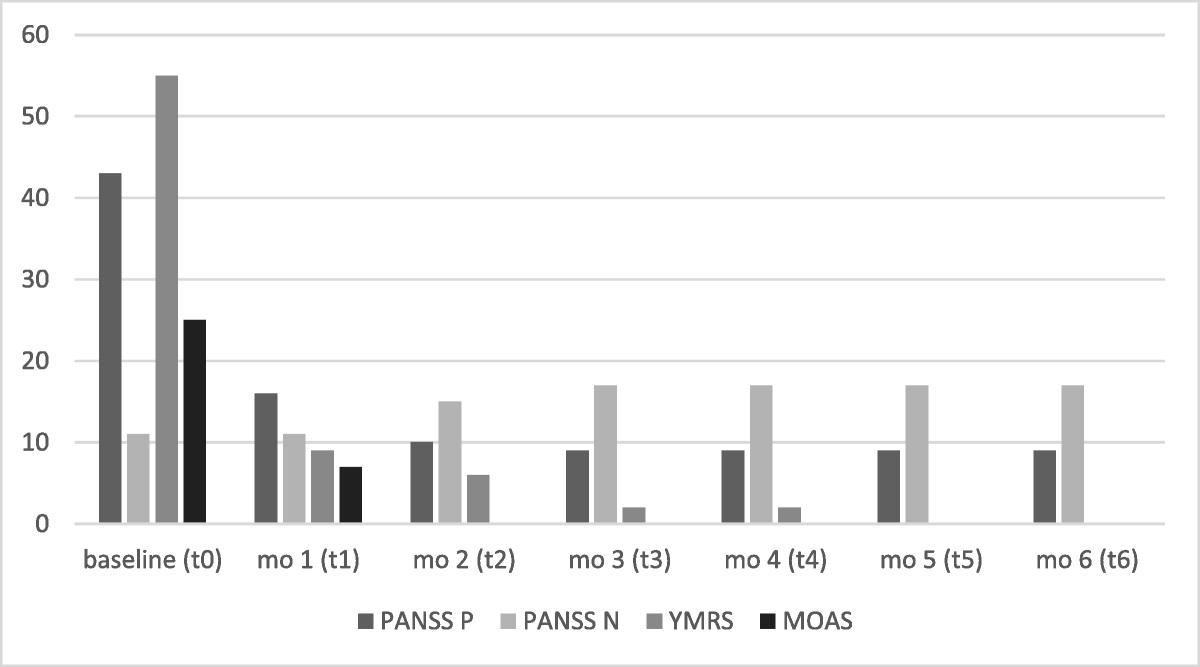
The safety endpoints included the following: treatment-emergent adverse events (TEAEs), related TEAEs (events that were possibly or definitely related to the study drug as assessed by the investigator), the Japanese version of the Calgary Depression Scale for Schizophrenics (JCDSS), the Positive and Negative Syndrome Scale (PANSS) for patients with schizophrenia/schizoaffective disorder, the Japanese version of the Montgomery-Asberg Depression Rating Scale (MADRS-J), and the Young Mania Rating Scale (YMRS) for patients with bipolar disorder/depressive disorder.
Statistical AnalysisBecause this was a secondary use study of data from the J-KINECT study, a formal sample size calculation was not performed. The safety analysis set included all patients who received at least 1 dose of the study drug and had available postbaseline safety data. The intention-to-treat (ITT) analysis set, which was used for the efficacy analyses, included all patients in the safety analysis set who had available baseline and at least 1 postbaseline AIMS total score (by central assessment). The number and proportion of patients, and their major demographic characteristics and baseline disease characteristics were tabulated for each treatment group in the ITT and safety analysis sets, organized by underlying disease. Descriptive statistics were calculated for continuous data. In the ITT analysis set, the number and proportion of patients using concomitant psychotropic medications were tabulated by underlying disease.
An analysis of variance was performed for the change from baseline in AIMS total score at week 6, with treatment group and underlying disease as fixed effects, and treatment group and underlying disease as interactions. The P value for the interaction term between treatment group and underlying disease was calculated. A significance level of 0.2 was used.
The means of the changes from baseline in AIMS total scores at week 6 of treatment were calculated, as well as mean differences between treatment groups (40 and 80 mg) and placebo (including SEs of the mean and 95% confidence intervals [CIs]), grouped by underlying disease.
Descriptive statistics for the changes from baseline in the AIMS total score at weeks 2, 4, 6, 16, 32, 48, and 52 were calculated by treatment group and underlying disease. Descriptive statistics were also calculated for the CGI-TD scores at weeks 6, 48, and 52 by treatment group and underlying disease.
The incidence of TEAEs was tabulated by underlying disease. Treatment-emergent adverse events were coded using the Medical Dictionary for Regulatory Activities version 23.0 and tabulated according to System Organ Class and Preferred Term. Descriptive statistics of measured values and the changes from baseline were calculated for the JCDSS, PANSS, MADRS-J, and YMRS at each assessment point for each treatment group by underlying disease.
Because this study with a post hoc analysis did not have a case-size design, no tests for validity were performed, and the assessments were based on precision (calculation of 95% CIs for the means). All statistical analyses were conducted using SAS software version 9.4 (SAS Institute Inc, Cary, North Carolina).
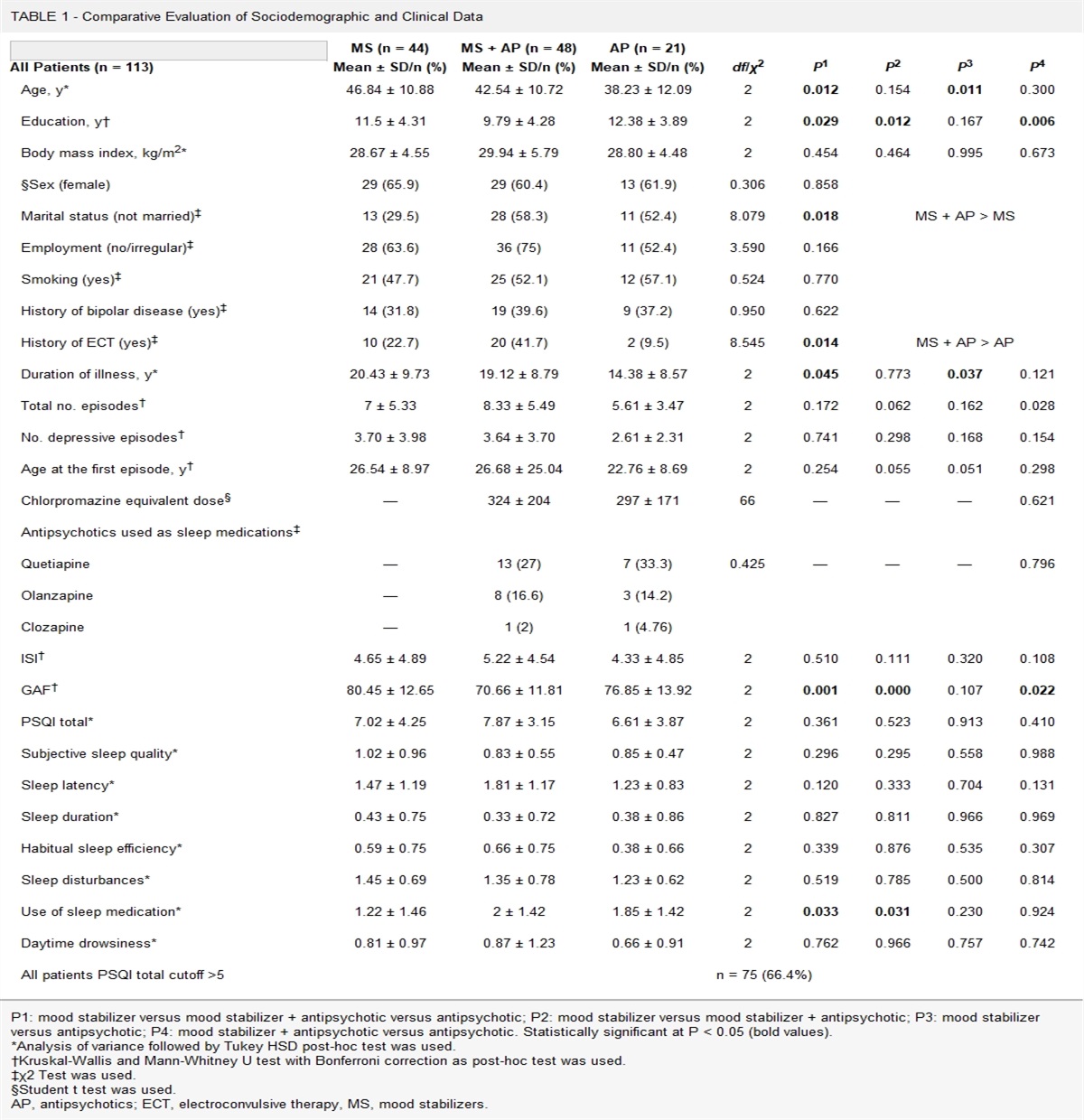
RESULTS ParticipantsThe patient disposition has been previously published.24 In brief, 680 patients provided informed consent, of whom 86, 85, and 85 met all inclusion criteria and were randomly allocated to the valbenazine 40-mg group, valbenazine 80-mg group, and placebo group, respectively. The patients with underlying schizophrenia/schizoaffective disorder in the ITT analysis set comprised 65.1% (54 of 83) of the valbenazine 40-mg group, 64.6% (53 of 82) of the valbenazine 80-mg group, and 63.1% (53 of 84) of the placebo group. The proportions of patients with underlying bipolar disorder/depressive disorder were 34.9% (29 of 83), 35.4% (29 of 82), and 36.9% (31 of 84), respectively. The respective proportions of patients in the safety analysis set were similar. The baseline demographic and clinical characteristics of patients by underlying disease in the ITT analysis set are described in Table 1.
TABLE 1 - Baseline Demographic and Clinical Characteristics (ITT Analysis Set) Schizophrenia/Schizoaffective Disorder Bipolar Disorder/Depressive Disorder Placebo (n = 53) Valbenazine Placebo (n = 31) Valbenazine 40 mg (n = 54) 80 mg (n = 53) 40 mg (n = 29) 80 mg (n = 29) Age, y 59.5 ± 13.2 57.5 ± 13.6 56.3 ± 13.6 60.9 ± 14.0 60.4 ± 14.8 60.7 ± 13.4 Sex, male 26 (49.1) 25 (46.3) 33 (62.3) 10 (32.3) 13 (44.8) 17 (58.6) Body mass index, kg/m2 23.70 ± 3.91 24.36 ± 4.28 23.96 ± 4.18 23.85 ± 3.73 21.62 ± 2.68 23.80 ± 4.34 Duration of TD, y <2 34 (64.2) 21 (38.9) 19 (35.8) 14 (45.2) 14 (48.3) 14 (48.3) ≥2 19 (35.8) 33 (61.1) 34 (64.2) 17 (54.8) 15 (51.7) 15 (51.7) Use of antipsychotics Yes 49 (92.5) 50 (92.6) 50 (94.3) 18 (58.1) 9 (31.0) 13 (44.8) No 4 (7.5) 4 (7.4) 3 (5.7) 13 (41.9) 20 (69.0) 16 (55.2) No. antipsychotics 1 34 (64.2) 30 (55.6) 30 (56.6) 15 (48.4) 7 (24.1) 12 (41.4) 2 14 (26.4) 15 (27.8) 20 (37.7) 3 (9.7) 1 (3.4) 1 (3.4) ≥3 1 (1.9) 5 (9.3) 0 (0.0) 0 (0.0) 1 (3.4) 0 (0.0) Atypical vs typical antipsychotics SGAs only 45 (84.9) 40 (74.1) 37 (69.8) 12 (38.7) 7 (24.1) 11 (37.9) FGAs only or both FGAs and SGAs 4 (7.5) 10 (18.5) 13 (24.5) 6 (19.4) 2 (6.9) 2 (6.9) Chlorpromazine equivalent <600 mg 34 (64.2) 38 (70.4) 33 (62.3) 17 (54.8) 7 (24.1) 10 (34.5) ≥600 mg 15 (28.3) 12 (22.2) 17 (32.1) 1 (3.2) 2 (6.9) 3 (10.3) Use of anticholinergic medication Yes 23 (43.4) 23 (42.6) 29 (54.7) 10 (32.3) 13 (44.8) 8 (27.6) No 30 (56.6) 31 (57.4) 24 (45.3) 21 (67.7) 16 (55.2) 21 (72.4) History of suicidal ideation or suicide attempt Yes 13 (24.5) 17 (31.5) 20 (37.7) 19 (61.3) 15 (51.7) 17 (58.6) No 40 (75.5) 37 (68.5) 33 (62.3) 12 (38.7) 14 (48.3) 12 (41.4) History of suicidality within 3 mo before screening Yes 3 (5.7) 3 (5.6) 2 (3.8) 1 (3.2) 5 (17.2) 4 (13.8) No 50 (94.3) 51 (94.4) 51 (96.2) 30 (96.8) 24 (82.8) 25 (86.2) AIMS dyskinesia total score (central assessment) 8.4 ± 4.4 7.0 ± 3.7 6.8 ± 4.4 7.5 ± 4.0 9.1 ± 3.8 8.6 ± 4.0Data are mean ± SD or n (%).
FGAs, first-generation antipsychotics; SGAs, second-generation antipsychotics.
For patients with schizophrenia/schizoaffective disorder, the mean age at the time of informed consent varied from 56 to 60 years in the valbenazine 40-mg, valbenazine 80-mg, and placebo groups. For patients with bipolar disorder/depressive disorder, the mean age at the time of informed consent was approximately 60 years in these groups.
In terms of baseline disease characteristics, the proportion of patients with a history of suicidal ideation or suicide attempt was higher in patients with bipolar disorder/depressive disorder (51.7%, 58.6%, and 61.3%, in the valbenazine 40-mg group, valbenazine 80-mg group, and placebo group, respectively) than in those with schizophrenia/schizoaffective disorder (31.5%, 37.7%, and 24.5%, respectively). Furthermore, the proportion of patients taking antipsychotics was higher in the schizophrenia/schizoaffective disorder group than in the bipolar disorder/depressive disorder group. The psychotropic medications taken at baseline by ≥2% of patients with either underlying disease are listed in Supplemental Digital Content 1, https://links.lww.com/JCP/A899. Finally, the mean ± SD baseline AIMS total scores based on the central assessment were higher in the placebo group (8.4 ± 4.4) than in the valbenazine 40-mg (7.0 ± 3.7) and 80-mg (6.8 ± 4.4) groups for patients with schizophrenia/schizoaffective disorder and higher in the valbenazine 40-mg (9.1 ± 3.8) and 80-mg (8.6 ± 4.0) groups than in the placebo group (7.5 ± 4.0) for patients with bipolar disorder/depressive disorder (Table 1). There were no other notable differences in baseline demographic and clinical characteristics between groups by underlying disease.
Efficacy OutcomesThe changes in AIMS total scores over time, organized by treatment group and underlying disease, are shown in Figure 2. For patients with schizophrenia/schizoaffective disorder, the mean changes from baseline in the AIMS total score at week 6 (95% CI) were −1.8 (−3.2 to −0.5) and −3.3 (−4.7 to −1.9) in the valbenazine 40- and 80-mg groups, respectively, and −2.4 (−3.9 to −0.9) and −3.5 (−5.1 to −1.9) in the valbenazine 40- and 80-mg groups, respectively, for patients with bipolar disorder/depressive disorder. Regardless of the underlying disease, both valbenazine groups showed improvement compared with placebo. There was no interaction between treatment group and underlying disease (P = 0.876). The AIMS total score during the valbenazine extension period remained lower than that at baseline (continued improvement in score) until week 48, confirming that long-term treatment also sustained the effect, regardless of the underlying disease.
 FIGURE 2:
FIGURE 2: Change from baseline in AIMS total score (central assessment; ITT analysis set). Patients from the placebo group were reallocated to the valbenazine 40- or 80-mg group at week 6. Data are mean ± SE.
The mean ± SE changes from baseline in the AIMS total score at week 52 (schizophrenia/schizoaffective disorder group: 40 mg, −0.3 ± 0.5; 80 mg, −0.7 ± 0.7; bipolar disorder/depressive disorder group: 40 mg, −1.1 ± 0.9; 80 mg, 0.0 ± 1.3) were comparable to baseline in both valbenazine groups, confirming that the treatment effect was attenuated after completion of treatment, regardless of the underlying disease.
The mean CGI-TD scores by treatment group and according to underlying disease are shown in Figure 3A (schizophrenia/schizoaffective disorder) and Figure 3B (bipolar disorder/depressive disorder). As with the AIMS scores, similar results were found regardless of the underlying disease. The mean ± SE CGI-TD scores for patients with schizophrenia/schizoaffective disorder at week 6 in the placebo group were 3.4 ± 0.1. The mean ± SE CGI-TD scores for patients with schizophrenia/schizoaffective disorder at weeks 6, 48, and 52 in the valbenazine 40-mg group were 3.0 ± 0.2, 2.5 ± 0.2, and 3.5 ± 0.2, respectively. The corresponding scores in the valbenazine 80-mg group were 2.7 ± 0.2, 2.3 ± 0.2, and 3.2 ± 0.2. The mean ± SE CGI-TD score for patients with bipolar disorder/depressive disorder at week 6 in the placebo group was 3.4 ± 0.1. The mean ± SE CGI-TD scores for patients with bipolar disorder/depressive disorder at weeks 6, 48, and 52 in the valbenazine 40-mg group were 3.1 ± 0.2, 2.2 ± 0.2, and 3.2 ± 0.2, respectively. The corresponding scores in the valbenazine 80-mg group were 2.9 ± 0.3, 2.4 ± 0.3, and 3.4 ± 0.3.
 FIGURE 3:
FIGURE 3: CGI-TD scores in (A) patients with schizophrenia/schizoaffective disorder and (B) bipolar disorder/depressive disorder (ITT analysis set). Data are mean ± SE.
Safety OutcomesThe incidences of TEAEs and related TEAEs by seriousness, and those related to discontinuation or dose reduction are listed in Table 2. During the placebo-controlled period, the incidences of TEAEs in patients with schizophrenia/schizoaffective disorder were 63.6% (35 of 55), 83.3% (45 of 54), and 37.7% (20 of 53), for the valbenazine 40-mg group, valbenazine 80-mg group, and placebo group, respectively. Among patients with bipolar disorder/depressive disorder, the incidences were 63.3% (19 of 30), 73.3% (22 of 30), and 54.8% (17 of 31), respectively. The incidences of related TEAEs in patients with schizophrenia/schizoaffective disorder were 30.9% (17 of 55), 59.3% (32 of 54), and 9.4% (5 of 53), for the valbenazine 40-mg group, valbenazine 80-mg group, and placebo group, respectively. In patients with bipolar disorder/depressive disorder, the corresponding incidences were 36.7% (11 of 30), 46.7% (14 of 30), and 19.4% (6 of 31). During the long-term treatment period, the incidences of TEAEs in the valbenazine 40- and 80-mg groups were 91.5% (75 of 82) and 94.9% (75 of 79), respectively, for patients with schizophrenia/schizoaffective disorder, and 86.4% (38 of 44) and 93.2% (41 of 44), respectively, for patients with bipolar disorder/depressive disorder. The incidence of TEAEs and related TEAEs was higher in each valbenazine group compared with the placebo group, and higher in the 80-mg group compared with the 40-mg group, for both underlying diseases, with similar trends in TEAEs and related TEAEs.
TABLE 2 - Summary of TEAEs and Related TEAEs (Safety Analysis Set) Placebo-Controlled Period Schizophrenia/Schizoaffective Disorder Bipolar Disorder/Depressive Disorder PlaceboCommon TEAEs (occurring at a frequency of ≥2% during the placebo-controlled period or ≥5% during the long-term treatment period in valbenazine groups with either underlying disease) are described in Table 3. Somnolence was the most common TEAE; the incidences during the placebo-controlled period were 19.3% (21 of 109) and 16.7% (10 of 60) in patients who received valbenazine with schizophrenia/schizoaffective disorder and bipolar disorder/depressive disorder, respectively. The respective incidences of somnolence in the placebo groups were 1.9% (1 of 53) and 3.2% (1 of 31); during the long-term treatment period, the incidences of somnolence were 19.3% (31 of 161) and 18.2% (16 of 88) in the schizophrenia/schizoaffective disorder and bipolar disorder/depressive disorder groups, respectively. During the placebo-controlled period, “schizophrenia (worsening)” occurred in patients with schizophrenia/schizoaffective disorder, but not in patients with bipolar disorder/depressive disorder. Furthermore, “depression (worsening)” and “bipolar disorder (worsening)” occurred in patients with bipolar disorder/depressive disorder, but not in patients with schizophrenia/schizoaffective disorder. During the long-term treatment period, patients with schizophrenia/schizoaffective disorder had a higher incidence of schizophrenia (worsening), and patients with bipolar disorder/depressive disorder had a higher incidence of depression (worsening).
TABLE 3 - TEAEs Occurring at a Frequency of ≥2% in the Placebo-Controlled Period or ≥5% in the Long-Term Treatment Period in Either Valbenazine Total Group (Safety Analysis Set) Placebo-Controlled Period Schizophrenia/Schizoaffective Disorder Bipolar Disorder/Depressive Disorder Placebo
留言 (0)