
記住我



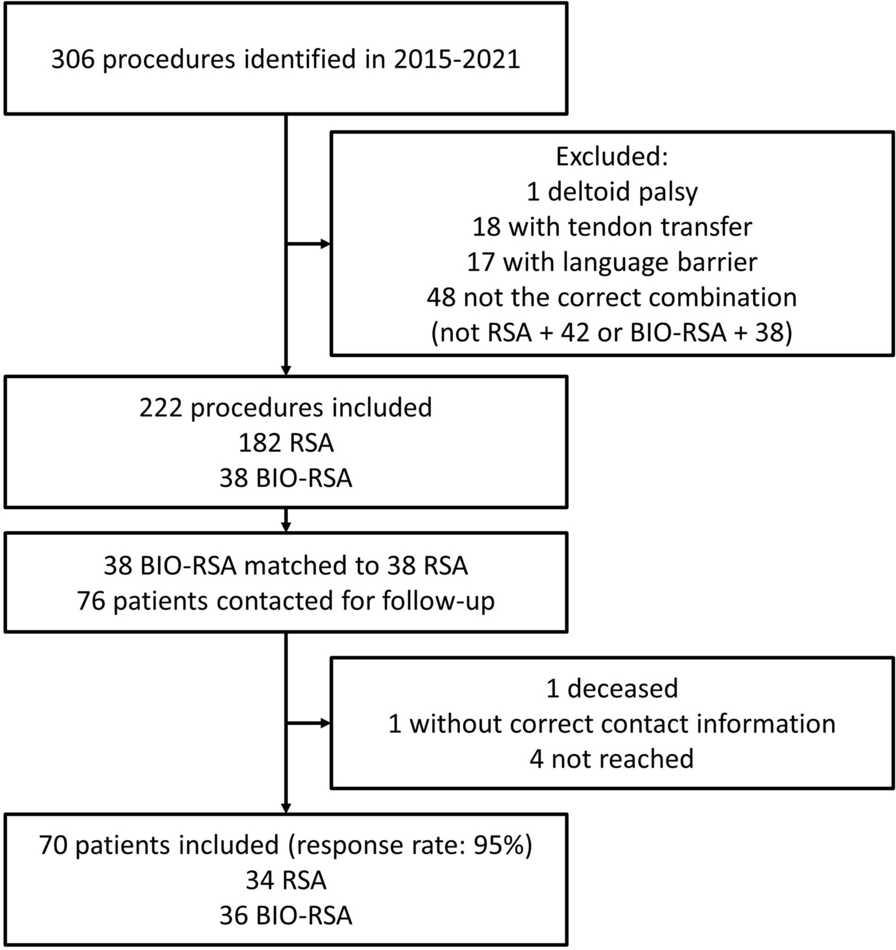





Ninety consecutive patients who underwent THA between 2016 and 2017 at a single, urban, high-volume university hospital were initially enrolled in the prospective comparative study. Five cases were subsequently excluded owing to incomplete information available, resulting in 90 patients with either unilateral (n = 85) or bilateral (n = 10) THA at a single institution with a total of 95 implanted THAs eligible for analysis. Eighty-four THAs were performed for primary coxarthrosis (88.4%). In addition, six cases of mild developmental dysplasia of the hip (6.3%), four post-traumatic coxarthroses (4.2%) and one avascular necrosis (1.1%) were also included in the current study.
Outpatient care included functional examination, and imaging was done using plain radiographs. Pre-operatively, X-rays in two planes and a low-dose CT scan were conducted, followed by a post-operative X-ray, 6 weeks, 3 months, 6 months and 1 year after surgery. After that, outpatient care was conducted annually. The pre-operative low-dose CT was done for 3D templating. All the X-rays and CT scans were performed using the same devices with the patient in a standardized (supine) position. Demographic data (age at time of surgery, gender, BMI), duration of surgery, and pre- and post-operative radiographic measurements of hip geometry were collected.
THA was performed in all patients using a new cementless short stem system (ANA.NOVA Proxy, ImplanTec GmbH, Mödling, Austria) and ceramic-on-ceramic head and liners. On the basis of X-ray and CT scans, the sizes of the implant components (i.e. cup and stem) were planned pre-operatively with both software systems (MediCAD 2D and 3D software). All operations were performed by a single consultant surgeon with an anterolateral approach to the hip with the patient in a supine position.
The study procedure followed accepted ethical, scientific and medical standards and was conducted in compliance with recognized international standards, including the principles of the Declaration of Helsinki. Informed consent was obtained from all the participants, and the study protocol was approved by the local ethics committee (28–152 ex 15/16) and a current amendment (received on 21 April 2020).
Pre-operative digital templatingThe MediCAD software system (mediCAD, Hectec GmbH, Altdorf, Germany) was used for pre-operative digital 2D and 3D templating, incorporating essential parameters such as femoral segmentation, acetabulum diameter, hip joint centre, femoral neck axis, femoral stem axis and leg length difference. The pre-operative measurements were carried out independently of the definitively used implants and the surgeon performing surgery.
Statistical analysisStatistical analyses were carried out using Stata/SE 15.1 (StataCorp, College Station, TX, USA). Mean values and medians were given with the corresponding standard deviation (SD) or interquartile range (IQR). Differences between 2D- and 3D-planned implants and used implants were compared with a paired t-test to calculate the significance. The absolute differences (i.e. positive values only) from 2D- and 3D-planned to definitive implants were calculated for each component (i.e. cup, stem). By reapplying paired t-tests, the absolute differences between 2D- and 3D-planned to definitive implants were estimated. Assuming that overlaying soft tissues may impair calibration of the X-rays for the 2D-based pre-operative planning owing to incoherent scattering, the correlation between BMI and the absolute difference of 2D- and 3D-based measurements compared with the definitive implant was estimated with regression analyses. They were performed to assess: (1) any potential association between BMI and Dorr types, (2) the accuracy of 2D- versus 3D-planned implants and (3) any potential improvements in the accuracy of 2D or 3D templating within the period covered by the study. Additionally, a multivariate linear regression analysis was calculated to evaluate 2D versus 3D templating accuracy in relation to the Dorr type. A two-sided p-value < 0.05 was considered statistically significant.
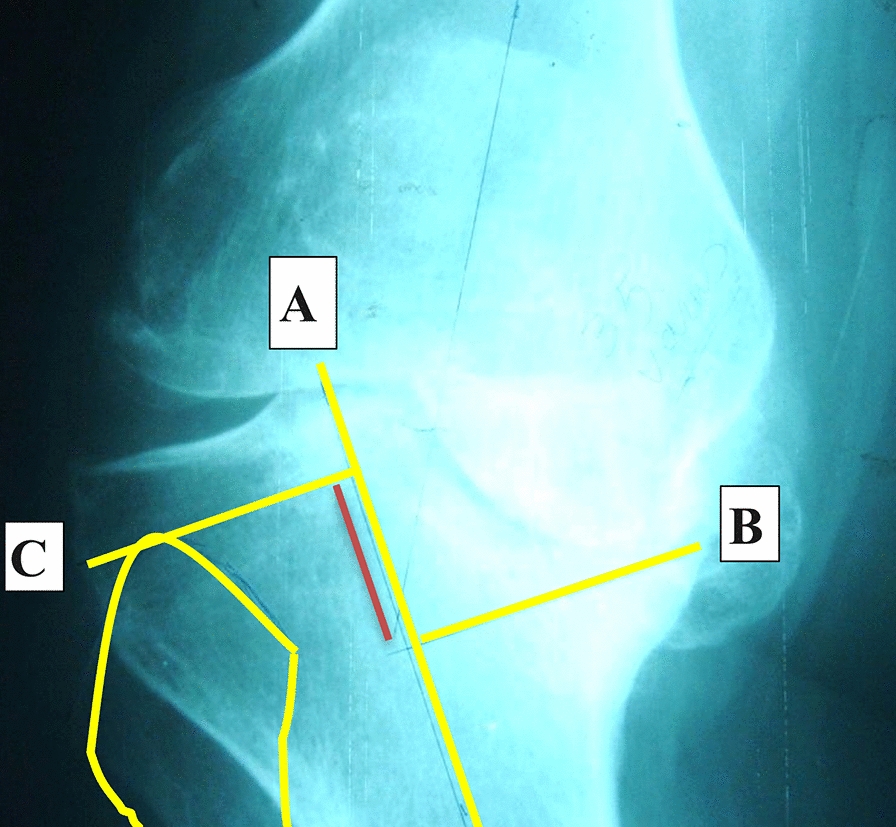
Described by Dorr et al. [28], the three morphological patterns of the femur were named A, B and C (Fig. 1). Dorr types were assessed as follows: type A with a funnel shape and narrow diaphyseal canal; type B exhibits proximal bone loss and widening of the diaphyseal canal; type C with an extensive medullary canal and blurred appearance to the bone cortex due to cortical thinning. The Dorr classification was chosen as it allows quantification of bone quality and anatomy at the proximal femur. Furthermore, depending on Dorr type, the implant itself may be positioned slightly differently and at varying size.
Fig. 1
Morphological types described by Dorr
留言 (0)